
Early diagnostics of neurodevelopmental disorders is a challenge of contemporary pediatric rehabilitation. The analysis of motor abilities is a basic element of neurological assessment of infants in which muscle tone distribution and head control are evaluated. Assessment is made through observations of spontaneous motor activity of infants with limited visual or audio stimuli from the environment. In clinical practice, an interview is mainly applied as a research method; however, there is a lack of objective, detailed and repeatable methods of assessing muscle tone distribution which may help to commence therapy as quickly as possible to prevent the development of non-physiological movement patterns. Objective methods of neurological evaluation of an infant may facilitate the process of a proper selection of therapeutic techniques and monitoring therapy effects.
According to the NDT/Bobath approach (Neurodevelopmental Treatment), in order to develop properly, infants need appropriate central stability of the trunk which involves integrated work of postural muscles and muscle tone and enables them to maintain balance during motor activities in different body positions [1]. Physiological movement patterns are determined by a proper muscle tone distribution which makes it possible to fight gravity and develop particular motor sequences. Muscle tone distribution differs depending on an infant’s age, which helps to assess the nervous system maturity and to detect potential developmental disorders. Premature infants may suffer from an impaired physiological development and function of the body. The shorter the fetal life, the less mature and less able to adapt to the new environment the infant is after birth.
In this study, support surface of premature infants was compared to support surface of full-term infants. By applying PodoBaby podoscope, an attempt was made at finding an objective and precise method of assessing infantile muscle tone distribution.
The aim of the work was to assess load surface with regard to muscle tone distribution of infants.
The following research questions were addressed:
- –
Does support surface on the right and left side of the body in premature infants lying in a supine and prone position differ from support surface in full-term infants?
- –
Does the length of trunk sides affect support surface on the right and left side of the body?
- –
Is there a correlation between load surface and the length of trunk sides?
Twenty-four infants aged 3-6 months were examined, including 12 premature infants (taking into account their adjusted age) and 12 full-term infants. They were patients of the Neurological Rehabilitation Day Ward at the Neurology, Epileptology and Pediatric Rehabilitation Clinic as well as the Neonatology, Pathology and Intensive Care Ward from the Children’s Memorial Health Institute in Warsaw.
The study group inclusion criteria were as follows: birth before 37 weeks and 3-6 months of adjusted age. In turn, 3-6 months of calendar age and birth on due date (from 38 to 42 weeks) constituted the control group inclusion criteria. The exclusion criteria for both groups included central nervous system damage, genetic and metabolic diseases. An approval from the ethics committee and consent from parents of the infants were obtained.
Prior to the commencement of the study, an interview concerning pregnancy and neonatal period as well as a current state of the infants was carried out and medical records were analysed. Then, a non-invasive measurement of support surface was performed with the use of PodoBaby – a digital podoscope for diagnosing infants and older children (fig. 1). The parameters of PodoBaby are as follows: size – 90x60x55-75 cm, examination surface – 80x50 cm, accuracy – 1 mm, 0.1 degree, connection – USB. PodoBaby podoscope is used for examining infants and diagnosing foot disorders in children up to 5 years old (maximum weight – 25 kg). Computer software connected with PodoBaby presents the results of measurements in the form of numeral parameters and printouts.

PodoBaby podoscope. Source: ww.cq.com.pl (16.09.2017)
The measurement with the use of PodoBaby podoscope makes it possible to perform an objective assessment of support surface in an infant lying in a supine or prone position with regard to the body contour.
The examination was performed in a prone and supine position. An undressed patient was placed on a transparent PodoBaby examination surface, which allowed examiners to take digital images from the bottom side. The images were converted into a digital signal and sent to the computer memory with the use of a special card. The registered image presented psychomotor abilities of an infant at the time of an examination. The infants were examined in safe conditions. One researcher was operating computer software, while the other researcher was supporting the infant lying on PodoBaby podoscope surface.
After an infant’s image was recorded in the computer software, appropriate measurement points were marked on the contour (fig. 2). The results of research were analysed with the use of a segment model and a simple (“Three areas and contour”) model.
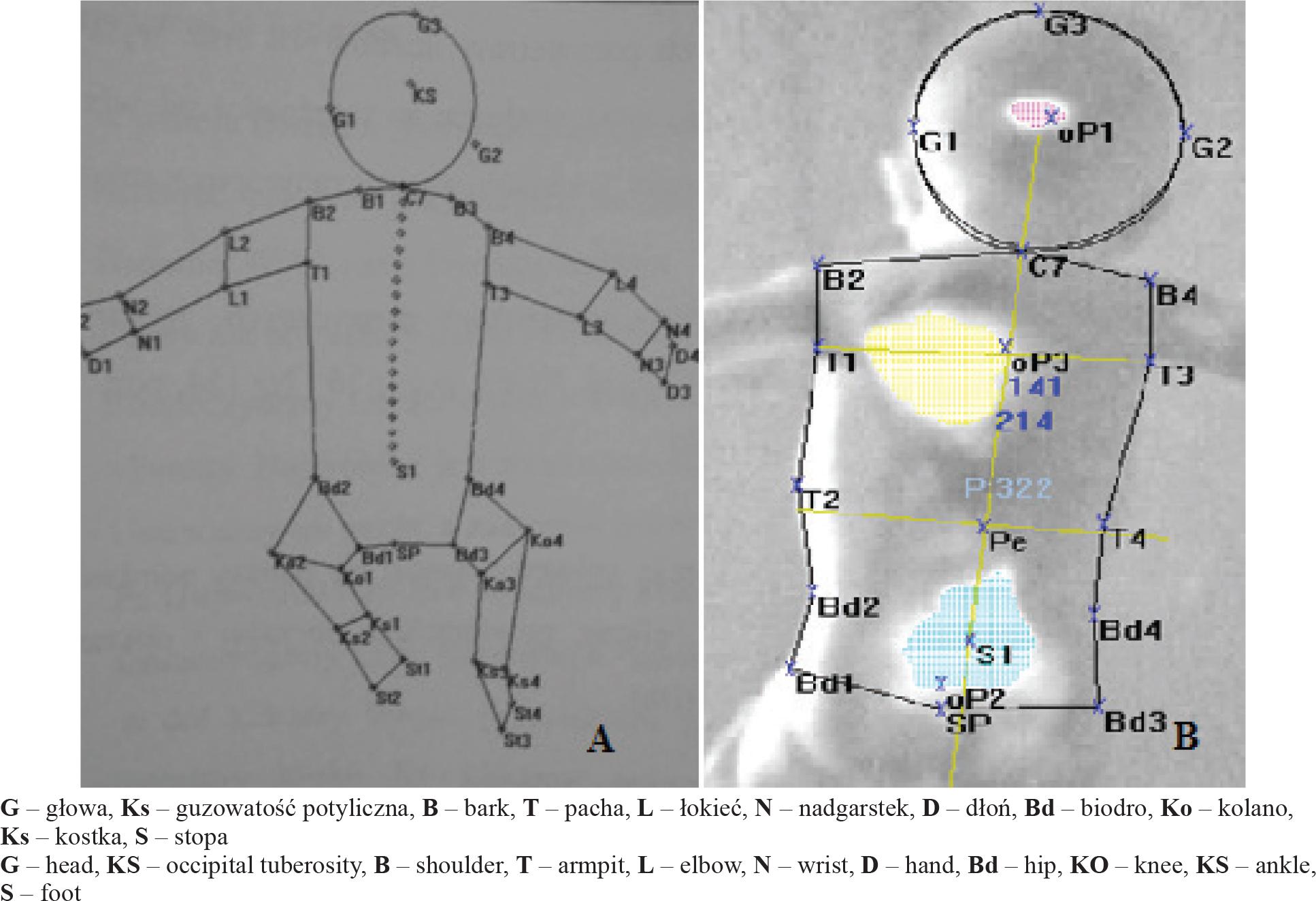
Segment model (2A); “Three areas and contour” model (2B). Source: www.cq.com.pl
In the “Three surfaces and contour” model, the main support surfaces were marked with points oP1-P3. Three surfaces were marked in a supine position (oP1 – surface located at the highest point, i.e. on the head; oP2 – surface in the upper part of the trunk; oP3 – surface in the lower part of the trunk) (fig. 2), while in a prone position, two surfaces were marked (oP2 and oP3). The computer automatically calculated the surfaces and their proportions for particular parts on the right and left side of the body. Thus, areas of the aforementioned surfaces with regard to the sagittal body axis (right-left) were compared. The longitudinal body axis was marked from the spinous process C7 to the first sacral vertebra S1.
The areas of support surface on the right and left side of the body and the lengths of trunk sides were analysed.
The number of study participants is presented in table 1.
The number of infants in the study and control groups
| Niemowlęta przedwcześnie urodzone, n/Premature infants, n | Niemowlęta urodzone o czasie, n/Full-term infants, n | |
|---|---|---|
| Wszyscy/Total | 12 | 12 |
| K/F | 8 (66,7%) | 6 |
| M/M | 4 (33,3%) | 6 |
The statistical analysis of results was performed with the use of Statistica v.12 software. The Student’s t-test was applied. Statistical significance was set at the level of p<0.05.
The percentage distribution of loads with regard to the longitudinal body axis was analysed both in a supine position (Tab. 2) as well as in a prone position (Tab. 3).
The percentage distribution of loads on the right and left side of the body in a supine position and differences regarding these loads between premature and full-term infants
| Urodzeni przedwcześnie/Premature infants | Urodzeni o czasie/Full-term infants | |||||
|---|---|---|---|---|---|---|
| % obciążenia P/% load R | % obciążenia L/% load L | różnica obciążenia/difference in load | % obciążenia P/% load R | % obciążenia L/% load L | różnica obciążenia/difference in load | |
| Średnia±SD; | 60,7±20,8 | 39,3±20,8 | -21,4±41,6 | 63,3±16,3 | 36,7±16,3 | -26,6±32,6 |
| Zakres | 6,8 – 20,2 | 9,8 – 93,2 | -80,3 – 86,3 | 37,9 – 93,2 | 6,8 – 62,1 | -86,3 – 24,3 |
P – P strona ciała, L – L strona ciała / R – right side of the body, L – left side of the body
The percentage distribution of loads on the right and left side of the body in a prone position and differences regarding these loads between premature and full-term infants
| Urodzeni przedwcześnie/Premature infants | Urodzeni o czasie/Full-term infants | |||||
|---|---|---|---|---|---|---|
| % obciążenia P/% load R | % obciążenia L/% load L | % obciążenia P/% load R | % obciążenia L/% load L | % obciążenia P/% load R | % obciążenia L/%load L | |
| Średnia±SD | 60,2±13,62166 | 39,8±13,62166 | 20,5±27,21706 | 53±16 | 47±16 | 6±32 |
| Zakres | 35,1 – 87,3 | 12,7 – 64,9 | -29,7 – 74,5 | 22,4 - 71 | 29 – 77,6 | -55,1 - 42 |
P – P strona ciała, L – L strona ciała / R – right side of the body, L – left side of the body
It was revealed that differences between the means for premature infants and full-term infants were not statistically significant (p=0.98). However, it is worth noting that while analysing the values for each infant individually, considerable differences between the loads on the right and left side of the body could be noted, which may prove the existence of muscle tone disorders and asymmetric body position.
It was revealed that the differences between the means for premature and full-term infants were not statistically significant (p=0.47). On the basis of data included in table 3 it was noted that mean values of loads on the right and left body side of full-term infants lying in a prone position were close to the values typical of trunk symmetry (approximately 50% on each side of the body), while in the case of premature infants, the values differed (60.2% to 39.8%). It leads to the conclusion that premature infants manifest infantile postural asymmetry and improper values of support surface on the right and left side of the body.
The results of the measurements of the lengths of trunk sides and differences between them are presented in table 4. The lengths of sides in a prone position were analysed in a segment model. While analysing the load on the right and left side of the body in a prone position, an increased load on the left side of the body and a longer left side of the trunk were noted more often in premature infants. Thus, when the load is transferred to the left side, this side gets longer, while the right side gets shorter.
The lengths of trunk sides and differences between them in the groups of premature and full-term infants in a prone position
| Urodzeni przedwcześnie/Premature infants | Urodzeni o czasie/Full-term infants | |||||
|---|---|---|---|---|---|---|
| Długość boku P/Length of side – R | Długość boku L/Length of side – L | Różnica długości boków/Difference in side lengths | Długość boku P/Length of side – R | Długość boku L/Length of side – L | Różnica długości boków/Difference in side lengths | |
| Średnia±SD/Mean±SD | 187,9±15,5 | 180,3±15,6 | 7,7±14,6 | 185±22,9 | 176,3±22,8 | 8,8±24,6 |
| Zakres/Range | 161 – 216 | 155 – 207 | -18 – 26 | 141 - 225 | 143 – 212 | -49 - 41 |
P – prawy, L – lewy / R – right, L – left
An interview technique is often applied in the clinical practice of physiotherapists working with infants and children. However, there is a lack of objective, detailed and repeatable methods of assessing muscle tone distribution. To date, numerous studies on infant diagnostics have been published but not many of them concerned the issue of assessing infants with the use of PodoBaby podoscope, which may result from a limited availability of the device.
Pyzio et al. used PodoBaby to examine differences between healthy infants and infants with developmental disorders. They revealed that differences regarding the loads on the right and left side of the body in healthy infants did not exceed 18%, while in the case of infants with developmental disorders, these differences reached 66% [2]. In turn, Czupryna et al. studied support surface in infants with disorders of the central nervous system. A dozen or so infants aged 2-3 months and 8 healthy infants from the control group were examined. It was revealed that infants with disorders of the central nervous system more often manifested trunk asymmetry in a supine position and greater loads in lower parts of the body, particularly in a prone position. However, the authors pointed out that PodoBaby examination should be treated as a new method of examining infants and therefore, it is difficult to compare the results with the findings of other authors [3].
Small study groups constitute a limitation of the studies that have been conducted with the use of PodoBaby podoscope to date. However, in 2013 the results of research conducted on 120 infants aged 3-6 months were published, where 60 study participants suffered from disorders of the central nervous system diagnosed with the use of Vojta method. It was concluded that the diagnosis of trunk asymmetry in PodoBaby examination confirmed the previous clinical diagnosis [4].
Pyzio et al. assessed PodoBaby podoscope measurement method. They analysed the usefulness of the device for assessing symmetry or asymmetry, support surface and transfer of support surface with the center of gravity. Podoscope examination was found to be an objective way of assessing a patient in pediatric rehabilitation [2].
In their research, Yuge et al. revealed that the quality of spontaneous motor activity of infants became one of the most reliable and justified predictors of neurological disorders, particularly the severe ones. The authors concluded that assessment of motor abilities in infants aged 3-5 months considerably improved the potential to identify the risk of developmental disorders [5].
In the literature, studies on the use of PodoBaby podoscope for assessing other positions can also be found. The aim of the work by Adamska et al. was to assess the position of pike sit in babies aged 9 months with the use of PodoBaby podoscope. It was revealed that PodoBaby podoscope may constitute a valuable completion of neurodevelopmental diagnostics [6].
In a similar study with the use of Sensor Mass System, Szopa et al. concluded that assessing the distribution of forces on force platform indirectly allowed for evaluating muscle tone distribution in different forms of activity and constituted a valuable completion of the assessment of motor patterns quality. The authors pointed out that modern examinations would facilitate diagnosing and taking appropriate decisions as well as obtaining better therapeutic results [7].
In the present study, we adopted research methodology similar to that described by Pyzio et al. [2,4]. This is a pilot study which is part of a bigger research project.
- –
No significant differences between premature and full-term infants were revealed in the right side loading in a supine position (analogous lack of differences was noted for the left side and a prone position).
- –
In a supine position, considerable asymmetry of the loads of trunk sides was noted in premature infants, while in the case of full-term infants, the mean values of loads were close to symmetry. The majority of information may be obtained from the analysis of an individual profile of each patient.
- –
There exists a correlation between support surface and the length of trunk sides in a prone position. The loaded side is lengthened while the unloaded side is shortened.