
Fig. 1.

Fig. 2.

Fig. 3.
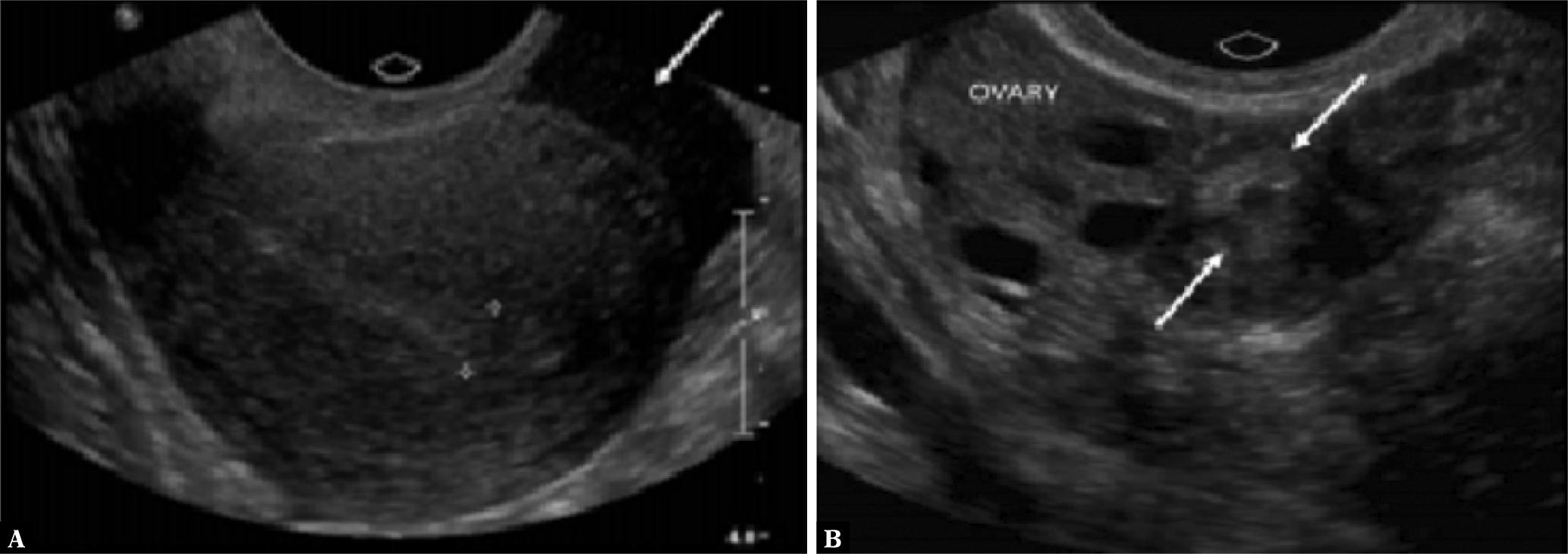
Fig. 4.
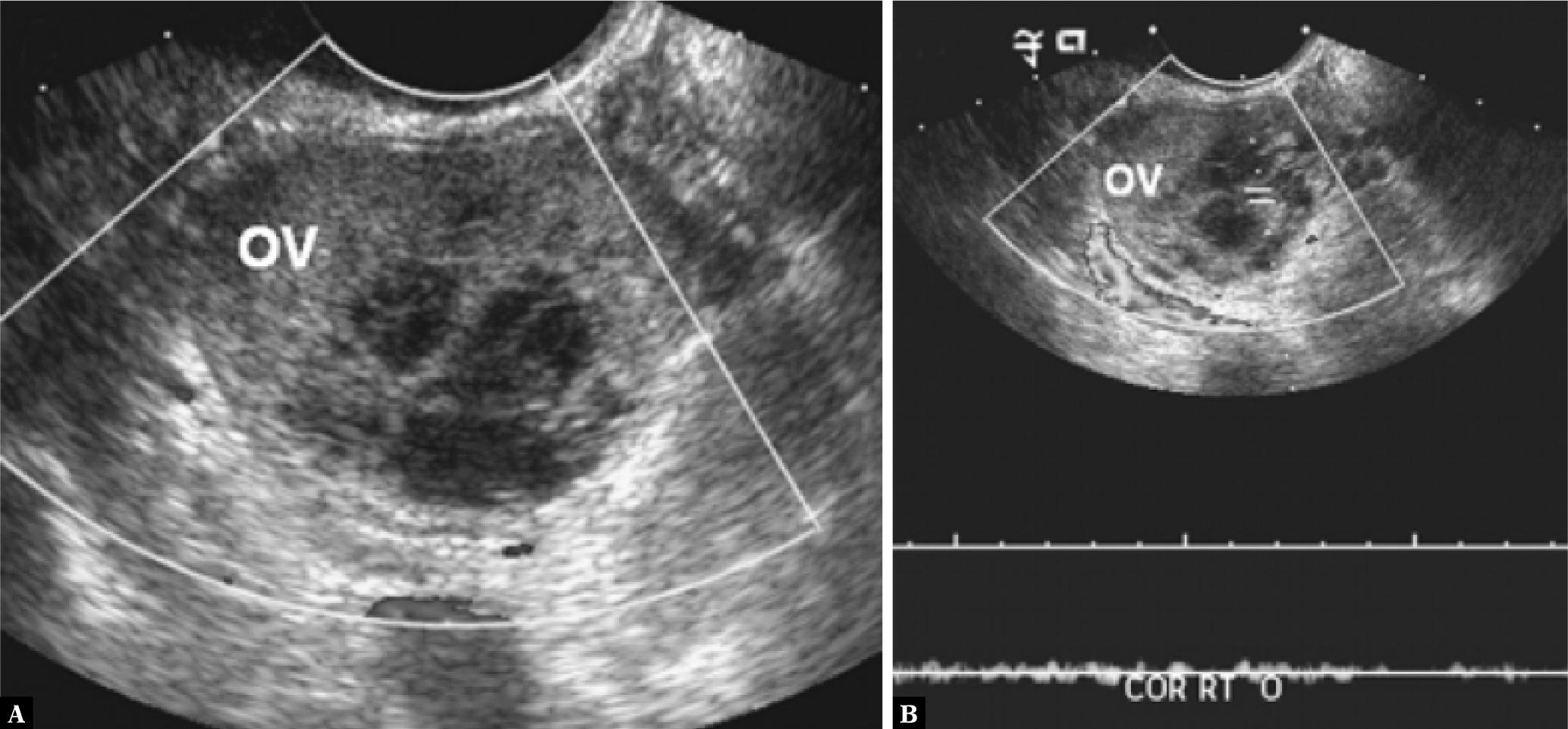
Fig. 5.
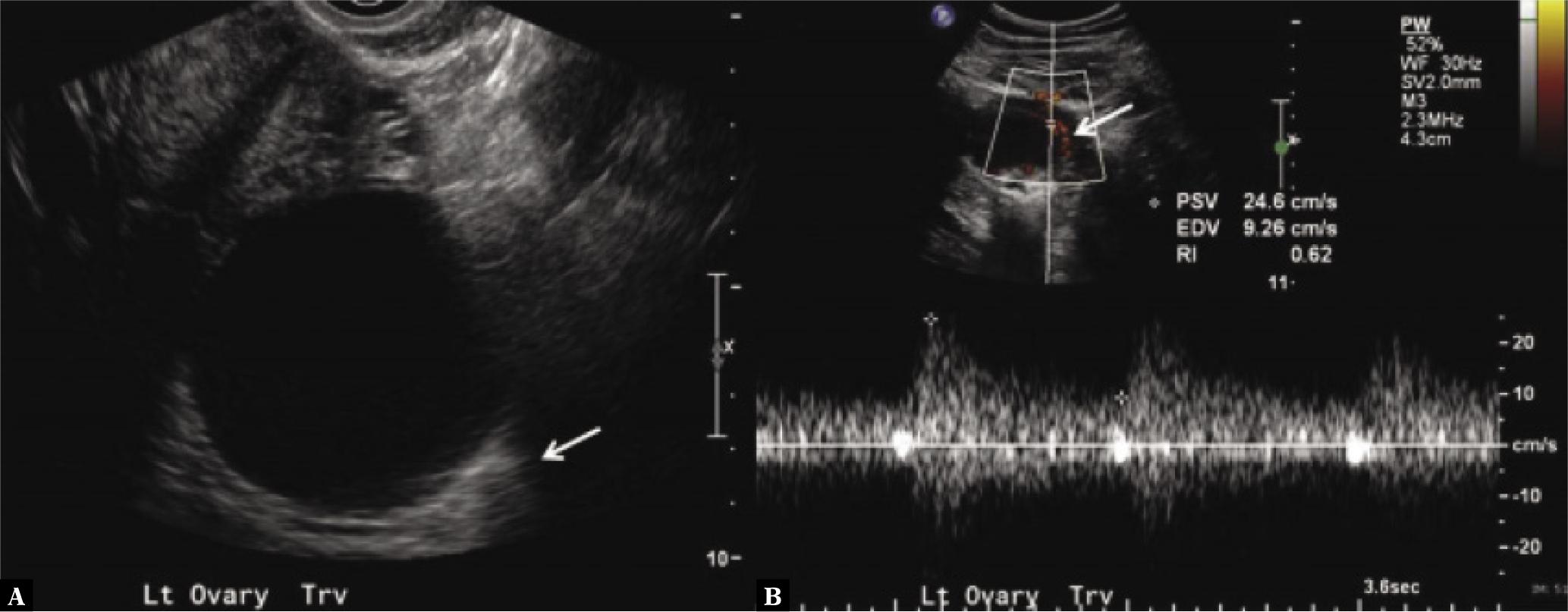
Fig. 6.
Gray-scale and Doppler ultrasound findings for the causes of acute pelvic pain
| Causes of acute pelvic pain | Gray-scale findings | Doppler findings |
|---|---|---|
| Pelvic inflammatory disease |
|
|
| Ectopic pregnancy |
|
|
| Adnexal torsion | A big hemorrhagic cyst in an edematous ovary, an enlarged ovary with follicles scattered peripherally:
|
|
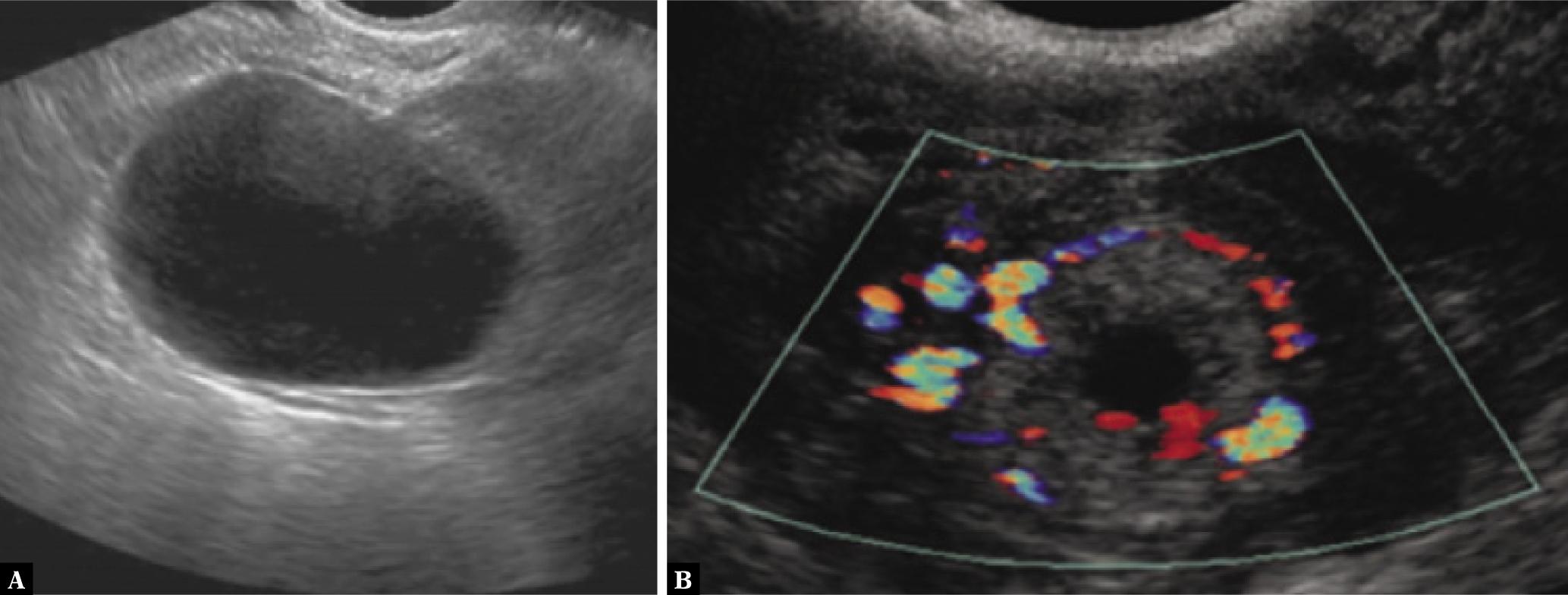
| Ovarian cysts |
|
|
| Adhesions | 2D transvaginal ultrasound (suggestive features):
|