
Weight faltering is a significant concern in child health, as it can progress to more severe conditions such as wasting, stunting, and underweight, which are key indicators of malnutrition.1 According to the World Health Organization (WHO), wasting is defined as low weight-for-height (Z-score <-2 standard deviation [SD]), indicating acute malnutrition caused by inadequate nutrient intake or disease. Stunting refers to low height-for-age (Z-score <-2 SD), reflecting chronic malnutrition that can impair cognitive and physical development. Meanwhile, underweight is characterized by low weight-for-age (Z-score <-2 SD), resulting from either acute or chronic malnutrition.2
Weight faltering refers to insufficient weight gain over time, where a child’s weight falls below the expected minimum monthly weight gain.3,4 While various definitions of weight faltering exist, a recent consensus document suggests considering weight faltering when there is a drop of 1 Z-score in weight-for-age over time, based on the WHO growth standards.5,6 This condition is an early indicator of growth disorders and should be closely monitored to prevent the child from progressing underweight, wasting, or stunting.7
Globally, child malnutrition remains a leading cause of morbidity and mortality, accounting for 45% of deaths in children under 5.1,8 In the United States, the estimated prevalence of children with nutrition-related issues, such as weight faltering, exceeds 10%, with higher rates among children in low-income households, those with special healthcare needs, and low birth weight children.1
In low- and middle-income countries, malnutrition in young children is still prevalent.9,10 A large-scale African study reported a 36% prevalence of wasting and weight faltering among children.11 In eastern India, the prevalence of stunting, wasting, and underweight children remains above 30%.12 Similarly, in Bangladesh, weight faltering affects 33% of children.13
Among the various determinants of stunting, weight faltering is a predominant factor in young children.14,15 According to the 2022 Indonesian Nutrition Status Survey, the prevalence of stunting in Indonesia is 21.6%, with a national target to reduce it to below 14%.16 Stunting is closely linked to weight faltering, with 2,349,669 cases reported nationwide.16 West Nusa Tenggara Barat (NTB) is among the provinces with the highest stunting prevalence (32.7%), significantly exceeding the national average.17 Additionally, NTB has 184,922 cases of infants experiencing weight faltering.17
The World Health Assembly (WHA) has emphasized the need to address child growth failure since 2012, urging countries to reduce low birth weight rates and address underweight issues.9 Weight faltering, if left unaddressed, can lead to underweight and increase the risk of long-term wasting and stunting,3,18 resulting in weakened immune responses, higher susceptibility to infections, cognitive impairments, and developmental challenges.19–21
Interventions to address weight faltering and stunting in Indonesia and NTB include specific and sensitive approaches. Specific interventions involve addressing pregnant women’s and teenage girls’ nutritional needs and promoting exclusive breastfeeding, while sensitive interventions focus on environmental, social, and cultural aspects.22,23 However, these approaches have not yet fully engaged the community, particularly pregnant women and mothers of young children, in caring for infants during the critical first 1000 d of life, as evidenced by the high number of weight-faltering cases in NTB.
Several interventions to address weight-related or nutritional issues include improving household and environmental sanitation, addressing social and demographic factors in families with weight-faltering children,24,25, and providing direct nutrition to underweight children through complementary feeding.26,27 Educational interventions for pregnant women28,29 and empowering mothers through self-help groups (SHGs) are also considered effective.
Previous research indicates that SHGs have a positive influence on behavioral changes among their members.30 Various studies suggest that SHGs can promote behavior change by enhancing health knowledge and strengthening group capacity.31,32 Recent studies even show that SHGs can be implemented online through social media groups, as demonstrated in studies involving respondents with psychological disorders.33 However, while previous studies have provided valuable insights, many have not adequately controlled for critical confounding factors that directly influence child weight outcomes, such as children’s daily nutritional intake and parenting styles. Furthermore, they have rarely included long-term follow-up, thereby limiting the generalizability of their findings.
An innovative approach is therefore needed to mitigate the potential long-term impact of weight faltering on stunting development. Developing SHGs within communities may enhance mothers’ understanding and attitudes toward stunting. Furthermore, empowering mothers and supporting them in meeting their children’s nutritional needs could be essential to improving child weight outcomes. This study makes a unique contribution by integrating an SHG-based intervention into community health services, a relatively novel approach in Indonesia that has not been extensively explored in prior research.
The study aimed to analyze the impact of SHGs on child weight, maternal knowledge, and maternal attitudes toward weight faltering and stunting among mothers of children experiencing weight faltering. Data collection focused on community groups, specifically mothers of children experiencing weight faltering, and the intervention was delivered through a community nursing model via the establishment of SHGs. The novelty of this study lies in evaluating the impact of SHGs on maternal knowledge, attitudes, and children’s weight—an aspect that, to our knowledge, has not been addressed in prior research targeting mothers of weight-faltering children for stunting prevention, thereby filling a critical gap in community-based interventions.
This study employed a quasi-experimental pretest–posttest design to evaluate the effectiveness of an SHG-based intervention in improving maternal knowledge, attitudes, and child weight. The study was conducted over 3 months (September–December 2023) at the Pringgarata and Kopang Community Health Centers in Central Lombok District, West Nusa Tenggara Province, Indonesia. The intervention consisted of 5 structured sessions delivered through community-based SHGs.
The SHG program was integrated into the existing Posyandu (Integrated Health Service Post) framework, a government-supported community health initiative operating under the supervision of local community health centers. By embedding SHGs within this established platform, the intervention ensured accessibility, sustainability, and alignment with ongoing maternal and child health services, while providing a novel community-driven model for addressing weight faltering.
The study population consisted of mothers with infants under 3 years old who were identified as experiencing weight faltering, defined as a drop of at least 1 Z-score in weight-for-age over time according to the WHO Child Growth Standards. Weight measurements were conducted by trained healthcare professionals and Integrated Health Service Post cadres using standardized and calibrated anthropometric scales to ensure accuracy.
The minimum required sample size was calculated using an online calculator designed for “before-and-after” clinical research.34 The parameters used were significance level (α) = 0.05, power (1-β) = 80%, effect size (E) = 0.50, and SD of change (SΔ) = 1.00. This calculation resulted in a minimum sample size of 34 participants. In practice, 52 participants were recruited using purposive sampling to account for potential attrition.
Inclusion criteria were (1) mothers with infants aged 0–36 months; (2) mothers actively participating in Integrated Health Service Post activities; and (3) infants identified as experiencing weight faltering but otherwise healthy. Exclusion criteria were (1) infants already diagnosed with stunting and (2) infants with chronic or infectious diseases. Eligible participants were recruited from 4 Integrated Health Service Posts within the study area.
The independent variable in this study was the SHG intervention. SHGs are informal, community-based support systems in which members provide mutual assistance to address shared challenges. These groups operate as peer-support mechanisms that foster empowerment through social learning, interpersonal interaction, and knowledge exchange.35,36 While SHGs have been widely adopted in global health programs, their integration into maternal and child health interventions in Indonesia remains limited. In NTB, SHGs are not yet incorporated into formal stunting-prevention strategies, as maternal and child health services primarily rely on the Pos Pelayanan Terpadu (Posyandu, Integrated Health Service Post) and Pusat Kesehatan Masyarakat (Puskesmas, Community Health Centers).
This study introduced SHGs as a novel intervention to empower mothers of children experiencing weight faltering through structured peer support, education, and training. The intervention was implemented in 5 stages (see Figure 1), combining peer-driven engagement with expert-guided nursing actions. The stages included group formation and orientation, counseling on weight faltering, structured health education, cooking demonstrations for complementary feeding, and post-intervention evaluation. A summary of the intervention activities is presented in Table 1.
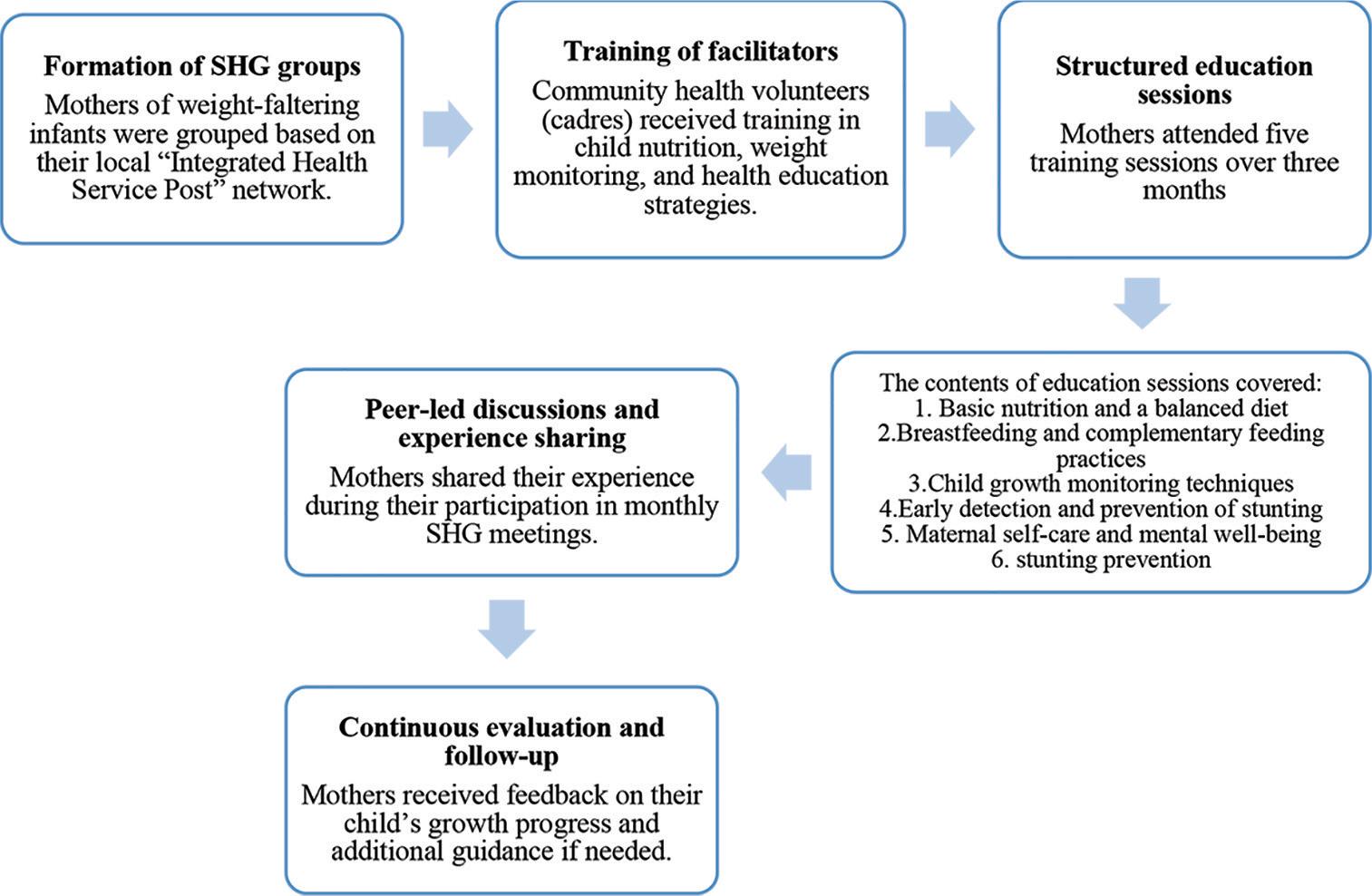
SHG implementation flowchart. Abbreviation: SHG, self-help group.
Stages and activities of the SHG intervention.
| Stage | Description of intervention | Method/approach |
|---|---|---|
| Activity 1: Group Formation and Orientation | Establishment of SHG among mothers of weight-faltering children; orientation on study objectives; explanation of research instruments; and informed consent obtained prior to baseline data collection. | Focus Group Discussion (Pre-intervention) |
| Activity 2: Counseling on Weight Faltering | One-on-one counseling sessions providing information on weight faltering, its relationship to stunting, and strategies for early identification. | Individual Counseling |
| Activity 3: Structured Health Education | Delivery of educational sessions covering essential nutrition, balanced diet, breastfeeding and complementary feeding practices, growth monitoring, maternal self-care, and stunting prevention. Content guided by the “Nursing Actions to Prevent Stunting” (TKCS) module. | Seminar and Group Discussion |
| Activity 4: Cooking Demonstration | Practical sessions demonstrating preparation of high-protein, nutritious complementary foods, followed by participants’ self-practice. | Demonstration and Hands-on Practice |
| Activity 5: Post-Intervention Evaluation | Assessment of maternal knowledge and attitudes after intervention; measurement of children’s weight changes to evaluate intervention outcomes. | Focus Group Discussion and Anthropometric Measurement (Post-intervention) |
Note: SHG, self-help group.
A key educational component of the intervention was the “Nursing Actions to Prevent Stunting” (TKCS) module, developed and validated by experts in nursing, public health, pediatrics, and nutrition. The module covered 4 main areas:
Understanding weight faltering and stunting and their risk factors.
Strategies for preventing weight faltering and stunting.
Nursing interventions for stunting prevention.
Integration of stunting-prevention strategies within the SHG framework.
The module was delivered through group discussions and facilitated by healthcare professionals and Posyandu cadres. By embedding this structured module within SHG activities, the intervention provided a culturally adapted and replicable approach to enhancing mothers’ knowledge, attitudes, and practices regarding the prevention of weight faltering and stunting.
The dependent variables in this study were children’s weight, mothers’ knowledge about stunting, and mothers’ attitudes toward stunting.
Children’s weight was the primary anthropometric outcome assessed in this study, with a specific focus on identifying weight faltering. Weight was measured using a standardized SECA digital weighing scale with an accuracy of ±50 g. Measurements were conducted at each SHG session by trained nurses and community health cadres.
To ensure accuracy and reliability, all personnel involved in the measurement process participated in a structured training program on anthropometric techniques before data collection. The training was facilitated by public health nutritionists from the community health center and lasted for 2 d. The curriculum included theoretical sessions on child growth monitoring, practical demonstrations of proper infant positioning during weighing, calibration of weighing scales, and standardized recording procedures. A competency assessment was conducted at the end of the training to verify the ability of cadres and nurses to consistently and accurately perform measurements.
Each weighing session began with scale calibration according to the manufacturer’s guidelines. Infants were weighed with minimal clothing and positioned correctly to minimize measurement error, following the WHO guidelines for child anthropometry. Weight faltering was operationally defined as a decrease of at least 1 Z-score in the child’s weight-for-age index over time, based on the WHO Child Growth Standards.
Mothers’ knowledge regarding weight faltering and stunting was assessed through a structured, closed-ended questionnaire consisting of 10 items that covered the definition, symptoms, impacts, management strategies, and information on high-protein foods. Each correct answer was awarded 1 point, with total scores ranging from 0 to 10. Knowledge levels were categorized as follows: good (8–10 points), sufficient (5–7 points), and insufficient (<5 points).37 The questionnaire was administered in Bahasa Indonesia to ensure comprehension and cultural appropriateness. Prior to implementation, the instrument underwent expert validation by pediatricians, nutritionists, and nursing academics, and was pilot-tested among 20 mothers outside the study population. Construct validity was supported by a Pearson correlation coefficient of 0.855, while internal consistency reliability demonstrated a Cronbach’s alpha of 0.870, indicating strong psychometric properties.
Maternal attitudes were measured using a 14-item questionnaire designed to capture mothers’ perceptions and parenting practices related to exclusive breastfeeding, complementary feeding, and stunting prevention. Each item was scored dichotomously (1 = positive, 0 = negative), yielding a total score ranging from 0 to 14. Attitude levels were classified as very good (11–14 points), good (7–10 points), and poor (<6 points).37 The instrument was adapted from previously validated maternal health attitude scales and underwent linguistic and cultural adaptation for the local context. Reliability testing showed good internal consistency, with a Cronbach’s alpha of 0.870. The questionnaire was also administered in Bahasa Indonesia and facilitated by trained enumerators to minimize misinterpretation and response bias.
Data collection was conducted between September and November 2023, in collaboration with 8 community health cadres affiliated with the Integrated Health Service Posts (Posyandu), under the supervision of the Pringgarata and Kopang Community Health Centers. Recruitment of participants was conducted during routine Posyandu sessions, supplemented with home visits for mothers who were unable to attend, ensuring comprehensive participation.
The study followed a structured sequence of activities consisting of a pretest survey, implementation of the SHG intervention, and a posttest evaluation. At baseline, respondents completed the knowledge and attitude questionnaires, while trained nurses and cadres took the children’s anthropometric measurements using WHO-standardized procedures. To maximize accessibility, questionnaires were distributed in both online format via Google Forms and printed versions administered directly during Posyandu sessions. Out of 58 recruited respondents, 52 completed all phases of data collection.
The SHG-based intervention was subsequently implemented over 3 consecutive weekly sessions. Each SHG group was facilitated by the researcher in collaboration with community health cadres, using the validated “Nursing Actions to Prevent Stunting” (TKCS) module as the core educational material. Intervention activities included group discussions, structured health education, peer support, and skill-based demonstrations such as complementary food preparation. Attendance was closely monitored, and health cadres provided continuous reminders to ensure participant engagement.
Posttest data collection was conducted at the final session, where anthropometric measurements were repeated and the knowledge and attitude questionnaires were re-administered. The research team supervised all data collection activities to ensure accuracy, adherence to protocol, and consistency across sites.
All tests were 2-sided with α = 0.05. Descriptive statistics summarized respondent characteristics (frequencies/percentages for categorical variables; means and SDs for continuous variables). Pre–post changes were evaluated using paired t-tests for maternal knowledge and attitude scores, and the Wilcoxon signed-rank test for child weight. Between-group comparisons of improvement used independent t-tests on change scores (Δ = post – pre) across maternal occupation, educational level, and child’s sex.
Multivariable analyses employed generalized estimating equations (GEE; Gaussian family, exchangeable working correlation) clustered by participant to account for within-subject dependence. Each model included time (post vs pre) and the following covariates: maternal age, educational attainment (≥senior high school vs <senior high school), employment status (employed vs unemployed/housewife), child age (months), and child sex. These models were prespecified to mitigate confounding by measured maternal and child characteristics and provide covariate-adjusted estimates of the intervention effect; residual confounding cannot be ruled out. Descriptive and bivariate analyses were performed using SPSS Statistics version 23 (IBM Corp., Armonk, NY, USA), and multivariable modeling was conducted in R.
Ethical approval for this study was obtained from the Research Ethics Committee of the Faculty of Health at Qamarul Huda Badaruddin University (No. 019/EC/FKES-UNIQHBA/YPPQH/VII/2023). This study strictly adhered to the ethical principles outlined in the Declaration of Helsinki (2013 Revision) and the International Ethical Guidelines for Health-related Research Involving Humans (2016).38
Participation in this study was voluntary, and participants had the right to withdraw at any time before data analysis began. The respective health center authorities granted permission to conduct research at the Pringgarata and Kopang Community Health Centers in the Central Lombok District.
To ensure confidentiality and anonymity, respondent data were handled with strict privacy measures. An information sheet was provided on the first page of the questionnaire, explaining the study objectives, SHG group formation process, study duration, potential risks, and expected benefits. Participants had to review the information and sign the informed consent form before completing the questionnaire. Additionally, respondents were explicitly informed that they could withdraw from the study without facing any consequences.
Table 2 summarizes the sociodemographic characteristics of 52 respondents. The mean age of mothers was 29.0 ± 6.5 years (range 20–45), and the mean age of children was 14.5 ± 8.5 months (range 2–36). More than half of the children were female (57.7%). The majority of mothers were housewives (82.7%), while smaller proportions worked as farmers (5.8%), as teachers (7.7%), as artists (1.9%), or abroad (1.9%). Regarding education, most had completed junior (38.5%) or senior high school (36.5%), while only 9.6% had higher education.
Characteristics of participants (n = 52).
| Variable and categories | Mean ± SD (Min-max) | n (%) |
|---|---|---|
| Age | ||
| Mother’s age | 29.0 ± 6.5 (20–45) | |
| Children’s age | 14.5 ± 8.5 (2–36) | |
| Mother’s occupation | ||
| Unemployed | 43 (82.7) | |
| Farmer | 3 (5.8) | |
| Teacher | 4 (7.7) | |
| Artist | 1 (1.9) | |
| Working abroad | 1 (1.9) | |
| Mother’s education | ||
| Elementary school | 8 (15.4) | |
| Junior high school | 20 (38.5) | |
| Senior high school | 19 (36.5) | |
| Diploma/bachelor | 5 (9.6) | |
| Children’s sex | ||
| Male | 22 (42.3) | |
| Female | 30 (57.7) |
Note: SD, standard deviation.
Figure 2 illustrates maternal knowledge of weight faltering and stunting. The highest correct response rate was for the item on nutritious food (78%), followed by knowledge about stunting (67.7%). Conversely, most respondents (85.5%) answered incorrectly regarding weight faltering, indicating a significant knowledge gap that requires targeted education.
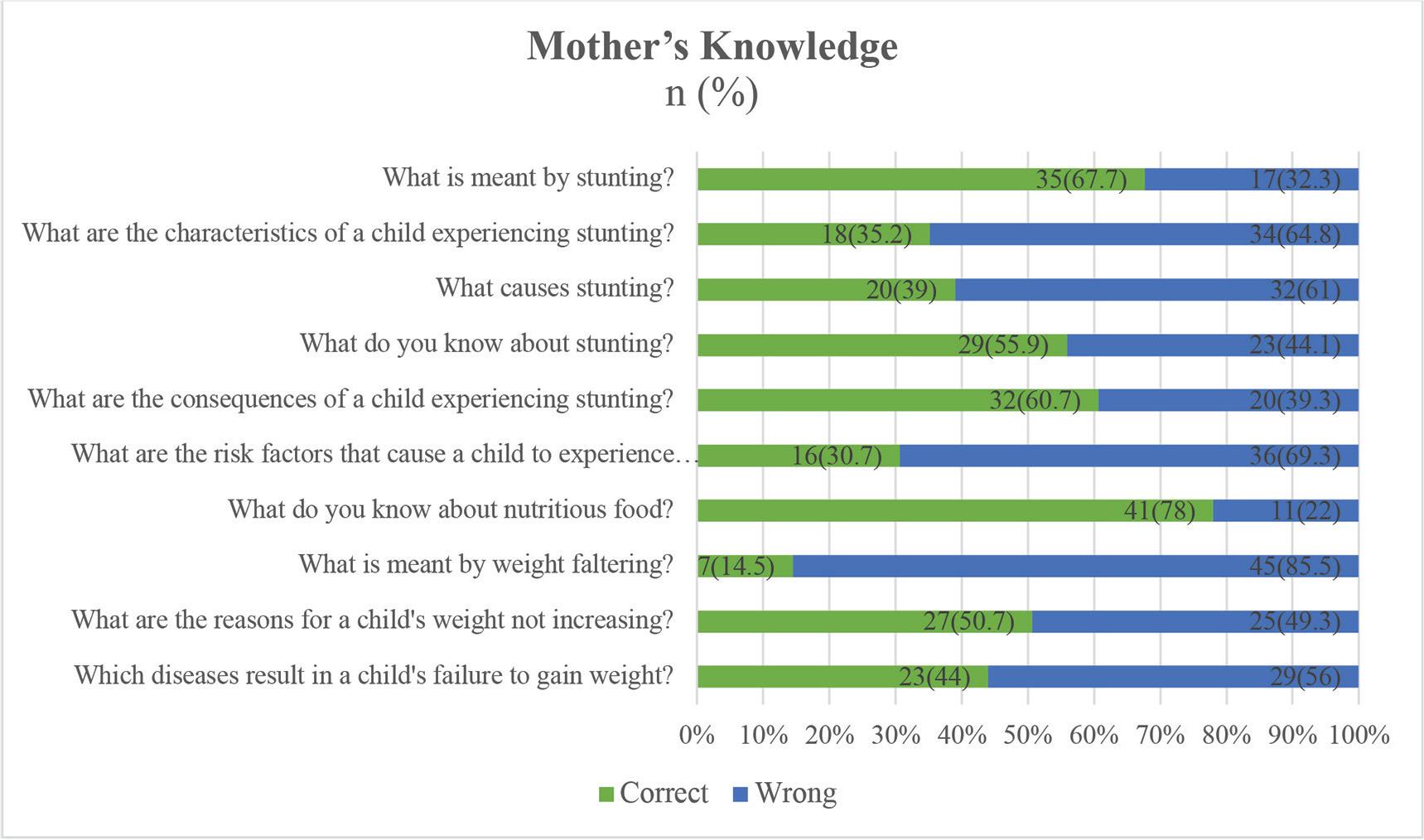
Mother’s knowledge about weight faltering and stunting.
Maternal attitudes (Figure 3) were generally positive. Most mothers (80.8%) agreed that good parenting is essential for child health, and 73.1% agreed that eating more eggs supports the prevention of stunting. However, fewer than 40% agreed with statements on the benefits of participation in Integrated Health Service Posts (Posyandu) and on the association between low birth weight and stunting, suggesting areas for further strengthening of attitudes.
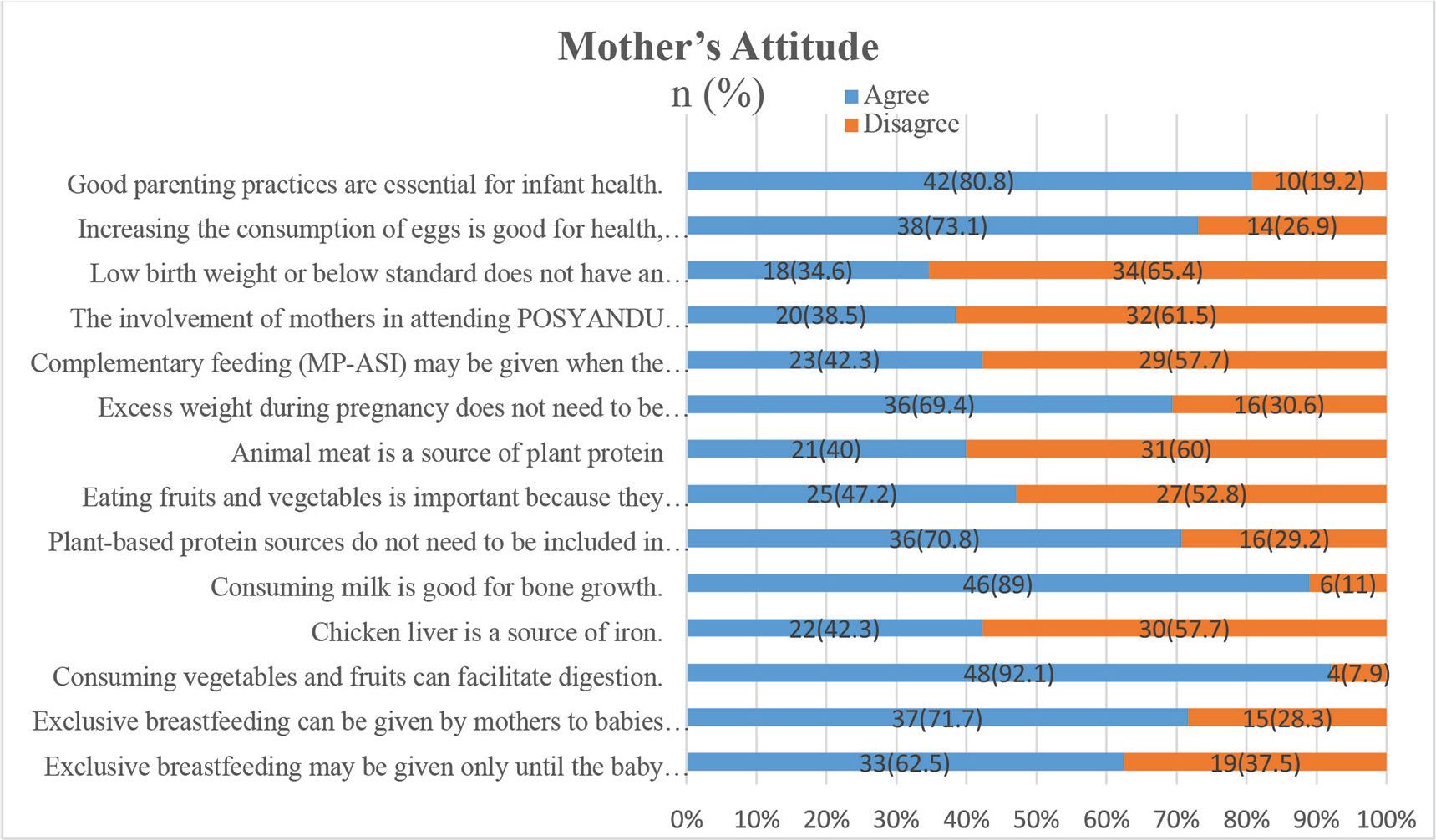
Mother’s attitude toward weight faltering and stunting.
The association between respondent characteristics (occupation, education, and child’s sex) and maternal knowledge is presented in Tables 3.1 and 3.2. Pre- and post-intervention chi-square tests yielded P-values >0.05 across all comparisons, indicating no statistically significant associations between respondent characteristics and maternal knowledge levels. However, descriptive patterns suggest that knowledge improvement was more pronounced among mothers with higher levels of education and employed status, although not reaching statistical significance.
Relationship between respondent characteristics and respondents’ level of knowledge pre-intervention (n = 52).
| Variables and categories | Knowledge level | 𝒳 | P * | ||
|---|---|---|---|---|---|
| Good | Sufficient | Insufficient | |||
| Mother’s occupation | 0.057 | 0.972 | |||
| Employed | 1 | 4 | 4 | ||
| Unemployed | 6 | 19 | 18 | ||
| Mother’s education | 5.950 | 0.051 | |||
| Elementary and junior high school | 2 | 10 | 16 | ||
| Senior high school and universities | 5 | 13 | 6 | ||
| Children’s sex | 1.910 | 0.385 | |||
| Male | 4 | 11 | 7 | ||
| Female | 3 | 12 | 15 | ||
Note: Chi-square test.
Relationship between respondent characteristics and respondents’ level of knowledge post-intervention (n = 52).
| Variables and categories | Knowledge level | 𝒳 | P* | ||
|---|---|---|---|---|---|
| Good | Sufficient | Insufficient | |||
| Mother’s occupation | |||||
| Employed | 5 | 3 | 1 | 3.803 | 0.149 |
| Unemployed | 10 | 26 | 7 | ||
| Mother’s education | |||||
| Elementary and junior high school | 9 | 15 | 4 | 0.329 | 0.848 |
| Senior high school and universities | 6 | 14 | 4 | ||
| Children’s sex | |||||
| Male | 6 | 13 | 3 | 0.184 | 0.912 |
| Female | 9 | 16 | 5 | ||
Note: Chi-square test.
Beyond sociodemographic associations, pre-post analyses were conducted to evaluate the effect of the SHG intervention (Table 4). The proportion of mothers with insufficient knowledge decreased from 40.4% to 15.4%, while those with good knowledge nearly doubled (l5.4%–28.8%). Attitudes also improved, with “very good” responses rising from 25.0% to 40.4%, and no respondents remaining in the poor category. Paired t-tests confirmed significant increases in maternal knowledge (5.6 ± 1.9 vs. 6.9 ± 1.3; P < 0.001) and attitudes (9.5 ± 2.7 vs. 11.5 ± 1.8; P < 0.001). For child weight, the Wilcoxon signed-rank test indicated a significant pre-post increase (P = 0.029; Tables 4 and 6).
Differences in maternal knowledge, maternal attitudes, and children’s weight before and after intervention (n = 52).
| Variables and categories | Pretest | Posttest | P * | ||||
|---|---|---|---|---|---|---|---|
| n (%) | Mean ± SD | Min-Max | n (%) | Mean ± SD | Min-Max | ||
| Mother’s knowledge | 5.6 ± 1.9 | 1.0–9.0 | 6.9 ± 1.3 | 3.0–9.0 | <0.001 | ||
| Good | 8 (15.4) | 15 (28.8) | |||||
| Sufficient | 23 (44.2) | 29 (55.8) | |||||
| Insufficient | 21 (40.4) | 8 (15.4) | |||||
| Mother’s attitude | 9.5 ± 2.7 | 4.0–13.0 | 11.5 ± 1.8 | 8.0–15.0 | <0.001 | ||
| Very good | 13 (25.0) | 21 (40.4) | |||||
| Good | 27 (51.9) | 31 (59.6) | |||||
| Poor | 12 (23,1) | 0 (0) | |||||
| Children’s weight | 52 (100) | 9.7 ± 10.8 | 3.4–85.0 | 10.2 ± 9.1 | 5.1–73.0 | 0.029 | |
Note: Paired t-test; SD, standard deviation.
Analysis of mean differences (Table 5) demonstrated varying trends across subgroups. Working mothers exhibited a greater mean increase in knowledge (2.0 ± 2.7) compared to unemployed mothers (1.2 ± 2.4), whereas unemployed mothers demonstrated greater improvements in attitudes (1.9 ± 3.0 vs. 0.9 ± 3.2). Similarly, mothers with elementary-junior high school education showed greater mean improvements in both knowledge (1.9 ± 2.6) and attitudes (2.2 ± 3.1) compared with those with higher education. Mothers of female children also exhibited greater improvements than those of male children for both knowledge (1.7 ± 2.6 vs. 0.9 ± 2.3) and attitudes (2.1 ± 2.1 vs. 1.2 ± 3.4).
Analysis of the mean difference (delta test) of knowledge and attitudes (n = 52).
| Variables and categories | Knowledge | P | Attitude | P | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Mother’s occupation | 0.371 | 0.389 | ||||
| Employed | 2.0 | 2.7 | 0.9 | 3.2 | ||
| Unemployed | 1.2 | 2.4 | 1.9 | 3.0 | ||
| Mother’s education | 0.072 | 0.217 | ||||
| Elementary and junior high school | 1.9 | 2.6 | 2.2 | 3.1 | ||
| Senior high school and universities | 0.7 | 2.1 | 1.1 | 3.0 | ||
| Children’s sex | 0.248 | 0.323 | ||||
| Male | 0.9 | 2.3 | 1.2 | 3.4 | ||
| Female | 1.7 | 2.6 | 2.1 | 2.1 | ||
Note: SD, standard deviation.
Nevertheless, independent t-tests revealed no statistically significant differences across these subgroups (P > 0.05). These findings indicate that while certain demographic groups appeared to benefit more in absolute terms, the SHG intervention effectively improved maternal knowledge and attitudes across all subgroups without significant disparity.
To mitigate confounding, covariate-adjusted GEE models were fitted, including maternal age, educational attainment, employment status, child age, and child sex. As shown in Table 6, the adjusted time effect (post vs pre) remained significant for maternal knowledge (β = 1.188; 95% confidence interval [CI] 0.336–2.041; P = 0.0063) and attitudes (β = 1.701; 95% CI 0.636–2.766; P = 0.0017), while it was not significant for child weight (β = 0.041; 95% CI - 0.665–0.747; P = 0.9095). Consistently, the Wilcoxon test demonstrated a significant pre–post increase in child weight (P = 0.029; Table 6), indicating that the short-term gain is detectable under distribution-free assumptions.
Multifactor analysis with adjusted intervention effects (post vs pre) from GEE and nonparametric robustness (Wilcoxon) (n = 52).
| Outcome | GEE β (post vs pre), 95% CI | P (GEE) | Wilcoxon P |
|---|---|---|---|
| Knowledge | 1.188 (0.336–2.041) | 0.0063 | 0.00071 |
| Attitude | 1.701 (0.636–2.766) | 0.0017 | 0.00067 |
| Child weight | 0.041 (-0.665 to 0.747) | 0.9095 | 0.0290 |
Note: CI, confidence interval; GEE, generalized estimating equations.
This study aimed to analyze the effect of SHG on child weight, maternal knowledge, and maternal attitudes toward weight faltering and stunting among mothers of children experiencing weight faltering. Nursing interventions to address weight faltering and prevent stunting require a combination of community nursing care models, including the formation of mother self-help groups (SHGs) for stunting prevention. This strategy was employed as a health promotion model targeting mothers with toddlers experiencing weight faltering, with the goal of improving maternal knowledge and attitudes in providing care and high-protein nutrition to their children to prevent stunting.
Health promotion has a long-standing tradition of empowering communities to gain control over the determinants of public health.1,39 Health innovations, multidisciplinary strategies, and public health education initiatives, especially those led by healthcare practitioners, help guide communities in addressing the complex challenges of stunting and its prevention.40–43 This study adopted such an approach, applying a community nursing model that incorporated education and training on stunting prevention, culminating in the establishment of SHGs among mothers of infants with weight faltering.32,44 Consistent with this approach, covariate-adjusted GEE models indicated that the intervention produced significant gains in maternal knowledge and attitudes, whereas the adjusted effect on child weight was not significant (Table 6); by contrast, a distribution-free Wilcoxon test still detected a significant pre-post increase in weight (P = 0.029; Table 4), suggesting a short-term improvement that may be attenuated after adjustment for covariates.
The results indicated that most mothers’ knowledge and attitudes were at a moderate level at baseline. Following the intervention, maternal knowledge improved significantly, with the number of respondents lacking sufficient knowledge decreasing from 21 to 8. Attitudes also improved, with no respondents showing poor attitudes in the posttest. This demonstrates that nearly all participants became more aware of the benefits of early prevention to protect their children from stunting, which was also reflected in the discussions during the third SHG meeting. These findings are consistent with studies in Bangladesh that demonstrated improved maternal knowledge and feeding behaviors following organized health education interventions, leading to higher infant feeding quality at 9 months.13 The substantial increase in maternal knowledge and positive attitudinal changes in this study are likely attributable to the stunting-prevention modules, which addressed participants’ specific challenges—many of whom had previously been unfamiliar with weight faltering, stunting, or preventive strategies. Previous research has similarly shown that stunting education that is tailored to respondents’ concerns can enhance engagement and learning outcomes.45,46 Local health cadres were also engaged to ensure that discussion topics were contextually relevant to participants’ daily problems. Taken together with the multivariable results, these patterns support the robustness of the knowledge and attitude improvements across demographic subgroups.
A key factor influencing maternal care for children experiencing weight faltering was the family’s economic condition, which correlated with maternal employment status and educational attainment. The majority of mothers in this study were unemployed or housewives (82.7%) and had a junior high school education (38.5%) or had not completed high school. These socioeconomic determinants are strongly linked to malnutrition and are often shaped by regional economic contexts.26,47–49 Thus, maternal education and household income are critical in preventing stunting. Addressing these determinants requires collaboration across multiple stakeholders, including government agencies and primary healthcare providers, to implement targeted policies such as providing subsidized or free high-protein foods.
These findings are consistent with studies from Madagascar, which reported high rates of weight faltering among infants in contexts of widespread poverty and low per capita income, where essential nutritional deficits were concentrated among vulnerable groups.41,50 Similarly, research in East Kalimantan, Indonesia, has shown that higher maternal education levels (at least high school) are associated with a lower risk of stunting,51 a result corroborated by studies from Kupang, East Nusa Tenggara.52 These findings suggest that improving education and increasing the per capita income are essential to reducing the prevalence of faltering and stunting in Indonesia.
The intervention strategy of combining SHGs with visual health education modules (“Nursing Actions to Prevent Stunting”) was effective in supporting mothers’ efforts to prevent stunting.53 Beyond education, cooking demonstrations were also provided to strengthen mothers’ attitudes toward preparing high-protein meals and to teach them how to create nutritious complementary foods for children aged 0–36 months.54,55 The evaluation of child weight showed that the average increase during the final study period was approximately 0.5 kg. In light of the adjusted analyses, the magnitude of short-term weight change observed here may reflect early behavioral changes that require longer exposure and tighter control of diet- and care-related confounders to translate into sustained anthropometric gains. It is therefore recommended that government agencies and community health stakeholders continue to promote the use of local protein-rich foods in stunting prevention programs, particularly through Integrated Health Service Post cadres, to sustain improvements in weight gain.
Another finding of this study is consistent with a previous trial in Malawi, which involved providing complementary foods alongside breast milk, including legumes, to infants with weight faltering; this intervention resulted in significant weight recovery.27 Similarly, in Gambia, a combination of nutritious staple foods and targeted nutritional interventions halved the prevalence of malnutrition among children.26 These results highlight the importance of sustaining preventive nutrition interventions to reduce the prevalence of faltering and stunting in Indonesia and comparable settings.
Despite its contributions, this study has some limitations. The sample size was relatively small, primarily due to recruitment challenges in engaging mothers of children with weight faltering and stunting. Additionally, no adjustments were made for potential confounding variables, such as daily nutrient intake, parenting style, hygiene practices, or sleep patterns, which may also influence child weight gain. The relatively short follow-up period of 3 months may further limit the generalizability of findings to longer-term outcomes. Accordingly, future studies should employ larger samples, longer follow-up, and prospective measurement of key confounders (e.g., dietary intake, caregiving practices, household hygiene) to yield more precise, covariate-adjusted estimates of the intervention’s impact on child growth. Nevertheless, these limitations should not overshadow the study’s contribution, as it provides valuable insights and a broad analysis of the impact of SHGs on maternal knowledge, maternal attitudes, and child weight gain.
The study found a significant improvement in maternal knowledge and attitudes following the intervention, with pretest and posttest knowledge levels showing a statistically significant difference, and attitude scores increasing significantly. In multivariable models, the post-intervention gains in knowledge and attitudes remained significant. In contrast, changes in child weight were modest—detectable in nonparametric pre–post testing but not significant after adjustment. The conclusion highlights that SHGs integrated within community services are valuable for promoting health education among mothers at risk of stunting. It suggests that community health centers should establish volunteer groups to collaborate with mothers’ groups, enhancing knowledge and attitudes about stunting prevention. Longer program exposure and closer control of diet- and care-related factors are likely needed to consolidate weight gains. In addition, the government should support such intervention by providing funding, enhancing infrastructure, and issuing regulations to ensure the sustainability of faltering and stunting prevention.