
The hip joint affects a proper control of body posture and human locomotion. An improper development of the hip joint may lead to numerous unfavourable changes in the musculoskeletal system such as pain, decreased muscle strength, uneven lower limbs, degenerative hip disease, gait disorders and changes in body posture [1–4].
Anomalies of the hip (AH) diagnosed in the in-fancy period may have various forms. Early diagnosis is conducted in order to determine developmental dysplasia of the hip (DDH). DDH manifests itself with an improper shape and a disturbed spatial orientation of the head of the femur and/or acetabulum [5]. This term defines various changes in the hip such as sublocation, dislocation or instability [6–9]. The frequency at which clinical symptoms of DDH are diagnosed may vary from 0.04% to 16.8% [10]. It depends, inter alia, on the adopted definition, criteria and methods of diagnosing, experience of the examiner, age and sex of children participating in the study or geographical location of the country in which the study was conducted [8,10–12]. Approximately 80% of the cases of the DDH are diagnosed in girls [5,7,10].
Dysplasia and other anomalies of the hip in the neonatal and infancy period are diagnosed on the basis of clinical, ultrasonographic or radiological examinations [3,4,10–18]. Clinical examinations include manual tests, an assessment of the ranges of motion in hip joints and the evaluation of body posture symmetry. Distressing symptoms include asymmetry or abducting movement limitation, differences in the length of lower limbs, asymmetry of gluteal and femoral folds and oblique pelvis position [5,12,17,19–21]. In the conservative treatment of DDH, hip orthoses are applied [22]. Physiotherapy may exert a positive influence on the build and function of a dysplastic hip [23].
Treatment and prophylactic activities should be applied not only to newborns and infants with DDH but also to those with hip movement limitations and accompanying asymmetry [21,24,25]. Numerous authors noted the correlation between the motor function of the hip and an improper build or position of other parts of the body [21,24,26–37]. It was noted that DDH is connected with congenital torticollis and plagiocephaly [21,27–36] and with a clubfoot [37]. In turn, the research which included pre-school and school children revealed that DDH predisposes them to occlusal asymmetry [35]. In other studies, attention was also drawn to the correlation of hip mobility dysfunction and scoliosis diagnosed at a later development stage [25,38–40]. It was also highlighted that maintaining a proper and symmetric range of motion in the hip is indispensable for avoiding an improper three-dimensional position of a lumbo-pelvic-hip complex [25]. The above-mentioned studies indicated the existence of certain cause-and-effect relationships between an improper structure and motor function of the hip, body asymmetry and scoliosis; however, to date, it has not been scientifically proven.
The aim of this research was to determine how often girls and boys with adolescent idiopathic scoliosis and their healthy counterparts experienced anomalies of the hip (AH) in their infancy period and to examine the correlation between the occurrence of AH and idiopathic scoliosis (IS).
The study was approved by the Senate Research Ethics Committee of the University of Physical Education in Warsaw (SKE 01-07/2016; 10.03.2016). The 3-month study was conducted in 2016 in two hospitals and four out-patient healthcare centres specialising in the conservative treatment of children and youth with scoliosis as well as in two primary schools and one lower-secondary school. The schools were located in the vicinity of the health centres and hospitals. The research included parents/guardians of girls and boys with idiopathic scoliosis and parents of healthy adolescents. They completed a short questionnaire on the basis of their child’s development history included in the medical records book and information from medical documentation possessed by parents/guardians.
Physiotherapists working with the youth with IS in the specialist healthcare centres provided the questionnaire to parents/guardians and asked them to complete it. At schools, the research was carried out in close cooperation with school directors and teachers. Parents/guardians completed the questionnaire during a parents’ meeting at school or at home if they did not have the medical records book with them. The participation in the study was voluntary. Parents/guardians were informed about the aims of the research, and gave their consent to take part in the study and to use information provided in the questionnaire except for personal data.
The questionnaire included questions regarding a child’s age and sex, type of delivery, diagnosed anomalies of the hip such as diagnosed dysplasia, limitations or asymmetry of the range of motion and the occurrence of scoliosis at a later development stage confirmed with an X-ray (Figure 1).
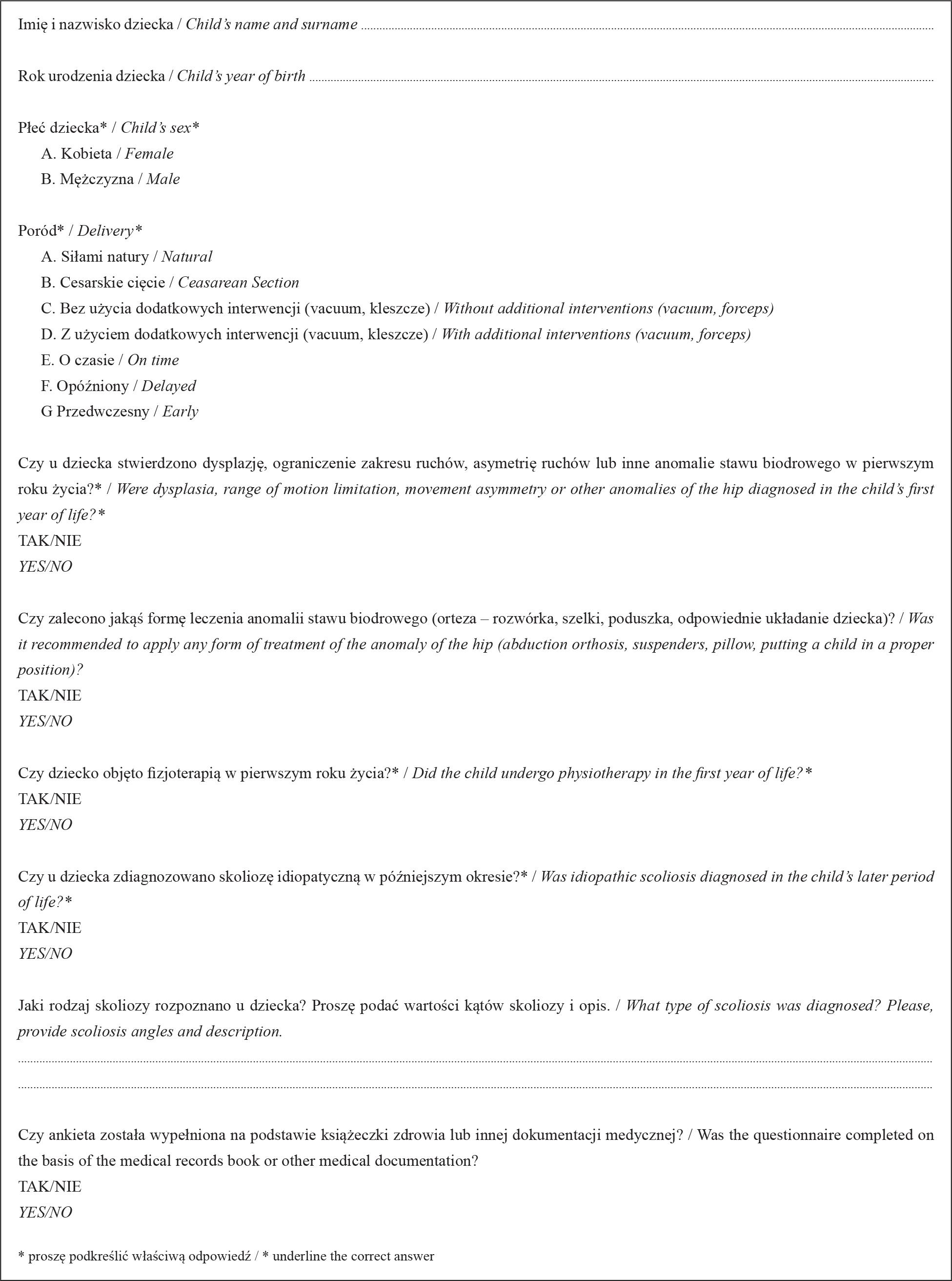
A questionnaire completed by parents/guardians of adolescents with and without idiopathic scoliosis
The study inclusion criteria were as follows:
- –
age 10-16 years;
- –
sex – boys and girls;
- –
good general health;
- –
the confirmation of the agreement of data provided in the questionnaire with information included in the medical records book or in other medical documentation;
- –
providing answers to questions concerning age, sex, the occurrence of AH in the first year of life, conservative treatment of the hip, implemented physiotherapy and the occurrence of IS;
- –
in the case of individuals who were diagnosed with IS – the value of Cobb angle min. 100.
The questionnaires lacking information regarding the delivery were accepted for the analysis.
The analysis did not include the questionnaires which:
- –
regarded children under 10 years of age or youth over 16 years of age;
- –
lacked information regarding age, sex, the occurrence of AH, applied hip treatment, physiotherapy in the first year of life;
- –
lacked data regarding the level of scoliosis and information on the occurrence of scoliosis type other than idiopathic one;
- –
included information on the scoliosis angle lower than 100.
In order to define the incidence of AH, two groups were created, i.e. an idiopathic scoliosis group (ISG) and a control group (CG). Taking into account the fact that both DDH [5, 7, 10] and IS [41] are diagnosed several times more often in girls than in boys, statistical analysis in each of the groups was conducted with regard to sex.
Statistical analysis was performed with the use of PQ Stat Version 1.6.2 software. In order to assess whether there exists a significant difference between the groups regarding the incidence of DDH, the percentage profiles were analysed in contingency tables with the use of Pearson chi-square test. Also, Cramer’s coefficient (V) providing information concerning the strength of the correlation between the selected variables was calculated. The significance level was set at α=0.05.
The research included 723 parents/guardians of children and youth with idiopathic scoliosis and their healthy counterparts. The analysis did not include 187 questionnaires (out of 723) which did not meet the inclusion criteria (Figure 2).
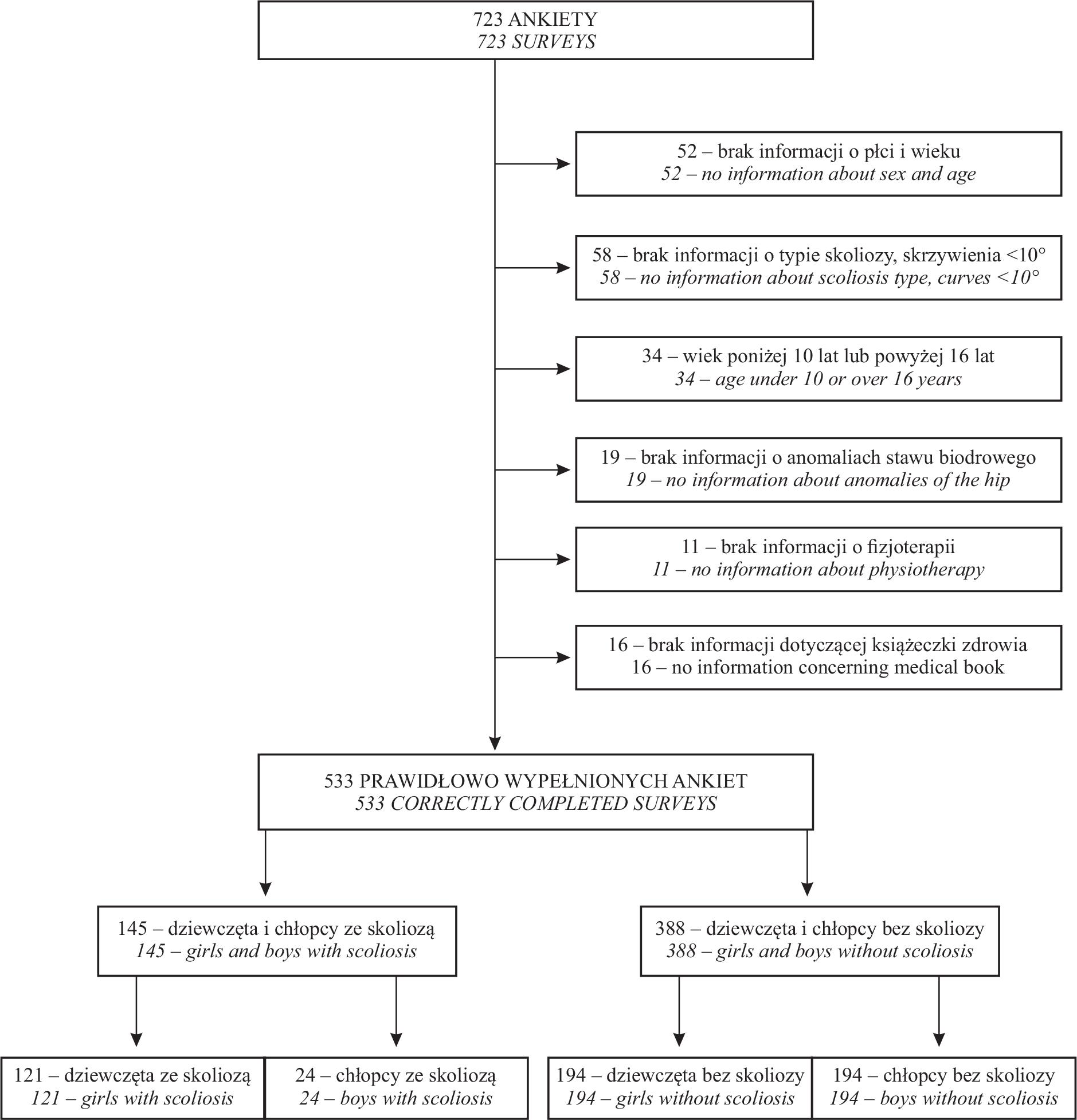
Qualification of the surveys completed by parents/guardians of adolescents with and without scoliosis
In the final analysis, 533 questionnaires were taken into consideration. These included 145 questionnaires completed by parents/guardians of children and youth with scoliosis and 388 questionnaires from the control group of the youth without scoliosis.
The ISG included 121 girls (mean age 13.8 years, SD 1.9) and 24 boys (mean age 12.9 years, SD 2.5). In this group, 51 individuals (35.2%) had single scoliosis, while 94 patients (64.8%) had double scoliosis. Information on the type and size of the curvature in the group of girls and boys with scoliosis is included in Table 1.
Characteristics of scoliosis in the group of girls and boys
| Skolioza | Częstość występowania | Kat Cobba, min, max | ||
|---|---|---|---|---|
| Dziewczęta | Jednołukowa | Piersiowa, lędźwiowa lub piersiowo-lędzwiowa | 30,6% | =19,5° (SD 10,2°); min 10°, max 51° |
| Dwułukowa | Piersiowa | 69,4% | =25,0° (SD 10,9°); min 10°, max 50° | |
| Lędźwiowa lub piersiowo-lędźwiowa | =23,4° (SD 9,5°); min 10°, max 50° | |||
| Chłopcy | Jednołukowa | Piersiowa, lędźwiowa lub piersiowo-lędzwiowa | 58,3% | =14,9° (SD 4,9°); min 10°, max 24° |
| Dwułukowa | Piersiowa | 41,7% | =30,0° (SD 11,9°); min 16°, max 55° | |
| Lędźwiowa lub piersiowo-lędźwiowa | =25,5° (SD 7,6°); min 14°, max 35° | |||
The control group (CG) included 194 girls (mean age 13.5 years, SD 2.0) and 194 boys (mean age 13.4 years, SD 2.1) without scoliosis.
The examined groups (ISG and CG) were uniform in terms of age and sex. Also no differences regarding the type of delivery between ISG and CG were noted.
No significant differences were noted in the groups of girls and boys with and without scoliosis in terms of the incidence of AH and no correlation between AH and scoliosis was found. (Table 2, Table 3).
Diagnosis of anomalies of the hip and the occurrence of scoliosis in the group of girls (AH – anomalies of the hip, ISG – idiopathic scoliosis group, CG – control group, n – number of participants)
| AH | Grupa | Ogółem | |
|---|---|---|---|
| ISG dziewczęta | CG dziewczęta | ||
| Brak | 85,12% | 88,66% | 87,30% |
| Występowały | 14,88% | 11,34% | 12,70% |
| Ogółem | 100% | 100% | 100% |
| χ2=0,840; p= 0,36 | V Cramera Cramer V=0,052; p= 0,36 | ||
Diagnosis of anomalies of the hip and the occurrence of scoliosis in the group of boys (AH – anomalies of the hip, ISG – idiopathic scoliosis group, CG – control group, n – number of participants)
| AH | Grupa | Ogółem | |
|---|---|---|---|
| ISG chłopcy | CG chłopcy | ||
| Brak | 91,67% | 96,39% | 95,87% |
| Występowały | 8,33% | 3,61% | 4,13% |
| Ogółem | 100% | 100% | 100% |
| χ2=1,205; p=0,27 | V Cramera Cramer V=0,074; p=0,27 | ||
The frequency of the application of treatment in the form of orthosis or preventive care (putting a child in a proper position) in the girls and boys with scoliosis and control groups did not differ significantly (Table 4, Table 5).
The treatment of anomalies of the hip and the occurrence of scoliosis in the group of girls (AH – anomalies of the hip, ISG – idiopathic scoliosis group, CG – control group, n – number of participants)
| Leczenie AH | Grupa | Ogółem | |
|---|---|---|---|
| ISG dziewczęta | ISG dziewczęta | ||
| Brak | 81,82% | 73,71% | 76,83% |
| Podjęto leczenie lub profilaktykę | 18,18% | 26,29% | 23,17% |
| Ogółem | 100% | 100% | 100% |
| χ2=2,751; p=0,09 | V Cramera Cramer V=0,093; p=0,09 | ||
The treatment of anomalies of the hip and the occurrence of scoliosis in the group of boys (AH – anomalies of the hip, ISG – idiopathic scoliosis group, CG – control group, n – number of participants)
| Leczenie AH | Grupa | Ogółem | |
|---|---|---|---|
| ISG chłopcy | ISG chłopcy | ||
| Brak | 91,67% | 82,47% | 83,49% |
| Podjęto leczenie lub profilaktykę | 8,33% | 17,53% | 16,51% |
| Ogółem | 100% | 100% | 100% |
| χ2=1,309; p=0,25 | V Cramera Cramer V=0,077; p=0,25 | ||
Physiotherapy in the first year of life was implemented more often among children with hip dysfunction than in the case of healthy children (Table 6); however, this difference was not statistically significant.
Physiotherapy in the first year of life and the occurrence of anomalies of the hip
| Fizjoterapia | Osoby z anomaliami stawu biodrowego (AH) | Osoby bez anomalii stawu biodrowego (AH) | Ogółem |
|---|---|---|---|
| Była prowadzona | 28,57% | 19,83% | 20,64% |
| Brak | 71,43% | 80,17% | 79,36% |
| Ogółem | 100% | 100% | 100% |
| χ2=2,074; p= 0,15 | V Cramera Cramer V=0,062; p=0,15 | ||
The aim of this research was to determine how often girls and boys with adolescent idiopathic scoliosis and their healthy counterparts experienced anomalies of the hip in their infancy period and to examine the correlation between the occurrence of anomalies of the hip and idiopathic scoliosis. The groups of adolescents participating in the research (scoliosis group and control group) did not differ in terms of age, sex or type of delivery. No significant differences regarding the incidence of AH in both groups were found and no correlation between AH and IS diagnosis in a later period of life was noted.
It is hard to refer the obtained results to the findings of other authors, since, to date, similar research has not been carried out. The incidence of AH at the level of 14.9% in the group of girls with scoliosis, 11.3% among the girls without scoliosis, 8.3% in the group of boys with scoliosis and 3.6% among the boys without scoliosis is higher than the mean incidence of hip dysplasia in the majority of the countries described in the literature [10]. The percentage values are higher since the study participants responded to a general question regarding the incidence of various anomalies of the hip in the infancy period. Thus, a positive response was provided both by parents/guardians of the youth who were diagnosed with DDH in the past and by parents/guardians of those who experienced movement limitations and asymmetry in the hip. In our opinion, collecting detailed information regarding the occurrence of DDH with the questionnaire was not possible due to incomplete knowledge of the issue demonstrated by the study participants and due to the fact that a definition of “dysplasia” used by doctors and other healthcare specialists is not uniform [9]. The research aimed at finding the correlation between IS and DDH in the infancy period confirmed by ultrasonography should be continued in specialist medical centres.
In the examined group of 533 participants, AH occurred three times more often in girls (12.7% of all the girls) than in boys (4.13% of all the boys). The analysis of the incidence of DDH conducted by other authors revealed that it was four times higher among girls than among boys [5,7,10]. Thus, in all the studies a clear correlation of the dysplasia of the hip and sex can be noted.
In our research, no significant correlation between the occurrence of AH in the infancy period and adolescent IS was revealed. These results do not comply with certain theories on a potential correlation between a disturbed movement function of the hip and the occurrence of scoliosis presented by some researchers [42]. Thus, anomalies of the hip coexisting with idiopathic scoliosis in children and youth [38,39,42] may be perceived as secondary changes accompanying scoliosis but not as its causes. However, it is worth highlighting again that the notion of AH in our research included various disorders of the hip. In order to define a clear correlation between particular anomalies of the hip and idiopathic scoliosis, further research and detailed diagnostics of hip joints in infants are needed.
It is worth noting that parents/guardians of children and youth without scoliosis applied treatment and preventive care in the infancy period on average 8% more often than parents/guardians of children with adolescent idiopathic scoliosis. However, this difference was not statistically significant. Perhaps following doctors’ recommendations regarding the prevention of anomalies of the hip decreases the risk of spine deformities; however, it needs to be explained in further research.
Physiotherapy was applied in adolescents with AH over 9% more often than in their healthy counterparts, but this difference was not statistically significant. Unfortunately, in this research no data were obtained regarding the reasons for referring to physiotherapy and the quality and duration of the applied therapy.
The present investigation is a pilot study. The questionnaire completed in the study by parents/guardians did not gather all the necessary information which would be valuable for the analysis of the study topic. It did not include detailed information concerning the type of hip diagnostics and its results, degree of the anomalies of the hip, a child’s age at the time of the research, the duration of conservative or preventive treatment, or indications for physiotherapy. These limitations resulted from the layout of the questionnaire including questions written in a simple language directed at people not connected with medicine. The correlation of DDH and other anomalies of the hip in the infancy period with IS needs to be examined in greater detail.
Anomalies of the hip such as dysplasia, movement limitations or asymmetry diagnosed in the infancy period did not reveal correlations with adolescent idiopathic scoliosis. Further research should be carried out with a focus on a separate analysis of the effects of dysplasia of the hip diagnosed in ultrasonography and other mobility-related anomalies of the hip on the occurrence of idiopathic scoliosis. It is necessary to prepare detailed documentation of hip examination in the infancy period.