
According to the definition of the World Federation of Occupational Therapists, occupational therapy is a health-related discipline that focuses on promoting health and well-being as well as enabling individuals to achieve life satisfaction through participating in various activities [1]. These include tasks that people want to do, need to do and are expected to do. The American Occupational Therapy Association defines activities as ordinary tasks performed on a daily basis. An activity is always of a personal significance to an individual; it is performed in a particular context and time and it has a psychological, social, cultural, ethnic and/or spiritual dimension [2].
We can distinguish activities associated with selfcare, leisure and productivity [3]. Self-care activities include e.g. getting dressed, preparing meals or eating. Leisure involves sports, hobbies or meeting friends. Productivity is linked with learning, professional work or household chores.
The primary goal of occupational therapy is to enable patients to take part in an activity they find significant, which helps to improve their well-being and increase their self-reliance as well as maintain health (in its broad sense) [3].
Occupational therapy can be performed on the basis of particular models which give form to undertaken activities. Reed and Sanderson claim that keeping up with the changing practice models is a significant factor in educating most occupational therapists [4]. It is an occupational therapist who makes a decision regarding which model is the best when it comes to analysing the patient’s state and selecting a proper therapeutic intervention. Some typical models applied in occupational therapy include Person-Environment-Occupation Model (PEO) [5], Kielhofner’s Model of Human Occupation (MOHO) [6] or Kawa Model [7].
The present study focuses on the last of the above models, i.e. the Kawa Model, which may also be successfully used by Polish occupational therapists.
The Kawa Model concentrates on an overall goal of occupational therapy, i.e. identifying activities that are important to patients and trying to enable therapy participants to do them. The application of the model allows therapists to recognize and interpret the state of patients taking into account their proper social and cultural contexts. The philosophy underlying the concept takes into account a postmodern and post-structural perspective, according to which people create their own interpretation of reality. The Kawa Model was created by Michael Iwama, a sociologist, anthropologist and an occupational therapist who was born in Japan and brought up in Canada.
This concept uses the metaphor of a river to depict a human life journey (in Japanese, ‘Kawa’ means ‘river’). The river constitutes the notion of ‘me’ of an individual and symbolises life journey. The source of the river represents the beginning of life, while the river mouth refers to death. In human life, the river flows through many meanders, encounters various obstacles and changes its level depending on the surroundings. Like a river, life is a complicated journey that takes place in a particular time and space. Iwama stresses that a human being ought to be perceived as a whole, together with the surroundings constituted by other people, physical environment and circumstances. These elements really affect an individual and an individual can influence them, too. The task of an occupational therapist is to examine and analyse all elements of the river in order to facilitate life flow [7].
Particular constructs of the model are metaphors of elements that form the river, i.e. water, river side walls, rocks and driftwood. The interpretation of the elements may vary depending on culture. In its initial version, the model referred to the culture of the East which determined the understanding of both particular components of the model and the whole concept. Attempts to apply the model in different parts of the world have shown the relevance of cultural influence on how the model is used and how its elements are perceived. Taking into account cultural relevance, particular components of the model such as water, river side walls, river bottom, rocks and driftwood will be described in terms of the Polish context.
Water (Mizu) represents the flow of human life and life energy. It affects all river elements and structures and the other way round. The flow of water can be either smooth or rough. The flow may be disturbed or impeded by the shape of the river bottom or by rocks. The flow represents the vigour and life dynamics of an individual. The weakened flow is a metaphor of feeling unwell and being in a state of disharmony [8].
River side walls (Kawa no Soku-Heki) and river bottom (Kawa no Zoko) represent physical, social, political and economic environments, which affect water flow. These elements are significant determinants of a person’s life flow in a particular social context. They determine the course of the flow as well as depth and width of the river. Physical environment includes space where an individual functions, e.g. home or workplace. Social environment consists of a family, social relations, professional work, friends, etc. Political and economic environment comprises specific conditions that influence an individual’s activity and possibilities of receiving institutional support. Compatibility of particular elements of physical, social, political and economic environments is essential for maintaining life flow. Using and sharing values with a social group that an individual belongs to is an important factor which gives that person a driving force [7].
Rocks (Iwa) represent life circumstances which are perceived by an individual as impediments that are difficult to remove. Each rock has its unique properties such as size, shape, colour and texture. Rocks can impede and obstruct flow. Some rocks represent illnesses or disabilities. In a therapeutic process, a patient has to identify rocks (problems), while an occupational therapist needs to determine how to remove the rock, change its location or decrease its size. If the patient has difficulties identifying the rock, the therapist may seek help from the patient’s relatives [8].
Driftwood (Ryuboku) depicts material and immaterial resources of a person such as personal attributes (e.g. reserved, outgoing), values (e.g. honest, hard-working), knowledge and experience (e.g. education, specific professional experience), skills (e.g. computer or public speaking skills), immaterial elements (e.g. having friends, siblings, children) and material assets (wealth, special equipment). These resources may exert either a positive or negative influence on circumstances and life flow. Even though driftwood may seem to be insignificant, it is a crucial element in therapy. For instance, a person’s strong religious faith combined with determination may be a positive factor that can erode or move rocks out of the way. Possessing enough financial resources to purchase special equipment helps to remove rocks and open a larger channel for one’s life to flow more strongly [8].
Spaces between obstructions (Sukima) are the last element of the river. These spaces are significant in terms of comprehending the patient’s state. They constitute the potential for conducting the process of occupational therapy. They give the therapist and the patient a reference point for analysing and solving problems at numerous levels. The occupational therapist has to enlarge spaces between rocks to let water flow and release the patient’s energy as well as let them perform activities they find significant.
The Kawa Model is a concept where the therapist focuses on the patient (Person-Centered Practice). The patient’s needs come to the fore and their perspective and expectations are taken into consideration. This approach stems from the Rogerian concept of the Client-Centered Therapy, according to which the therapist, by using non-directive techniques, helps the patient to accept themselves and to actualize the ‘self’ [9]. The therapy participant ought to experience unconditional acceptance, understanding and appreciation as a human being [10]. Rogers’s ideas adapted to the needs of occupational therapy are manifested through individualizing the care based on realizing needs, experiences and habits that are significant to the therapy participant [11]. The essence of the Person-Centered Practice approach was accurately captured by Sumsion, who stated that it means partnership between the patient and the therapist which strengthens and engages the person and allows them to perform important roles connected with activities they do in various environments [12]. The occupational therapist acts as a specialist who is expected to support the patient in an effort to become capable of expressing their needs and expectations [13].
The application of the Kawa Model in occupational therapy helps to structure a person’s narration. It also gives a possibility to put questions under discussion in order. Moreover, it makes it possible to obtain a full picture of the situation of the patient undergoing occupational therapy bearing in mind their resources and putting them in a specific social context.
The procedure of implementing the Kawa Model involves the following steps [7]. At first, the therapist explains the idea of the examination by stressing that the objective is to recognize the situation and try to define tasks that will be performed during the therapy. The therapist explains the significance of each component of the model and clarifies the meaning of water, rocks, river side walls and river bottom. Afterwards, the participant is asked to draw the river representing their life flow (step 1). When drawing the picture, the patient is not under time pressure. The drawing mainly aims to help to appreciate and understand an individual’s perspective in a narrative context. It is essential that the participant should speak freely. Next, the person draws the river cross section. It is worth mentioning that the river cross section is a diagnostic and therapeutic tool and it is a basis for planning, performing and assessing a specific intervention. When the drawing is completed, the therapist and the patient discuss its particular elements. First of all, they focus on explaining the context, i.e. on making an overall analysis of the person’s situation and of particular elements of the drawing (step 2). After that, the issues under discussion are prioritized according to the participant’s perspective (step 3). Later, the therapist and the patient identify the focal points of the therapeutic intervention (step 4). The next stage involves performing the intervention (step 5). The final stage is the evaluation of the completed intervention (step 6). At the end of the therapy it is worth asking the person to draw the river cross section again so as to compare the differences regarding the river elements, e.g. improving the flow and removing rocks or reducing their size. The occupational therapist should monitor the whole process and make sure its high quality is maintained. Furthermore, the therapist ought to make the participant feel comfortable and maintain partner relations.
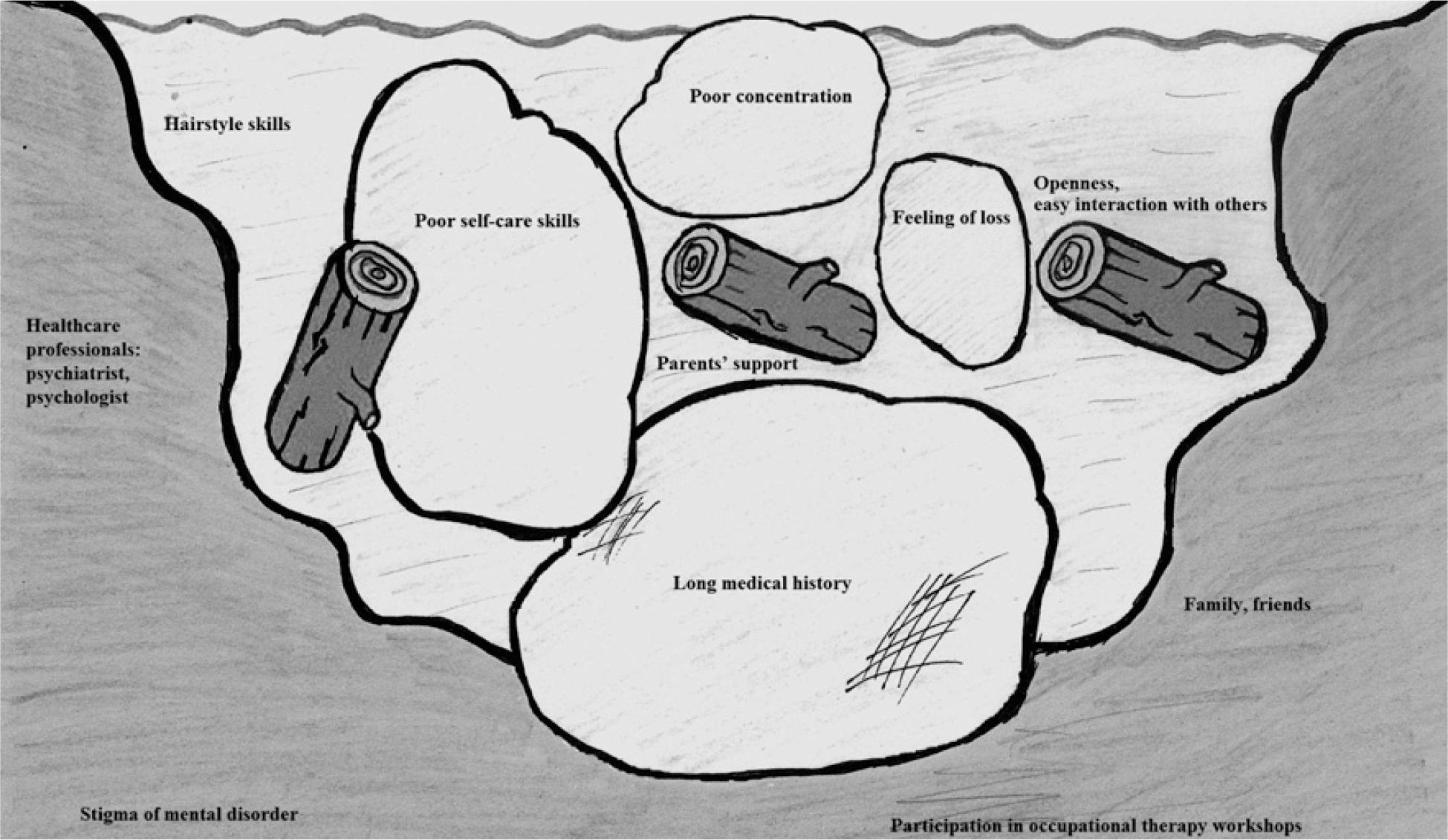
Ewa is 26 years old. She is an only child. She lives with her parents in a three-room flat. Ewa is dependent on her parents. She has never had a job. She is a sociable person and finds it easy to interact with others. She is keen on hairdressing and she follows the latest trends in hairstyling. Before falling ill, she had intended to enrol on a hairdresser course. Ten years ago she was diagnosed with paranoid schizophrenia. She was hospitalized twice. Currently she is tolerating drugs well. Ewa receives tremendous support from her parents, who do all the household chores for her. The patient does not develop her self-care skills. She is incapable of preparing her own meals and she does not do the shopping. She visits a psychiatrist and takes part in an individual therapy. Moreover, she participates in occupational therapy workshops. The people who attend the same meetings are her friends, who she meets outside the institution. The patient is convinced that she is perceived through the prism of her mental disorder and it causes her to feel lost.
The following description is a simplified version which refers to the analysis of the river cross section drawn by the patient and identifies areas of possible therapeutic interventions.
Water. The goal of the therapeutic intervention is to maximise Ewa’s life flow, which involves reducing and changing elements that impede free flow of life energy.
River side walls and bottom. Ewa lives with her parents who support her. She has a group of friends. She receives help from healthcare specialists and attends occupational therapy workshops. In her social environment she is perceived as a mentally challenged person.
Rocks. The major problem is that the patient has been ill for a long time, which affects her current situation considerably. Moreover, her self-care skills are poor as she cannot prepare her own meals nor can she do the shopping. Therefore, dealing with rocks should involve reducing limitations connected with poor self-care skills. Also, monitoring the patient’s psychophysical state is crucial. Ewa feels anxious about her future, which is associated with the fact that she perceives herself as a person with a mental disorder. Because of that she feels lost. Poor concentration can only be improved through participating in cognitive training sessions.
Driftwood. Ewa demonstrates the following personality attributes: openness, easy interaction with others. She likes hairstyling and she is interested in the latest trends in this field. Immaterial resources include strong support from her family and friends from occupational therapy workshops. From the standpoint of occupational therapy, drawing on the patient’s potential and engaging her in activities she finds significant (e.g. hairstyling) are fundamental issues.
Anthropometric points on the subject’s body [the authors’ own material]
Spaces between rocks. The role of occupational therapy is to maximise water flow that represents Ewa’s life energy. It may come about through improving her self-care skills. The key thing is to educate the woman’s closest relatives so that they will endorse her in an effort to improve her skills instead of helping her out with the simplest chores. It is essential that Ewa be allowed to perform the task that will render her life meaningful, improve her mood and boost her confidence regarding her skills. Her hairdressing interests and skills could be a starting point. For instance, the woman may begin to develop her skills by styling the hair of the participants of occupational therapy workshops. The next stage could be to improve these skills through taking part in special trainings and courses. Contacts with other people will increase Ewa’s participation in social life and may help her cope with fear of being perceived only through the prism of her disorder.
The Kawa Model is one of the options that an occupational therapist can make use of in order to determine and understand the situation of the therapy participant. It is possible to obtain a lot of data in a relatively short period of time.
Without doubt, the knowledge of the concept itself is needed to apply the model in therapeutic practice. It is also necessary to have at least basic psychological knowledge that would facilitate establishing a rapport and conducting occupational therapy effectively in accordance with the Person-Centered Practice approach.
As it has already been mentioned, the model developed by Michael Iwama is not well-known in Poland. Mainly students educated according to the latest international standards acquire some knowledge about it. However, professionally active occupational therapists can also update their knowledge of the subject and enrich their practice with approaches that are recognized worldwide and focus on the most important aspect of occupational therapy, i.e. enabling the patient to be healthy and ensuring their well-being through their participation in activities they find significant.