
Cerebral palsy (CP) is the most common cause of physical disability among children [1–5]. Three children per 1000 births in the world are diagnosed with CP, while spastic hemiplegia is its most common form (39% of all the diagnosed cases) [4–8].
As a result of improper muscle tension, weaker muscles and sensory disorders in the affected upper limb, children with spastic hemiplegia often have difficulties reaching for objects, gripping or manipulating them [9,10]. These limitations affect performing activities of daily living (ADLs) such as getting dressed, washing, eating, writing or playing [10–13].
Due to numerous obstacles encountered while performing ADLs, a phenomenon of learned non-use of an affected upper limb can be noted in children with spastic hemiplegia. Due to the fact that children want to catch up with their counterparts and be as fast and effective as them, they neglect the affected limb and use the more efficient one in all activities [10, 14–17].
Currently, Constraint-Induced Movement Therapy (CIMT) is one of the most commonly used interventions which brings about positive effects in overcoming learned non-use [11,14,18]. In this therapy, the unaffected upper limb is restrained with the use of a bandage, glove, orthosis, arm sling or plaster, while the affected limb is trained intensively to perform ADLs [15,16,19,20]. In recent years, more and more studies have revealed some positive effects of CIMT and mCIMT (modified Constraint-Induced Movement Therapy), e.g. an improvement in function, speed, agility and in spontaneous use of the affected upper limb [21–26].
In mCIMT, the main guidelines of CIMT are preserved but with certain modifications regarding, inter alia, duration of the unaffected upper limb restraint, duration of the therapy (number of sessions per week, number of weeks), venue where the therapy is carried out (home, summer camp, kindergarten, hospital) or people who conduct the therapy (parents, guardians, physiotherapists, occupational therapists) [11,20].
In order to achieve optimal effects in the function of an upper limb in children with hemiplegia, the studies recommend combining mCIMT with Bimanual Training (BIT) [27–29]. Following intensive therapy of an upper limb, carefully planned bimanual tasks and plays are implemented.
BIT is a scientifically confirmed method which efficiently improves the function of an affected upper limb and bimanual coordination. It also brings about positive effects in learning self-care activities [12,26,30,31].
The effectiveness of CIMT as well as BIT has been clearly confirmed in numerous scientific studies. However, there are still doubts regarding an optimal amount of therapy, the frequency and intensity of the procedure, duration of intervals (CIMT-BIT), type of restraint applied on the upper limb or the most favourable environment (group or individual therapy, at the clinic or at home) [10,20–22,32].
The aim of the study was to assess the effectiveness of two-week CIMT combined with BIT carried out in an innovative environment within the project titled “The Pirate Group”.
The study included 16 children with CP aged 3-6 years. Due to health issues, one child did not complete the therapy. Mean age of the study participants was 4.23 years (SD=1.03). Inclusion criteria were as follows: diagnosed CP (in the form of spastic hemiplegia), age 3-6 years, level I or II (moving without supporting devices) according to the Gross Motor Function Classification System (GMFCS), level I-III according to the Manual Ability Classification System (MACS) and level I-III according to the Communication Function Classification System (CFCS). Exclusion criteria were as follows: intellectual disability making it impossible to cooperate and follow the therapist’s instructions, uncontrolled seizures, inability to move unsupported. The characteristics of the examined group are included in table 1.
Characteristics of the study group
| n | płeć/sex | wiek w latach/age in years | GMFCS | MACS | CFCS | zajęta strona ciała/affected body side |
|---|---|---|---|---|---|---|
| 1 | M | 5,5 | I | II | I | P/R |
| 2 | M | 3 | I | II | I | P/R |
| 3 | M | 4 | I | II | I | P/R |
| 4 | M | 5 | I | I | I | P/R |
| 5 | M | 6 | I | II | I | P/R |
| 6 | M | 4 | I | II | I | P/R |
| 7 | K/F | 4,5 | I | II | I | P/R |
| 8 | M | 4,5 | II | I | II | P/R |
| 9 | M | 3 | II | III | III | P/R |
| 10 | M | 3,5 | I | II | I | P/R |
| 11 | K/F | 4,5 | I | I | I | P/R |
| 12 | M | 6 | II | II | II | L |
| 13 | M | 3 | II | III | III | P/R |
| 14 | M | 3,5 | I | II | I | P/R |
| 15 | K/F | 3,5 | I | II | I | L |
GMFCS, Gross Motor Function Classification System; MACS, Manual Ability Classification System; CFCS, Communication Function Classification System.
The therapy in “The Pirate Group” was conducted in the form of two-week camps, i.e. 10 days from Monday to Friday, for two hours per day. The first hour and a half was devoted CIMT, while the remaining half an hour was spent performing BIT. In CIMT, an unaffected upper limb (arm, forearm and hand) was restrained with a bandage. During a two-week camp in “The Pirate Group”, children were not taking part in any other form of therapy. During the therapy carried out in a specially arranged room, children performed activities connected, inter alia, with repairing a boat (painting sails, sawing planks, taking out old nails), sailing (hoisting sails, searching for a desert island through a field glass, washing the boat), self-care (putting on a pirate’s outfit, painting moustache and beard, preparing food for a trip). In order to ensure the best quality of the performed activities and depending on the situation, the therapists used wrist braces with thumb strap and kinesio taping. A detailed description of the procedure and organisation of the project “The Pirate Group” is included in the work by Beata Wnuk [33].
In total, 4 camps took place between March 2016 and April 2017. Children were working in the teams of four and each child had one therapist. All the therapists participating in the project were certified NDT-Bobath therapists. Activities were held in a specially arranged room adapted to the needs of the project in Olinek Intensive Therapy Centre.
At the beginning and at the end of the camp, each child underwent Assisting Hand Assessment (AHA), which made it possible to formulate individual goals of the therapy and to assess its effectiveness. AHA was carried out by an independent physiotherapist (not participating in the therapy) who was qualified for carrying out this test.
AHA test is a standardised tool for assessing arm function applied in children aged 18 months to 12 years with spastic hemiplegia or brachial plexus disorder. The aim of AHA is to measure and describe the effectiveness of using an affected limb as an assisting limb during bimanual activities. During a 15-20-minute test, the way in which a child is spontaneously playing with objects that require the use of both hands is assessed. The test is conducted in the form of a play and thus, children are eager to follow the therapist’s instructions without being forced to do so and their performance is spontaneous and natural, which makes it possible to assess the child’s real abilities [13,14,34,35].
In order to verify the effects of the therapy, Student’s T test (for dependent variables) was applied. Statistical analysis was performed with the use of Statistica 12 software.
On the basis of the statistical analysis, significant differences between the results of AHA conducted prior to and after the therapy were found (t(14)=9.12, p<0.0001). A mean improvement in logit scale for AHA units was 8.33 (SD=3.53).
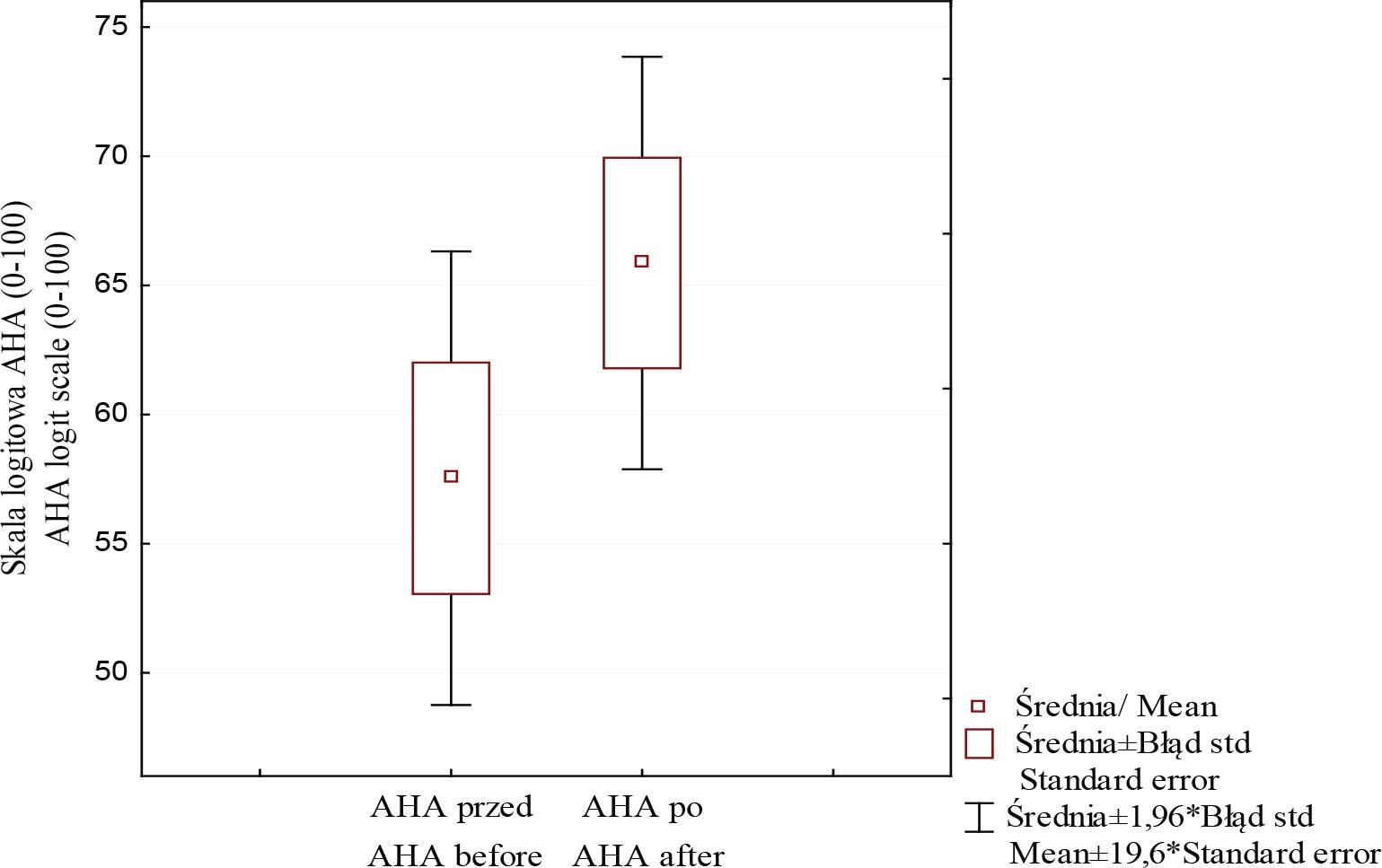
Comparison of mean results of AHA test before and after the therapy for the whole study group
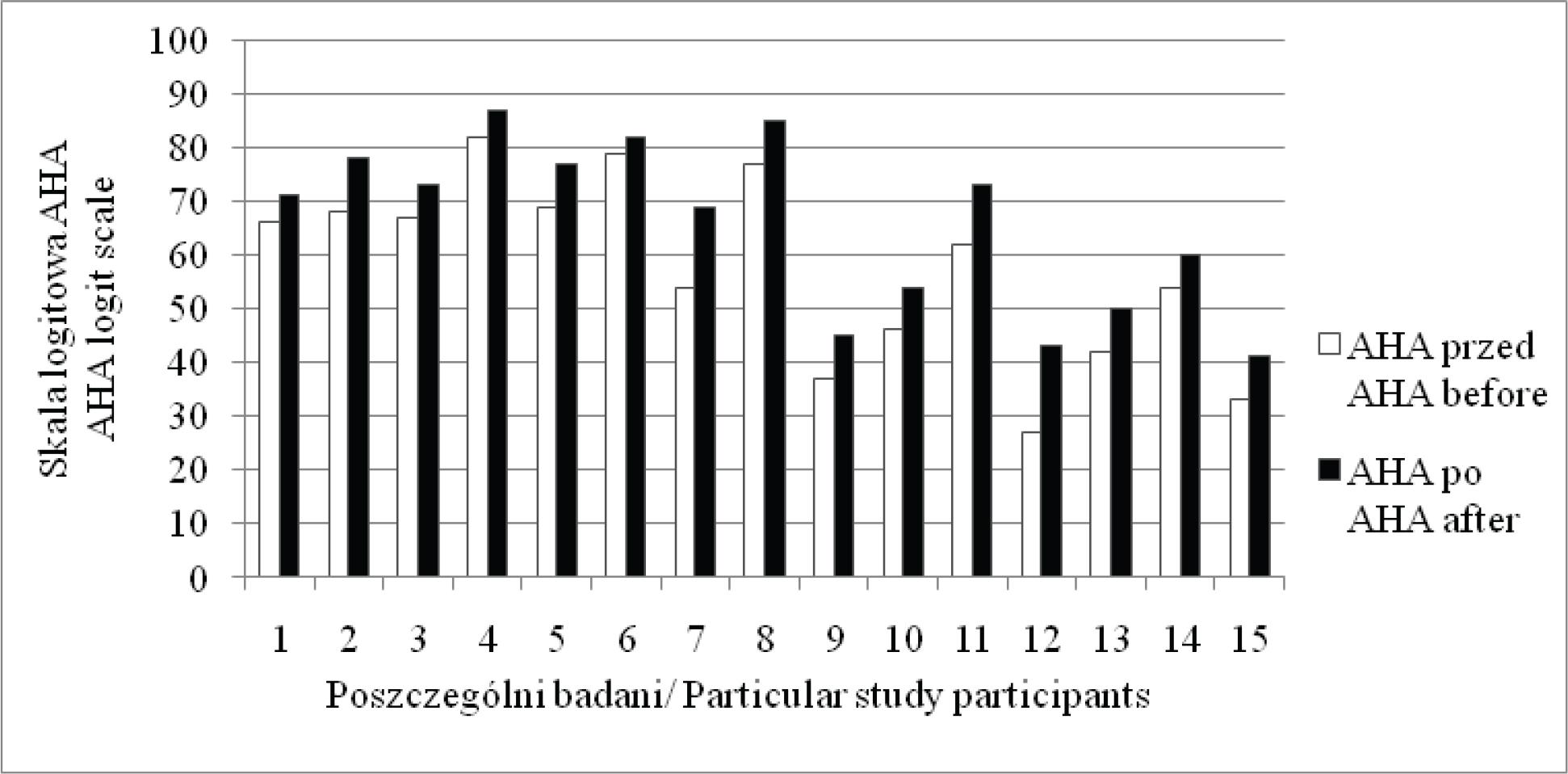
Results of AHA test before and after the therapy for particular study participants
An improvement in arm function in AHA test was noted in all the study participants.
No statistically significant correlations between the participants’ age and an improvement in arm function in AHA test were noted.
In recent years, numerous studies have been conducted which aimed at confirming the effectiveness of CIMT and BIT. However, it is not always easy to apply theory in practice.
The aim of our work was to verify whether the project “The Pirate Group” was an effective form of therapy of an upper limb in children with spastic hemiplegia.
The study revealed that a two-week camp in “The Pirate Group” based on CIMT and BIT led to an improvement (in quantitative and qualitative terms) in a spontaneous use of an upper limb in children with hemiplegia.
Through restraining a dominating upper limb as well as intensive training, children learned to use their affected limb more often and in a different manner than they did on an everyday basis. This improved the effectiveness of an assisting arm in such activities as moving an arm and forearm, holding and reaching for something, adjusting and releasing a grip or manipulating with objects.
These results are consistent with the findings of other researchers [16,21]. However, applying BIT every day was the main aspect that differed the project “The Pirate Group” from the studies by other authors who usually applied BIT after several weeks of CIMT.
Moreover, it is possible that a relatively short procedure (2 weeks, 2 hours per day, i.e. 20 hours of therapy) provided such satisfactory effects. The results of our research are similar to or even better than the results of other researchers [16,26,36,37], who applied much longer therapy CIMT-BIT (from 54 to 96 hours of therapy). According to the authors, it may be related to the fact that all the physiotherapists were certified NDT-Bobath therapists and focused not only on the amount but also on the quality of the performed activities. They paid attention and supported movement patterns and positions not only regarding fine but also gross motor skills, according to the guidelines of the NDT-Bobath concept. However, it would be worth conducting further research to find out what duration of the therapy in “The Pirate Group” would bring about the best effects.
“The Pirate Group” was a demanding environment for children with hemiplegia. It provided numerous challenges and difficult problems to solve and encouraged them to cooperate with peers. The fact that the therapy was conducted in the form of fun and play was a motivating factor for children participating in the project. Playing as well as working in pairs was a reinforcing factor which allowed them to overcome difficulties. What is really significant is that children did not show frustration or discomfort during everyday restraint of a dominating arm. The participants were eager to come to classes and could not wait for the next day. Parents informed us that children preferred the therapy in “The Pirate Group” to individual therapy which they attended prior to the camp. Moreover, parents also engaged in the therapy. Together with the therapists they participated in the process of selecting short-and long-term goals for their children. In addition, when provided with valuable suggestions (e.g. the selection of appropriate cutlery or orthopaedic equipment for an upper limb), parents implemented them immediately. Our observations were similar to the findings of Aarts [16].
Also, feedback from parents concerning changes which occurred during the camp, e.g. “Shin took a mug in both hands for the first time”, “For the first time, Max pushed a button in a lift with a finger of a spastic hand”, “Yesterday Gustaw peeled a banana without any help using both hands”, was very significant. An increased interest in an affected upper limb after CIMT conducted in home conditions was also noted by Rostami [38].
Preparing difficult but possible to perform tasks increased the children’s independence in everyday life, while achieving success increased their self-esteem. Similar findings were presented by Brito Brandao [23].
The environment created in the project “The Pirate Group” was also significant. Working in groups required certain social skills and good communication between the participants. Interactions between children increased their engagement, supported them and motivated them to work. This was also noted by other researchers in their studies [10,12,16,29,39].
Although the results are very promising, the research has certain limitations. One of them was a small number of participants. To date, 15 children have participated in the project “The Pirate Group” but further camps and studies with a bigger number of participants are planned. Another study limitation was the lack of control group. The research revealed that children participating in the camp achieved a considerable improvement of an affected upper limb; however, it would be worth comparing these results with a group of children attending mCIMT without such environment or without group therapy as in the “The Pirate Group”.
The therapeutic programme based on CIMT combined with BIT in the project “The Pirate Group” is an effective therapeutic intervention focused on a child and improving spontaneous activity of an affected upper limb in children with hemiplegia. The therapy in the form of fun and play motivates children to work and provides numerous challenges.