
Figure 1.
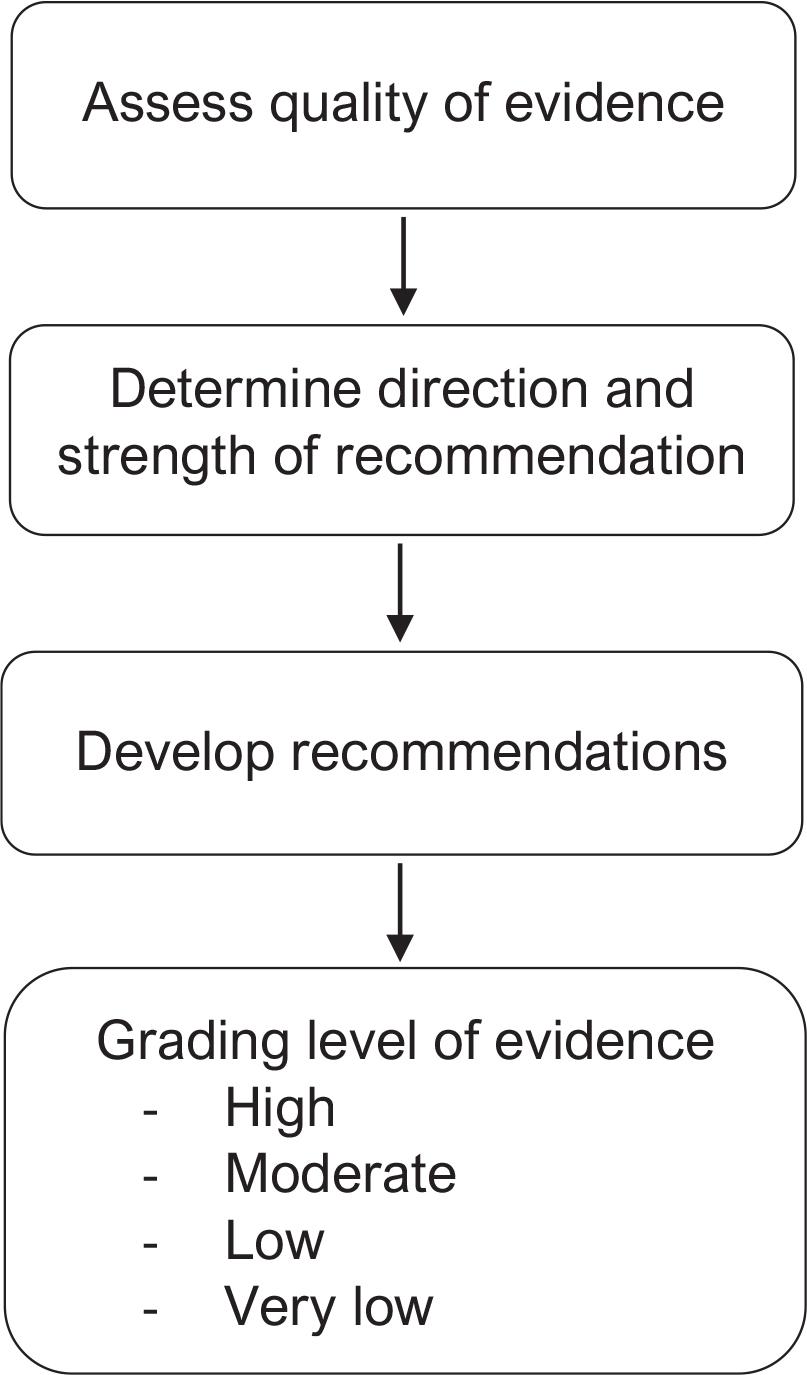
Figure 2.
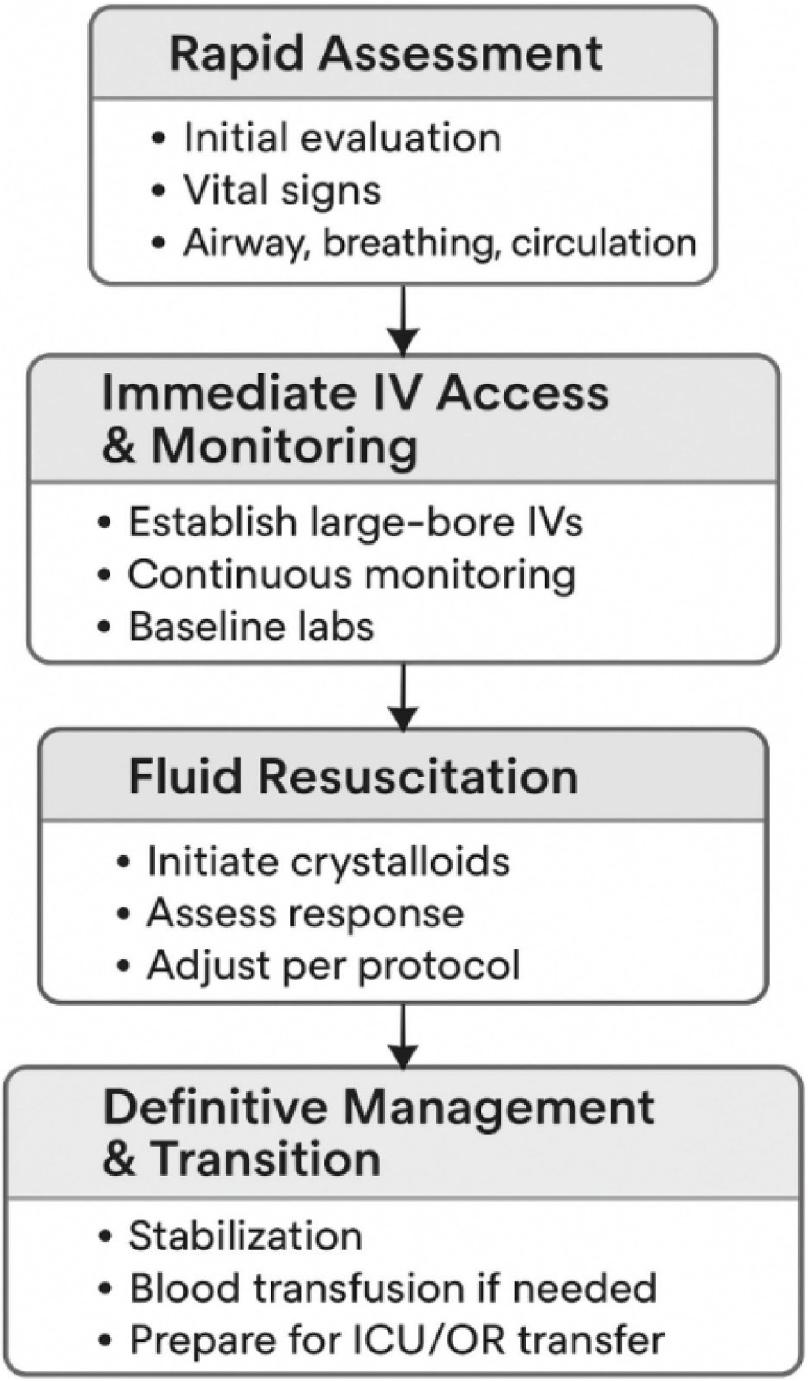
Figure 3.
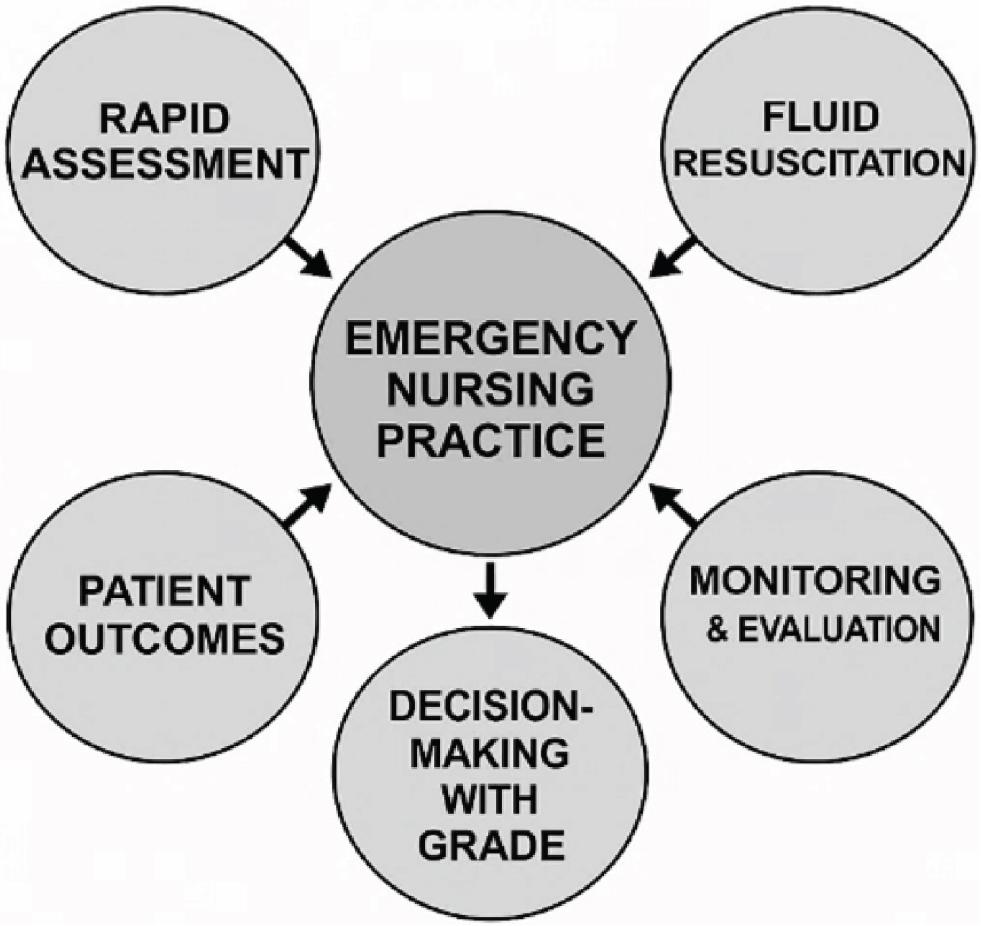
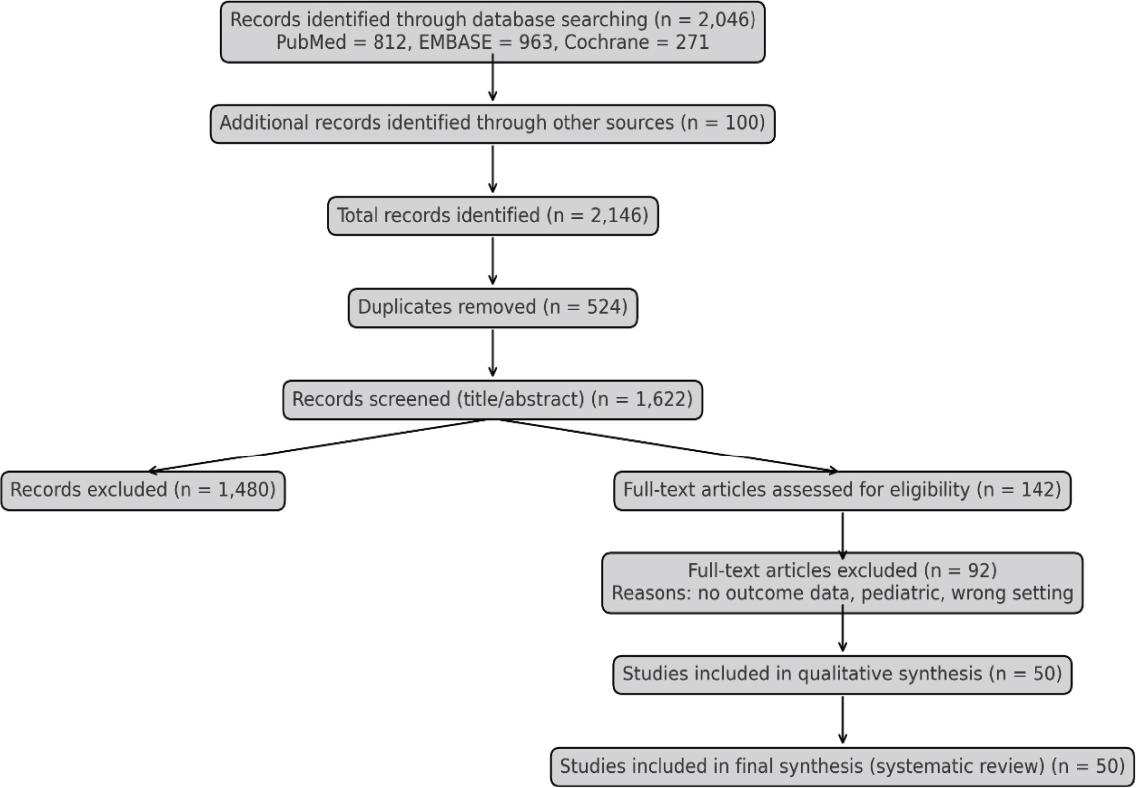
Figure 4.
Importance of the GRADE system in emergency nursing practice [33]
| Aspect | Description | Impact on nursing practice |
|---|---|---|
| Evidence-based decision making | GRADE categorises evidence quality (high, moderate, low, and very low). | Helps nurses choose interventions based on strong clinical evidence. |
| Rapid emergency response | Provides clear, actionable recommendations (strong vs. weak). | Supports fast and accurate decisions in time-sensitive situations. |
| Clinical confidence & autonomy | Promotes understanding of the rationale behind clinical guidelines. | Empowers nurses to act confidently and advocate for best practices. |
| Standardised care delivery | Ensures consistency in interventions across settings and among practitioners. | Reduces variability and enhances patient safety and outcomes. |
| Patient-centred risk assessment | Weighs benefits, harms, patient values, and resource use in decision-making. | Enables personalised and safe care plans for individual patients. |
| Guideline development | Used in global frameworks, like WHO, NICE, and speciality societies. | Involves nurses in developing/updating local evidence-based protocols. |
Practice variation by health care setting
| Setting type | Crystalloid use (%) | Protocol-based care | Nurse training level | GRADE-adherent practice |
|---|---|---|---|---|
| High-income urban | 95 | High | Advanced | Yes |
| Middle-income tertiary | 84 | Moderate | Intermediate | Partial |
| Rural/low-eresource | 72 | Low | Basic | Minimal |
Timing of initial fluid resuscitation and associated clinical trends
| Timing of first fluid administration | Consistency across studies | Reported clinical trend | Narrative interpretation |
|---|---|---|---|
| <30 min | High | Improved survival and perfusion | Early nursing action is critical |
| 30-60 min | Moderate | Intermediate outcomes | Delay may reduce effectiveness |
| >60 min | High | Increased complications and mortality | Clinically undesirable delay |
Qualitative comparison of fluid types and reported clinical outcomes
| Fluid type | Consistency of evidence | Reported outcome direction | Safety profile (narrative) | Clinical interpretation |
|---|---|---|---|---|
| NS | High | Haemodynamic stabilisation | Risk of hyperchloremic acidosis with large volumes | Effective first-line crystalloid; monitoring required |
| LR/balanced crystalloids | Moderate-high | Comparable or improved metabolic outcomes | Lower risk of acidosis | Preferred when large volumes anticipated |
| Colloids (e.g. starches and gelatins) | Moderate | No survival advantage | Increased renal and cost-related risks | Not recommended as first-line therapy |
| Blood products (trauma-specific) | High (trauma) | Improved survival when bleeding is controlled | Requires protocolised use | Adjunct in haemorrhagic shock, not volume replacement |
Nurse-led interventions and their qualitative impact on emergency care outcomes
| Nurse-led intervention | Frequency reported | Observed impact on care | Contribution to evidence synthesis |
|---|---|---|---|
| Early large-bore IV access | Very common | Reduced time to resuscitation | Core nursing responsibility |
| Structured triage protocols (e.g. ESI) | Common | Faster shock recognition | Improves prioritisation |
| Continuous vital sign monitoring | Universal | Early detection of deterioration | Central to reassessment |
| Urine output tracking | Common | Guides fluid titration | Supports goal-directed therapy |
| GRADE-informed checklists | Limited but growing | Improved protocol adherence | Promising implementation strategy |
Characteristics of included studies contributing to the narrative evidence synthesis
| Author (Year) | Country | Study design | Population/context | Sample size | Emergency setting | Key contribution to narrative synthesis |
|---|---|---|---|---|---|---|
| Shrestha et al. (2018) | USA | RCT | Adult trauma with hemorrhagic shock | 320 | Urban ED | Compared crystalloids vs colloids; informed safety and renal outcomes |
| Lin et al. (2020) | China | Cohort | Surgical emergency hypovolemia | 150 | Tertiary ED | Observational evidence supporting early crystalloid use |
| Bampoe et al. (2017) | UK | RCT | Trauma patients | 210 | Trauma centre | Demonstrated benefit of earlier fluid initiation |
| Self et al. (2018) | USA | RCT | Mixed ED shock patients | 280 | Urban ED | Highlighted metabolic effects of saline vs balanced crystalloids |
| Shah et al. (2018) | Egypt | Cross-sectional | Mixed hypovolemic ED patients | 200 | General hospital | Assessed nursing assessment accuracy and fluid practice |
| Brohi et al. (2019) | Spain | RCT | ED patients | 180 | Urban ED | Evaluated nurse-led bolus titration protocols |
| Singh et al. (2016) | India | RCT | Dehydrated adults | 120 | Rural ED | Supported the feasibility of LR in low-resource EDs |
| Guyette et al. (2017) | Spain | Systematic review | Multiple etiologies | — | Multicenter | Synthesised comparative fluid outcomes for narrative integration |
Grade assessment criteria
| Clinical question | Evidence quality | Strength of recommendation | Justification |
|---|---|---|---|
| Crystalloids vs. colloids | High | Strong | Multiple RCTs Myburgh et al. [30], Perel et al. [31], and Lewis et al. [33] show no survival advantage with colloids and a higher risk of acute kidney injury. |
| Early fluid administration (<30 min) vs. delayed | Moderate | Strong | Evidence from cohort studies (Lee et al., 2017) and RCTs demonstrates reduced mortality with earlier fluid initiation, though heterogeneity across patient populations exists. |
| Nurse-led protocols | Moderate | Conditional | Moderate-quality evidence (Patel et al., 2018) supports improved IV access times and monitoring, but effectiveness depends on training and context. |
| Fluid volume per bolus | Low | Conditional | Evidence is limited and inconsistent (de Lange et al. [27], Lu et al. [28]) indicating the need for further trials to determine optimal bolus size. |