
Constipation is not defined as a disease but as a number of symptoms, such as decreased frequency of defecation (<3 x week), hard stools, obstructed defecation, defecating with an effort and the feeling of incomplete defecation. If a patient suffers from 3 of the aforementioned symptoms simultaneously, constipation is diagnosed [1].
According to epidemiological studies, this problem concerns 13.4% of the healthy population in Poland. Female gender (2:1) and age (>65 years) are factors predisposing to obstructed defecation [2]. In individuals with advanced cancer, it is the third most common symptom noted in 42-50% of the patients [3–6]. After the implementation of opioid treatment, it occurs in as many as 70-90% of the patients [3,4].
Apart from constipation, opioid treatment is accompanied by a number of symptoms in the digestive system, such as dry mouth, lack of appetite, gastroparesis, gastroesophageal reflux disease, abdominal cavity disorders and flatulence [7–9]. Apart from iatrogenic effects of pharmacological pain treatment resulting in weak peristalsis, secondary factors leading to constipation in the group of patients under palliative care include, inter alia, lower physical activity [5,10–12], limited amount of food and liquids intake, inadequate diet or the lack of intimacy and independence during defecation, which leads to ignoring the urge to defecate and, as a result, to constipation [5,6,13]. An inability to sit up, which is common among the patients of hospices, also leads to fecal loading [5,6,14–17].
Intervetions undertaken in the case of constipation may be divided into three groups, i.e. non-pharmacological (conservative), pharmacological and surgical ones [18,19]. Due to the area of interest of our study, mainly physiotherapeutic procedures being an element of conservative treatment of constipation are presented in our article. Experts dealing with the issue of constipation recommend an increase in physical activity and various forms of physiotherapy, regardless of its etiology [5,10,11,20]. The Polish Association of Palliative Care also recommends encouraging patients to take up physical activity and become more independent [16].
The process of defecation depends to a large extent on a proper function and strength of pelvic floor muscles, diaphragm and abdominal muscles which are indispensable for creating proper tension [21]. Therefore, kinesiotherapy includes the training of these muscles and the practice of diaphragmatic breathing [5,22].
The role of a physiotherapist is also significant when it comes to postural re-education during defecation and during everyday activities as it may facilitate the process of defecation [12]. If a sitting position is not possible, the patient should be taught to defecate in a supine position, particularly on the left side with a bent left lower limb [5].
In its recommendations, The Polish Association of Palliative Care treats education (information concerning the diagnosis, prophylactics, and treatment of constipation) as a precondition for succesful procedures in this area [14]. Therefore, following an inteview with a patient, a physiotherapist with broad knowledge about the treatment of constipation, may provide useful suggestions and implement a variety of procedures which facilitate defecating.
In the available literature there is a scarcity of studies analysing the application of abdominal massage in palliative care patients. There are reports on the effectiveness of this form of therapy in treating patients with multiple sclerosis [23], in neurogenic bowel management after spinal cord injury [18] and in chronic constipation [24]. The researchers unanimously concluded that this procedure reduced discomfort and pain as well as bowel transit time, and it also stimulated bowel peristalsis and at the same time increased the frequency of defecation. Moreover, the application of abdominal massage aimed at facilitating digestion and excretion in preterm infants is commonly known [25]. The available literature also includes reports on attempts at applying abdominal massage with the use of mechanical devices in patients with spinal cord injuries. However, contrary to manual massage, these attempts were not well tolerated by the study participants [26].
Due to an increasing life expectancy of cancer patients, there is a growing need for proper care and prevention of disorders connected with obstructed defecation, particularly in the final stage of the disease [27]. The aim of our study was to assess the effects of abdominal massage, which successfully reduces constipation in various diseases, on palliative care patients.
The research included 18 patients of a hospice in Warsaw (mean age 78.1 ± 10 years). The study participants were randomly (by assigning numbers) divided into two groups, i.e. a pilot group – patients with uneven numbers (M-massage, n=9), who were treated with kinesiotherapy and abdominal massage, and a control group – patients with even numbers (NM-no massage, n=9) who were treated with kinesiotherapy only. However, due to the progression of cancer and long duration of the study (8 weeks), complete study documentation could be obtained only in the case of 11 patients (6 women, 7 men – mean age 78.3 ± 10 years). Therefore, final statistical analysis was conducted in two groups: the pilot group (M, n=6) and the control group (NM, n=5).
The main cause of constipation found by the doctor in all the study participants was a long-term use of opioids and limited physical activity (bedridden patients). In the patients qualified for the study, the symptoms of constipation persisted despite a longterm use of osmotic and laxatic drugs. During the study, the doses or types of drugs were not changed. All the patients were able to eat without support and to perform some minor activities on their beds; however, they were not able to change their position into sitting independently or to maintain a sitting position.
Each time, the head of the palliative care facility as well as the patients and doctors gave their written consent to participate in the study. Therapeutic interventions were conducted with proper care and in compliance with ethical standards regarding studies on human participants.
The inclusion criteria were as follows: conscious and voluntary consent to participate in the study, estimated survival time >14 days and the occurrence of three of the following elements constituting the definition of constipation: frequency of defecation <3 times per week, hard stools, defecating with an effort, the feeling of incomplete defecation, obstructed defecation.
The following individuals were excluded from the study: patients with limited contact skills, patients in agonal state, patients with counterindications to abdominal massage (abdominal surgeries or radiotherapy less than 6 weeks before), as well as patients with intestinal obstruction and inflammation or disorders of unknown etiology in the abdominal cavity [5].
Therapeutic procedures in both groups were carried out by one physiotherapist in the period of 8 subsequent weeks. The procedures were performed in the morning, as at this time of the day the activity of digestive system is at its peak [5]. Abdominal massage, an activity which did not require any input from the patient, was given 7 days a week, 15 minutes a day. Kinesiotherapeutic exercises were implemented 5 days a week (15 minutes a day) due to their relatively active character and the feeling of fatigue accompanying cancer. Kinesiotherapy was conducted in the same manner in both groups and was based on active-passive and active exercises aimed at activating the bedridden patient, activating abdominal and limb muscles and teaching the patient proper diaphragmatic breathing.
Abdominal massage involved manual stimulation of large intestine aimed at regulating myofascial tension in the abdominal area, boosting bowel peristalsis and helping fecal mass transfer towards rectum. The procedure was divided into three subsequent 5-minute phases (fig. 1) which were performed according to the direction of the digestive system, i.e. I – normalisation of muscular tension of abdominal cavity organs, II – mechanical stimulation aimed at transferring fecal loading from large intestine (descending colon, transverse colon, ascending colon), III – relaxation [5].
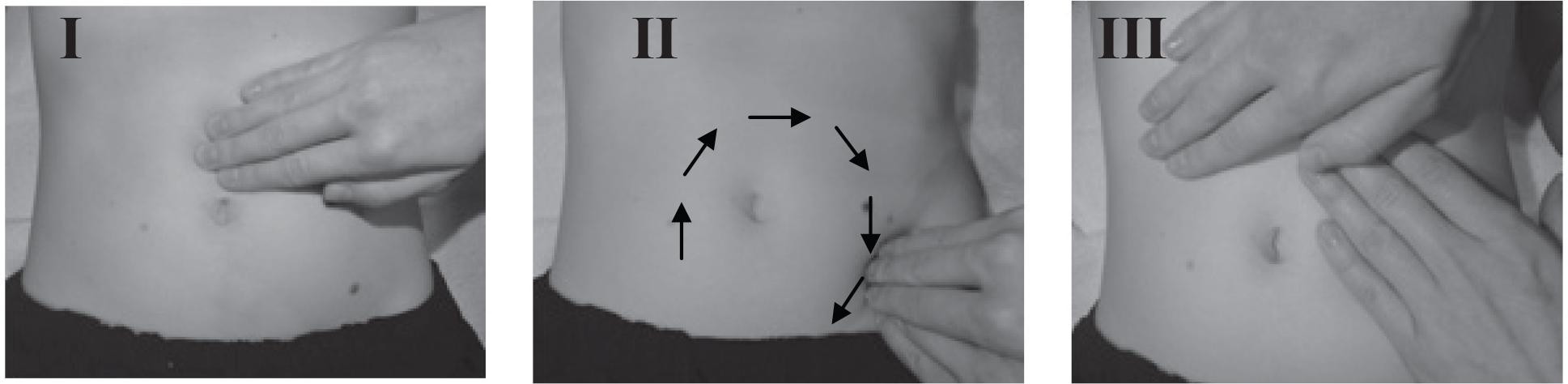
Abdominal massage phases I-III (arrows show the direction of the procedure)
The intensity of constipation was assessed on the basis of the Bowel Function Index (BFI) [28]. The frequency of defecation was analysed with the use of medical documentation. Abdomen circumference was measured with anthropometric tape (1 mm accuracy) placed at the level of the umbilicus of a patient in a supine position with extended lower limbs. It was also monitored whether the patients consumed all the meals and liquids planned in their diet.
The same tools were applied in both groups. The measurements were made once per week on the same day in the whole study period. In order to avoid the influence of the bond between a patient and a therapist/researcher on the assessment of the treatment effectiveness [29, 30] and to exclude confirmation error associated with the researcher, third persons were asked to collect the completed questionnaires and to evaluate the obtained results.
The BFI was selected due to its simplicity and clarity for a patient and because of its confirmed validation [31]. The questionaire assessed three elements (max. 10 points each), i.e. obstructed defecation, the feeling of incomplete defecation and intensity of constipation. A lower mean of points meant lower intensity of the disorders. The mean value >2.9 indicated constipation, the result ≤2.9 constituted the norm, while a change of a mean value by 1.2 or more meant a significant change in the intensity of constipation [32].
The collected data were analysed statistically with the use of Statistica software. The calculated values included means, standard deviations and percentage differences, where the results of the first measurement were treated as 100%. The comparative analysis of both groups was performed with the use of ANOVA for repeated measures. The type and duration of the applied therapy were factors taken into account in the analysis. In order to assess detailed differences, the Tukey’s Unequal N HSD test was applied.
On the basis of the statistical analysis of the values of abdomen circumference, no effects of interaction between the duration and type of the applied therapy were revealed (F(7.14) =0.44; p=0.864). A positive percentage difference between abdomen circumference in the 1st and 8th week of the therapy in the group with massage was not statistically significant (Tab. 1).
Mean ±SD values of abdomen circumference [cm] obtained in subsequent weeks in the groups with massage (M, n=6) and without massage (NM, n=5)
| OBWÓD BRZUCHA/ABDOMEN CIRCUMFERENCE [cm] | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TYDZIEŃ/WEEK | ||||||||||||
| I | II | III | IV | V | VI | VII | VIII | RÓŻNICA/DIFFERENCE I-VIII [%] | Fdf=7,14 | P | ||
| M/M | 110,0 | 107,8 | 106,0 | 105,2 | 104,3 | 103,5 | 104,0 | 104,0 | 5 | 0,44 | 0,864 | |
| SD | 11,3 | 8,2 | 10,6 | 9,7 | 10,6 | 10,1 | 11,4 | 11,4 | ||||
| BM/NM | 88,0 | 96,6 | 95,4 | 96,0 | 98,2 | 98,0 | 94,8 | 104,8 | -18,2 | |||
| SD | 23,5 | 21,3 | 20,2 | 20,3 | 19,4 | 20,0 | 20,7 | 13,9 | ||||
An increase in the frequency of defecation in the group with massage observed in subsequent weeks with a simultaneous decrease in its frequency in the group without massage did not reach the level of statistical significance (Tab. 2). However, in this case, a certain tendency can be noted (p=0.081).
Mean ±SD values of the number of defecations obtained in subsequent weeks in the groups with massage (M, n=6) and without massage (NM, n=5)
| LICZBA WYPRÓŻNIEŃ/NUMBER OF DEFECATIONS | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TYDZIEŃ/WEEK | ||||||||||||
| I | II | III | IV | V | VI | VII | VIII | RÓŻNICA/DIFFERENCE I-VIII [%] | Fdf=7,14 | P | ||
| M/M | 3,3 | 3,0 | 3,5 | 4,3 | 3,7 | 4,7 | 4,8 | 4,6 | -38 | 2,36 | 0,081 | |
| SD | 2,3 | 0,7 | 0,5 | 1,5 | 1,6 | 0,8 | 1,3 | 1,1 | ||||
| BM/NM | 2,7 | 2,2 | 2,8 | 2,4 | 2,6 | 2,6 | 1,8 | 1,3 | 50 | |||
| SD | 2,1 | 1,6 | 1,3 | 1,5 | 1,5 | 1,3 | 1,0 | 0,6 | ||||
The comparative analysis of both groups did not reveal statistically significant differences between therapy type and duration and mean values obtained by the study participants in particular elements of BFI (Tab. 3). However, there occurred a considerable percentage difference between the first and the last measurement in the group with massage, which pointed to the a final decrease in defecation disorders. Moreover, in this group, almost every week, a gradual decrease in the values of particular elements of BFI compared to the previous week was observed.
Mean ±SD values of particular elements of BFI obtained in subsequent weeks in the groups with massage (M, n=6) and without massage (NM, n=5)
| INDEKS CZYNNOŚCI JELIT – SKŁADOWE [pkt]/BOWEL FUNCTION INDEX (BFI) – ELEMENTS [pts] | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SKŁADOWA A/ELEMENT A | TRUDNOŚĆ WYPRÓŻNIANIA/OBSTRUCTED DEFECATION | |||||||||||
| TYDZIEŃ/WEEK | ||||||||||||
| I | II | III | IV | V | VI | VII | VIII | RÓŻNICA/DIFFERENCE I-VIII [%] | Fdf=7,14 | P | ||
| M/M | 7,3 | 6 | 4,7 | 3,2 | 2,7 | 1,5 | 1,2 | 1 | 86 | 2,11 | 0,112 | |
| SD | 2,1 | 4,3 | 2,3 | 3 | 2 | 1,8 | 1,1 | 1,4 | ||||
| BM/NM | 6 | 4,6 | 6,2 | 4,8 | 4,2 | 5,2 | 6 | 6,3 | -5,56 | |||
| SD | 3,6 | 4 | 2,9 | 3,8 | 3,2 | 1,8 | 1,4 | 3,8 | ||||
| SKŁADOWA B/ELEMENT B | POCZUCIE NIEPEŁNEGO WYPRÓŻNIENIA/FEELING OF INCOMPLETE DEFECATION | |||||||||||
| TYDZIEŃ/WEEK | ||||||||||||
| I | II | III | IV | V | VI | VII | VIII | RÓŻNICA/DIFFERENCE I-VIII [%] | Fdf=7,14 | P | ||
| M/M | 7,7 | 6 | 4,7 | 2 | 1,3 | 0,8 | 0,4 | 0,6 | 92 | 2,32 | 0,085 | |
| SD | 2,3 | 4,3 | 3 | 3,1 | 1,8 | 1,3 | 0,9 | 0,9 | ||||
| BM/NM | 6 | 2,8 | 4,8 | 4,6 | 4,6 | 5,6 | 6,8 | 6,7 | -11,1 | |||
| SD | 2,6 | 3,1 | 2,2 | 3,2 | 2,9 | 3 | 2,2 | 3,2 | ||||
| SKŁADOWA C/ELEMENT C | OCENA CIĘŻKOŚCI ZAPARCIA/CONSTIPATION INTENSITY | |||||||||||
| TYDZIEŃ/WEEK | ||||||||||||
| I | II | III | IV | V | VI | VII | VIII | RÓŻNICA/DIFFERENCE I-VIII [%] | Fdf=7,14 | P | ||
| M/M | 6,7 | 5,4 | 5,7 | 3 | 1,5 | 1,8 | 1,2 | 0,6 | 91 | 1,34 | 0,303 | |
| SD | 2,3 | 4,2 | 2,7 | 3,2 | 2,3 | 1,8 | 1,3 | 0,5 | ||||
| BM/NM | 4,7 | 3,6 | 5,6 | 3,8 | 5 | 5,8 | 5,5 | 5,3 | -14,3 | |||
| SD | 2,1 | 3,8 | 1,5 | 3,2 | 2,3 | 3,1 | 2,4 | 3,1 | ||||
The analysis of changes in the total mean value of all the elements of BFI did not reveal statistical significance (p=0.091) (fig. 2). However, it should be pointed out that from the 5th week a clear tendency indicating a gradual decrease in the symptoms of constipation (lower BFI) was noted in the group with abdominal massage with a simultaneous increase in these symptoms in the group without massage.
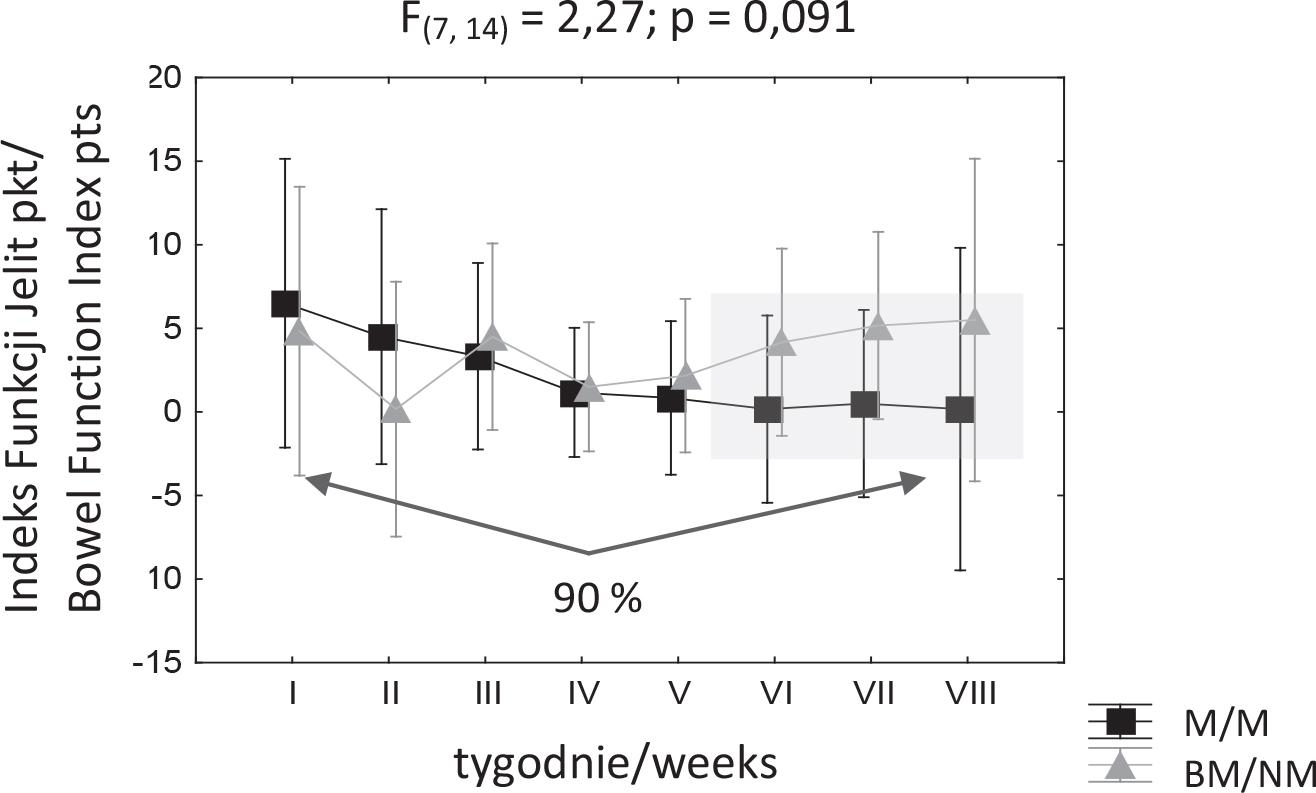
Mean ±SD values of the Bowel Function Index [pts] obtained in subsequent weeks in the groups with massage (M, n=6) and without massage (NM, n=5)
Apart from the data directly regarding the problems with defecating, an issue of nutrition was also taken into account in the measurements. The question related to drinking additional liquids was answered negatively by 100% of the patients. The question whether the patients consumed all the meals planned in their diet was answered positively by 100% of the study participants.
Apart from using objective measurement tools in the study, the patients’ comments regarding their subjective feelings connected with defecating were collected. After abdominal massage, the patients usually reported an improvement in breathing (lightness), reduced abdominal pain, easier urination and releasing gas. Several patients reported diarrhoea. The patients’ original comments were as follows: “it’s easier to breathe”, “the pain is not as strong as before the massage”, “I’ve got abundant loose stools”, “I defecated during the massage with releasing gas and belching”, “you’ve managed to do something that nobody had ever been able to do!”, “unfortunately, I have a diarrhoea”, “I feel less pain in the ribs area”, “together with an improvement in defecating, I started urinating without pain”.
In subsequent weeks, clear changes were also noted in palpation examination, e.g. better abdominal wall flexibility and improved mobility of soft tissues. In the final weeks of the therapy also fecal mass, which, at the beginning, could be located palpably and which was very hard, was no longer palpable. Moreover, pain which sometimes occurred during abdomen palpation also ceased.
Patients under palliative care constitute a specific group in which it is difficult to conduct research due to a progressive type of a disease [29]. Also, the range of therapeutic procedures which can be applied in this population is considerably limited. Therefore, any attempts at transferring various treatment methods that could help to alleviate health problems in this group seem to be worthy. The few publications available on the subject prove an innovative character of the presented research, indicate its justifiability and at the same time make it difficult to compare the findings with observations of other researchers.
The review of the literature made it possible to conclude that abdominal massage is a form of therapy which is successfully applied in preventing constipation in elderly individuals as well as in patients with multiple sclerosis, Parkinson’s disease and spinal cord injuries. The latest research in this field indicated its effectiveness in treating chemotherapy-induced constipation in patients with breast cancer [33]. Moreover, attempts were made at implementing abdominal massage as a method of preventing ventilator-associated pneumonia in enterally-fed patients of intensive care unit [34]. This study seems to be particularly significant in the case of patient care in the final stage of a disease. The pilot study which confirmed a decrease in the symptoms of constipation after abdominal massage with aromatherapy in Asians in an advanced stage of cancer is also worth noting [35].
Our research also indicated positive effects of abdominal massage on patients treated at a palliative care facility, although it should be pointed out that the observed changes were only close to reaching the level of statistical significance. Therefore, they can only be treated as tendencies. A small number of participants could be a factor determining the observed level of significance. However, it is worth pointing out the fact that in the case of the group with abdominal massage, the changes in the majority of the measurements were positive, in contrast to the group without massage in which disorders did not change or increased in intensity. This trend can be clearly noted in the mean value of the Bowel Function Index (fig. 2), which reflected an increase in constipation. Although, in terms of statistics, only a tendency could be noted, available reports showed that a change in the mean BFI value by 1 or 2 points indicates a significant difference in the intensity of constipation [32]. In our study, this difference exceeded this value considerably (fig. 2), which may indicate a decrease in the symptoms of constipation in the group with massage.
This thesis also seems to be confirmed by subjective opinions of patients who received a massage. They noticed an improvement in the quality of defecating and experienced a reduced feeling of discomfort and pain in the abdomen, releasing gases and easier breathing. Taking into account the aspect of ventilation seems to be particularly significant in the context of future studies.
With the use of an interview as a research tool, other researchers made similar observations regarding individuals with intellectual disabilities [36] and Parkinson’s disease [36]. In the interviews, study participants indicated the fact that the frequency and ease of defecation increased and their mood improved after abdominal massage [36,37]. In our study, the patients’ remarks concerning an improvement in urinating as a “side effect” of the therapy seemed interesting as well. Manual work on the visceral system may have led to rebalancing pressure in the abdominal cavity, which, at the same time, facilitated urination. This may be proved by increased flexibility of abdominal wall. Therefore, assessing the flexibility of abdominal wall may serve as a better measurement of the effectiveness of the therapy, as the measurements of abdomen circumference did not reveal statistically significant differences but only a decreasing tendency in the group with massage (Tab. 1). Easier urination may also be explained with general effects of abdominal massage, which, apart from mechanical activity, may regulate the work of the autonomous system [36].
Positive remarks of the patients regarding their subjective feelings after massage indicated the need for adding the quality assessment in the future research. The analysis of constipation in an individual context is also in line with the suggestion put forward by Böhmer [38], who defined it as a subjective feeling based on individual perception of changes experienced with regard to the normal bowel function.
In the period during which abdominal massage was applied, the 5th week appeared to be particularly significant. Mean BFI (fig. 2) in the 5th week clearly improved in the group with massage with a simultaneous decrease in the quality of defecation in individuals without massage. This tendency continued in the next weeks until the completion of the study, which may indicate that 5 weeks is a minimal period after which certain effects can be expected. In the available literature, various periods of massage application can be noted depending on the disease in which constipation occurs, e.g. 6 weeks in the Parkinson’s disease [37], 10 weeks in spinal cord injuries and chronic bowel dysfunction [26] and 6 months in the case of intellectual disability [36]. Moreover, the frequency and duration of particular procedures vary, e.g. 1 min./10 times a day – patients with breast cancer after chemotherapy [33], 10 min./once a day – patients with Parkinson’s disease [37], 15 min./twice a day – mechanically ventilated patients [34]. It is hard to conclude unanimously how long it would be necessary to massage palliative care patients in order to achieve the desired effects. The frequency and regularity are significant [36]. During our research, a few patients reported diarrhoea, which may indicate that massage received 7 times a week constituted a stimulus which was too strong for the digestive system. The aim of the future research will be to determine the minimal duration of the therapy which will bring about the desired effects and to define optimal frequency of the procedures.
During our research, an increase in the frequency of defecation was also noted in contrast to the group without massage, where a decrease or an unchanged level of the frequency of defecation was noted (Tab. 2). However, these differences were not statistically significant although the observed changes were in line with the findings of McClurg et al. [23] in their randomised study on 15 patients with MS who manifested a significant increase in the number of defecations after abdominal massage.
The literature of the subject points to the consumption of an insufficient amount of liquids, improper diet and the lack of physical activity as the main risk factors of constipation [5,10,11,13,16]. The patients in both groups had the same diet and the meals were provided regularly at the same hours. The level of mobility of the patients included in the study was also similar, as all of them moved only on their beds and were not able to sit up. This state did not change in the whole period of the research, so it may be assumed that neither factor affected the obtained results.
The observed tendencies indicating a decrease in the symptoms of constipation and subjective feeling of constipation in the group with abdominal massage as well as additional positive effects occurring during and after the massage make it possible to assume that applying this type of intervention in the case of problems with defecation is justified.
To sum up, it is worth noting that the problem of constipation regards a considerable number of hospice patients and therefore, abdominal massage, as an additional, non-invasive form of suppotive treatment seems to be a noteworthy tool in palliative care [24]. It is also worth pointing out that both patients and their caretakers indicated a high level of satisfaction with this form of therapy [33,36]. The study participants also mentioned the simplicity of the procedure and the possibility to perform it independently by a patient or caretaker after receiving proper instructions and watching recommendations on DVD [36,37]. It provides an opportunity to continue physiotherapeutic procedures which may bring significant profits in long-term prevention of constipation. Effective application of abdominal massage may also reduce the costs of treatment by decreasing the amount of administered medications.
The study was carried out on a small number of participants; however, it may constitute a basis for creating a research project taking into account a bigger sample size. In the future, it may allow us to confirm the tendencies noted in the pilot study. Due to the lack of possibility to control certain variables and their large number (speed of disease progression, necessity to change medications) in the case of patients in an advanced stage of cancer, it is not possible to predict their influence on the obtained results, which may disturb the clinical image. It is also significant to keep a register of subjective feelings of a patient connected with procedures and defecation, consumed and excreted liquids as well as consumed products that were not included in the planned diet. Regardless of their character (active, passive), the number of intervenions per week should be made uniform.
Owing to the fact that the literature lacks in studies on the possibility to apply abdominal massage as a method of preventing constipation in patients in an advanced stage of cancer, an attempt was made at exploring this issue. On the basis of the literature review, it may be assumed that it is the first study of this type conducted in a palliative care facility, which points to an innovative character of the presented pilot study. Our experiment made it possible to define research areas and potentially weak points which should be taken into account when planning further projects. A random selection of the study participants to particular groups, the application of a single-blind study method, a prospective character of the study and a long period of intervention undoubtedly prove the value of the work. Despite the fact that only certain tendencies regarding the effects of abdominal massage on the symptoms of constipation were noted, the study constitutes a significant attempt at enriching physiotherapeutic procedures, which are limited in the case of palliative care patients, with further tools helping to alleviate health problems in this specific group of patients.
The presented research material was a pilot study, so caution is advised when drawing conclusions. However, it is worth pointing out that the results are promising. On the basis of the research material analysis, following conclusions may be drawn:
Abdominal massage may lead to the subjective feeling of a decrease in disorders connected with opioid-induced constipation.
It is worth considering the implementation of this form of therapy in the case of patients in the advanced stage of cancer.
There is a need for further research in this field which will include a larger number of patients.