
Total hip arthroplasty (THA) is a widely performed surgical procedure for treating various end-stage hip diseases. With the aging population increasing, the number of patients undergoing this operation is growing steadily each year.1 According to projections, the number of THA procedures will double by 2030.2 The success of THA depends not only on proper surgical alignment but also on effective postoperative rehabilitation. Some researchers have emphasized that incorporating active functional exercises after joint replacement significantly improves recovery outcomes compared with relying solely on passive exercises.3 This approach alleviates pain and enhances postoperative motor function.
The concept of kinesiophobia originates from the “fear-avoidance” model, introduced by Lethem et al. in 1983,4 and is primarily associated with chronic pain and surgical procedures. Kinesiophobia causes patients to fear engaging in daily physical activities, leading to avoidance or refusal to exercise because of concerns about potential harm or injury. This avoidance can result in postoperative anxiety, depression, and other negative emotional states.5,6 The study7 have shown that patients with kinesiophobia following joint replacement surgery have a significantly higher risk of complications, such as joint capsule adhesion, muscle atrophy, and lower extremity deep venous thrombosis, due to their reluctance to participate in functional exercises after surgery.
The incidence of kinesiophobia after joint replacement has been reported to exceed 30%.8 This significant surgical population and high prevalence have drawn increasing attention from clinicians in recent years. However, research on postoperative kinesiophobia following THA remains in its early stages. Identifying the risk factors associated with kinesiophobia is essential for reducing its incidence after THA. Addressing certain risk factors during the perioperative period can help prevent the development of kinesiophobia. This study prospectively investigated the factors contributing to kinesiophobia after THA, aiming to provide a theoretical basis for mitigating its occurrence.
In total, 213 patients who underwent THA at a Class III Grade A hospital in Henan Province from June 2020 to June 2023 were selected as the study population using convenience sampling. This research was approved by the hospital’s ethics committee, and all patients provided informed consent for their inclusion in the study. The inclusion criteria were an age of 18 years or older, meeting the diagnostic criteria for end-stage hip diseases and the surgical indications for THA, and no significant cardiovascular or cerebrovascular events within 6 months before the surgery. The exclusion criteria were abnormal coagulation function; severe cardiac, hepatic, or renal complications, severe malnutrition; concurrent surgeries during the perioperative period; and participation in other similar studies.
Demographic data were recorded, including patient age, sex, body mass index, American Society of Anesthesiologists (ASA) score, presence of diabetes mellitus or hypertension, preoperative visual analogue scale (VAS) score, and duration of preoperative pain.
Surgical data were also collected, including the revision surgery status, whether the procedure was unilateral or bilateral, the operation time, the incision length, and intraoperative blood loss.
The Tampa Scale of Kinesiophobia (TSK) was administered to enrolled patients within 48 h postoperatively. The scale consists of 17 questions scored from 1 to 4 points, reflecting the level of agreement (“strongly disagree” to “strongly agree”). A TSK score of >37 indicates kinesiophobia. The TSK score is positively correlated with the intensity of fear related to exercise. The Cronbach’s alpha coefficient for this scale was 0.740, and the test–retest reliability was 0.860.
Adapted from Thomee’s scale, the Knee-Self Efficacy Scale (K-SES) was used to assess self-efficacy in joint replacement patients within 24 h of admission. The scale comprises 22 items rated from 0 to 10, representing confidence levels (“not sure” to “very sure”). The total score reflects the overall level of self-efficacy. The Cronbach’s alpha coefficient for this scale was 0.913, and the test-retest reliability was 0.886.
The Social Support Rating Scale (SSRS) compiled by Xiao11 based on Chinese conditions, is a 10-item scale including 3 dimensions: subjective support (4 items), objective support (3 items), and the utilization of support (3 items). Total scores range from 11 to 72 and reflect the level of perceived social support. Higher scores indicate more subjective socialsupport, objective social support, and better utilization of social support. The scale has been widely used in the Chinese population and has good reliability and validity. The Cronbach alpha coefficient of the scale for this sample was 0.704.
Statistical analysis was performed using SPSS 22.0 software (IBM Corporation, Armonk, New York, United States). Measurement data are expressed as mean ± standard deviation. The independent samples t-test was used to compare 2 groups with normally distributed data, while the rank-sum test was applied for non-normally distributed data. Count data were analyzed using either the chi-square test or Fisher’s exact test. Ordinal data between 2 groups were compared using the Mann–Whitney U test. Binary multivariate logistic regression was conducted to evaluate the association between the occurrence of kinesiophobia after THA and other factors, treating kinesiophobia as the dependent variable and other variables as independent variables. Spearman correlation analysis was performed using GraphPad Prism 9.0 (GraphPad Software, Boston, United States) to identify risk factors. Statistical significance was defined as P < 0.05.
According to the aforementioned TSK score criteria, kinesiophobia was diagnosed postoperatively when the score exceeded 37. Among the cohort of 213 patients who underwent THA, 38 cases of postoperative kinesiophobia were identified, resulting in an incidence rate of 17.84%.
The patients were divided into 2 groups based on the diagnosis of kinesiophobia after THA: the kinesiophobia group (n = 38) and the non-kinesiophobia group (n = 175). The baseline characteristics and comparison results of these 2 groups are presented in Table 1. Patients in the kinesiophobia group had significantly higher preoperative VAS scores and significantly longer preoperative pain durations than those in the non-kinesiophobia group (P < 0.05). By contrast, patients in the kinesiophobia group had significantly lower education levels, self-efficacy scores, and social support scores than those in the non-kinesiophobia group (P < 0.05). No significant differences were found between the 2 groups regarding age, sex, body mass index, ASA classification, preoperative complications, revision surgery rate, one-stage bilateral replacement rate, operation time, incision length, or intraoperative blood loss (P > 0.05)
Baseline data and univariate analysis results of patients in the 2 groups (
| Indicators | The kinesiophobia group (n = 38) | The non-kinesiophobia group (n = 175) | Statistical value | P |
|---|---|---|---|---|
| Age (years) | 66.18 ± 6.93 | 64.27 ± 7.31 | t = 1.478 | 0.141 |
| Gender (cases, male/female) | 20/18 | 94/81 | x2 = 0.015 | 0.903 |
| BMI (kg/m2) | 28.05 ± 4.07 | 27.70 ± 5.09 | t = 0.397 | 0.692 |
| ASA classification (cases, I/II/III) | 22/15/1 | 102/61/12 | Z = -0.155 | 0.877 |
| Comorbidities | ||||
| Diabetes (cases, yes/no) | 4/34 | 17/158 | x2 = 0.023 | 0.879 |
| Hypertension (cases, 0/I/II/III) | 4/19/13/2 | 21/101/42/11 | Z = -0.873 | 0.383 |
| Preoperative VAS (points) | 6.29 ± 1.27 | 5.52 ± 1.11 | t = 3.456 | 0.001 |
| Preoperative pain duration (months) | 65.95 ± 10.97 | 62.86 ± 7.23 | t = 2.152 | 0.033 |
| Revision surgery (cases, yes/no) | 6/32 | 10/165 | x2 = 3.227 | 0.072 |
| Single/bilateral surgery (cases, single/bilateral) | 33/5 | 167/8 | x2 = 2.658 | 0.103 |
| Operative duration (min) | 130.45 ± 41.15 | 128.83 ± 29.94 | t = 0.230 | 0.819 |
| Length of incision (cm) | 14.53 ± 1.30 | 14.58 ± 1.41 | t = -0.227 | 0.821 |
| Intraoperative blood loss (mL) | 308.37 ± 50.49 | 306.18 ± 41.53 | t = 0.249 | 0.804 |
| Education level (cases, junior high school and below/high school/college and above) | 30/5/3 | 85/40/50 | Z = -3.452 | 0.001 |
| K-SES (points) | 141.24 ± 14.84 | 160.90 ± 13.80 | t = -7.854 | <0.001 |
| SSRS (points) | 52.32 ± 6.95 | 59.57 ± 6.40 | t = -6.238 | <0.001 |
Note: ASA, American Society of Anesthesiologists; BMI, body mass index; K-SES, Knee-Self Efficacy Scale; SSRS, Social Support Rating Scale; VAS, visual analogue scale.
Table 2 presents the results of the binary logistic regression analysis, with the occurrence of kinesiophobia after THA as the dependent variable and various factors as independent variables. The validity of the model was assessed using a chi-square test (χ2 = 96.161, P < 0.001), demonstrating a classification accuracy of 90.70%. Preoperative VAS scores were identified as a significant risk factor for post-THA kinesiophobia (P < 0.05). Additionally, education level and self-efficacy were found to be protective factors associated with a reduced likelihood of developing kinesiophobia following THA (P < 0.05).
Binary Logistic regression analysis results of kinesiophobia after THA.
| Factors | Regression coefficient | Standard error | P |
|---|---|---|---|
| Education level | –1.282 | 0.409 | 0.002 |
| Preoperative VAS | 0.616 | 0.252 | 0.015 |
| Self-efficacy | –0.102 | 0.022 | <0.001 |
Note: CI, confidence intervell OR, odds ratio; THA, total hip arthroplasty; VAS, visual analogue scale.
The results indicated that education level, preoperative VAS score, and self-efficacy were significantly associated with the occurrence and severity of kinesiophobia after THA. To further evaluate the impact of each factor on the degree of kinesiophobia, clinical data—including TSK score, education level, preoperative VAS score, and self-efficacy—were analyzed for the 38 patients diagnosed with kinesiophobia after THA. The correlation analysis revealed that education level exhibited a significant negative association with the TSK score (r = –0.647, P < 0.001), while the preoperative VAS score showed a positive correlation with the TSK score (r = 0.697, P < 0.001). Moreover, selfefficacy demonstrated a significant negative correlation with the TSK score (r = –0.756, P < 0.001). These findings suggest that higher education levels and greater self-efficacy act as protective factors against the occurrence and severity of kinesiophobia following THA (Figure 1).
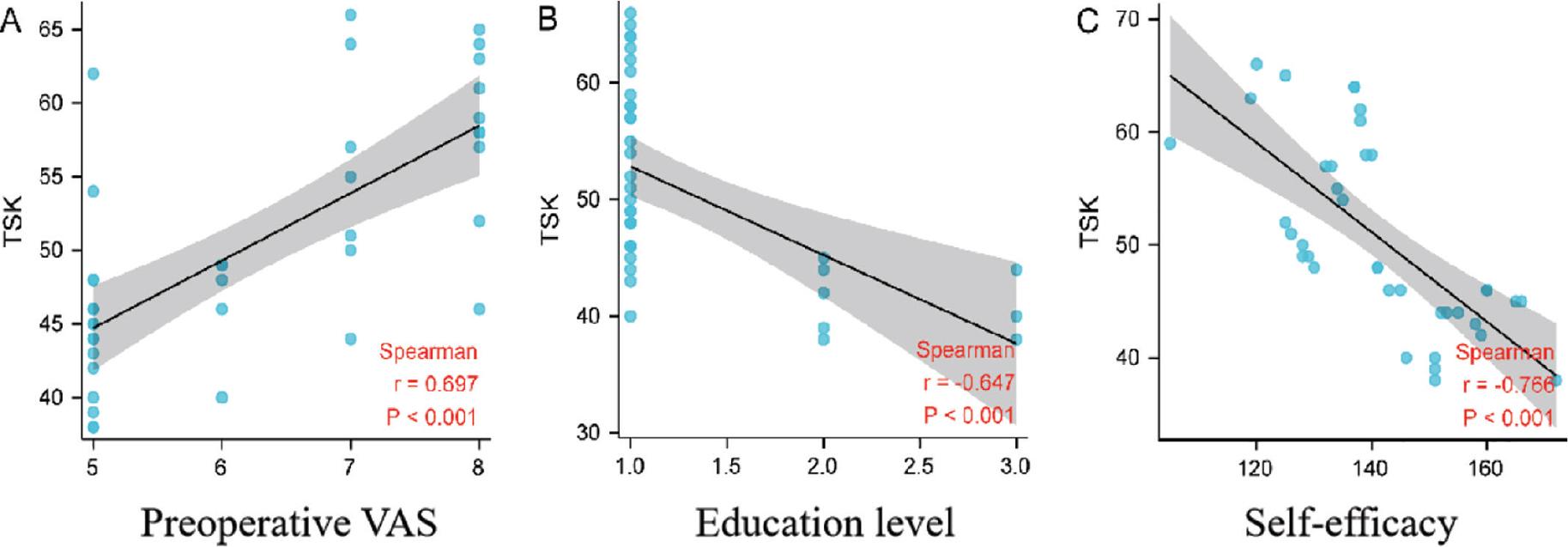
The scatter plots of Spearman correlation between risk factors and TSK scores; (A) Preoperative VAS is positively correlated with TSK scores; (B) Education level is negatively correlated with TSK scores; (C) Self-efficacy is negatively correlated with TSK scores.
Note: TSK, Tampa Scale of Kinesiophobia; VAS, visual analogue scale.
THA is a well-established surgical procedure for treating various end-stage hip diseases, providing significant pain relief and substantial restoration of limb function. As a result, the number of THA surgeries has been steadily increasing in recent years.12 However, postoperative kinesiophobia, a common complication, has garnered attention because of its potential negative impact. Irrational fear among patients can delay early functional exercises and increase the risk of joint replacement adhesion.13 In severe cases, it may even lead to deep venous thrombosis.14 Our study showed that the incidence of kinesiophobia after THA was 17.84%, slightly lower than rates reported in domestic and international literature for joint replacement.8 Binary logistic regression analysis identified the preoperative VAS score, education level, and self-efficacy as factors associated with kinesiophobia after THA. Specifically, higher preoperative VAS scores were positively correlated with greater degrees of kinesiophobia, while education level and self-efficacy demonstrated negative correlations.
The findings from previous studies15,16 have demonstrated a consistent association between the severity of pain and the development of kinesiophobia following surgery, which aligns with our results (odds ratio [OR] = 1.851, P = 0.015). The research has also reported a positive correlation between pain intensity and kinesiophobia levels.17 Prolonged preoperative pain leads patients to perceive pain as harmful, causing them to avoid activities that might induce postoperative discomfort. Studies have indicated that prolonged pain causes patients to excessively focus on external pain signals and interpret them as potential threats, resulting in reluctance to engage in sports or functional exercises.18 Our study further confirmed this by identifying a significant positive correlation between the severity of pain and the degree of kinesiophobia (r = 0.697, P < 0.001) after THA. These findings highlight the critical role of medical professionals in providing not only adequate postoperative analgesia but also proactive preoperative education. This education should address the relationship between pain and activity, emphasizing the importance of early postoperative functional exercise and reassuring patients about its benefits.
The findings of this study revealed that a lower education level was an independent risk factor for kinesiophobia after THA (OR = 0.277, P = 0.002), consistent with previous research outcomes.19 Scholars investigating subacute low back pain have similarly reported that individuals with lower educational attainment are more likely to exhibit resistance to exercise.19 Patients with higher levels of education are better equipped to acquire perioperative rehabilitation knowledge through various sources and approach pain management more rationally. Conversely, patients with limited cognitive abilities and knowledge acquisition due to lower education levels may develop misconceptions about early functional exercise, exacerbating their fear response. Additionally, another study20 indicated that patients with lower education levels may struggle to comprehend health education content provided by medical staff regarding pain management. This lack of understanding, combined with poor compliance during the perioperative period, could contribute to the higher incidence of kinesiophobia in this group. To address this issue, healthcare professionals should engage in multidisciplinary collaboration to implement specialized cognitive-behavioral interventions. These interventions, encompassing psychological, rehabilitative, and nursing perspectives, should aim to enhance patients’ understanding of perioperative functional exercise and pain management. Such efforts can actively encourage postoperative physical activity, particularly among highrisk populations.
Self-efficacy refers to an individual’s belief in their ability to engage in a specific behavior and achieve a desired outcome within a given situation, essentially reflecting confidence in one’s capability to succeed, often expressed as “I can do it.”10 It plays a pivotal role in regulating behavior and influencing physical activity levels. Studies conducted internationally have demonstrated that patients with high self-efficacy are more likely to acknowledge and overcome pain symptoms, adopt a positive attitude toward postoperative pain management, and show greater willingness to address discomfort through exercise. Zelle et al.21 identified a significant negative correlation between self-efficacy and kinesiophobia, and our study further supports these findings. We observed that self-efficacy is associated with reduced kinesiophobia after THA (OR = 0.903, P < 0.001) and has a significant negative correlation with the degree of kinesiophobia (r = –0.766, P < 0.001). These results align with prior research22,23 indicating that higher self-efficacy and positive coping styles are linked to lower incidence rates of limb disuse disability and depression by reducing kinesiophobia. Consequently, healthcare professionals should proactively identify and address patients’ negative emotions during the perioperative period while encouraging family members to provide spiritual and emotional support. Such interventions are essential for helping patients maintain a positive mindset necessary to overcome exercise-related fears.
The present study has several limitations. First, it is a single-center study with a relatively small sample size. Future research should involve multicenter studies with larger sample sizes to provide a more comprehensive understanding of the risk factors associated with kinesiophobia after THA. Second, because the study only included data from patients who underwent THA at 1 tertiary hospital, selection bias may have influenced the findings. The inclusion of patients undergoing THA from hospitals of different levels in future studies would improve the generalizability of the results.
In conclusion, preoperative pain intensity, educational level, and self-efficacy are significant factors associated with kinesiophobia after THA. For high-risk groups exhibiting these risk factors, implementing multidisciplinary collaborative management programs during the perioperative period may effectively reduce the occurrence of kinesiophobia.