
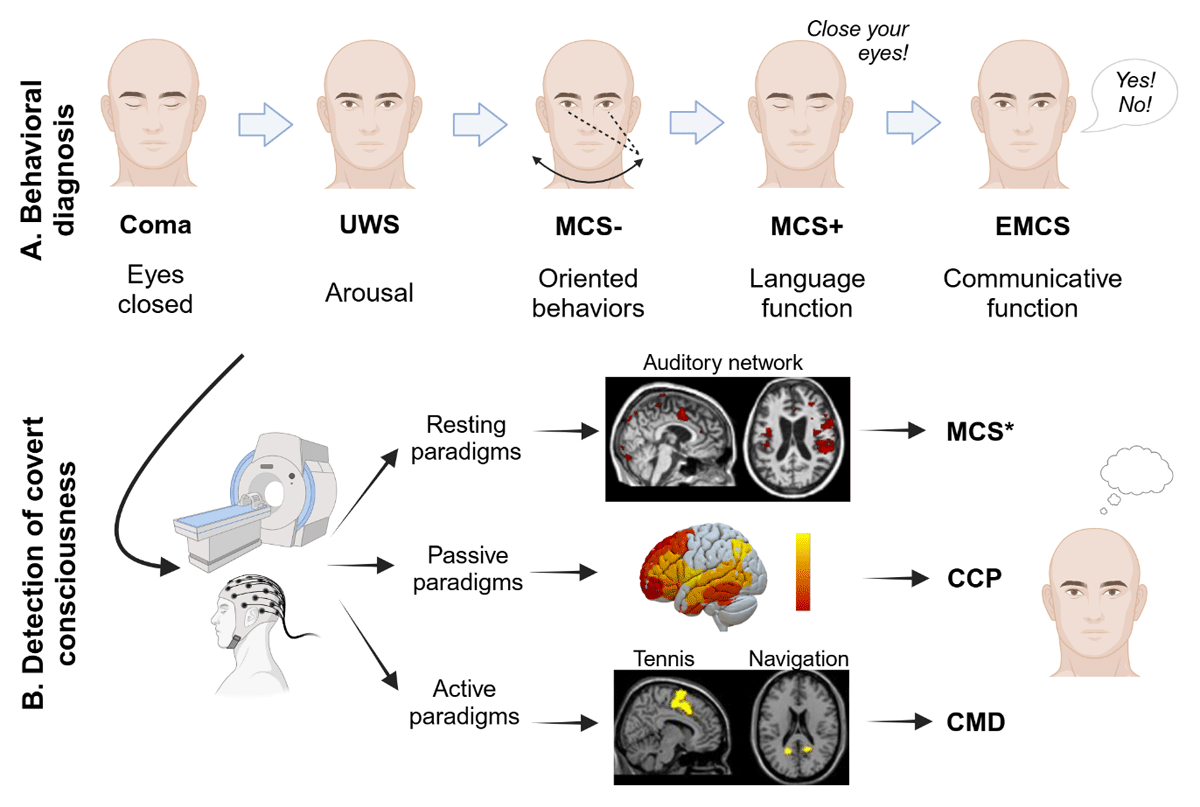
Figure 1
Characterization of consciousness levels after severe brain injury. A. Diagnosis is based on behavioral assessments: unresponsive wakefulness syndrome (UWS), minimally conscious state (MCS) and emergence from the MCS (EMCS). B. Neuroimaging or electrophysiological paradigms detect covert consciousness: non-behavioral MCS (MCS*) is identified in the resting state, covert cortical processing (CCP) in passive listening tasks, and cognitive motor dissociation (CMD) in active mental imagery tasks. Created with Biorender.com.
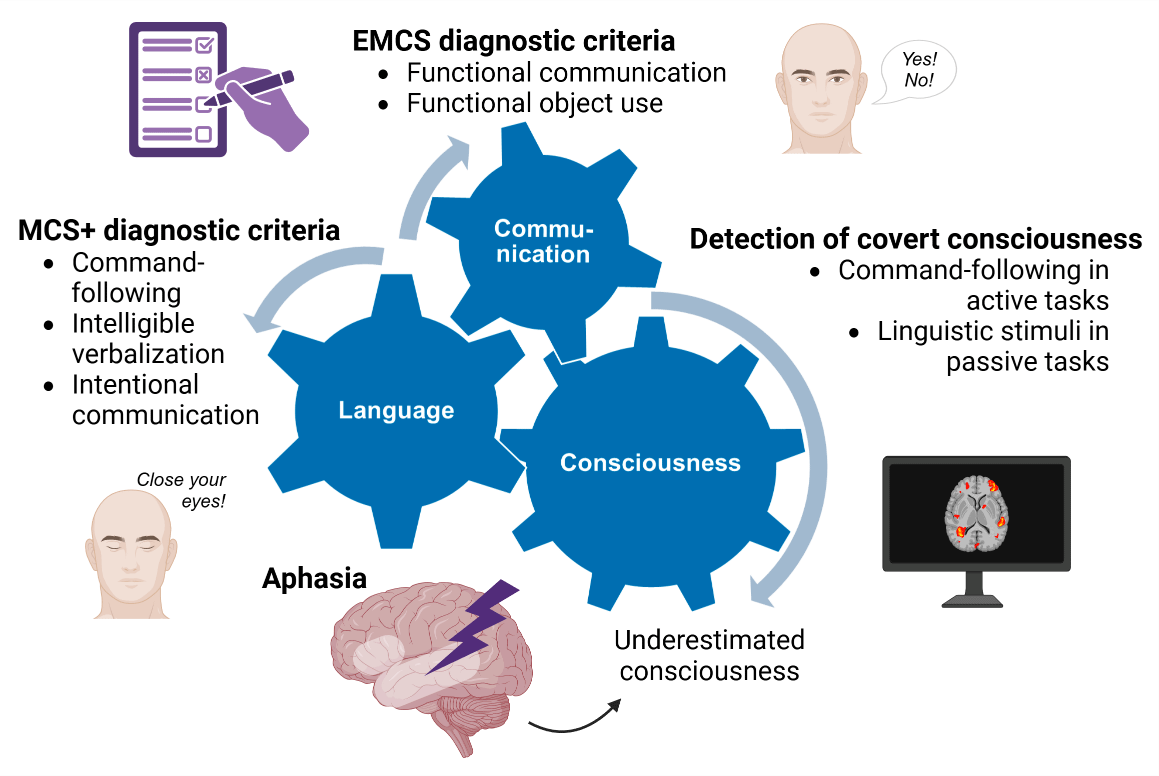
Figure 2
Interconnection of language, communication, and consciousness. Language-related and communication items are included in standardized behavioral assessment scales as criteria for MCS+ and EMCS diagnoses. Neuroimaging or electrophysiological passive and active paradigms detect residual covert consciousness based on language stimuli. Consequently, language impairments may lead to an underestimation of patients’ consciousness level. Created with Biorender.com.
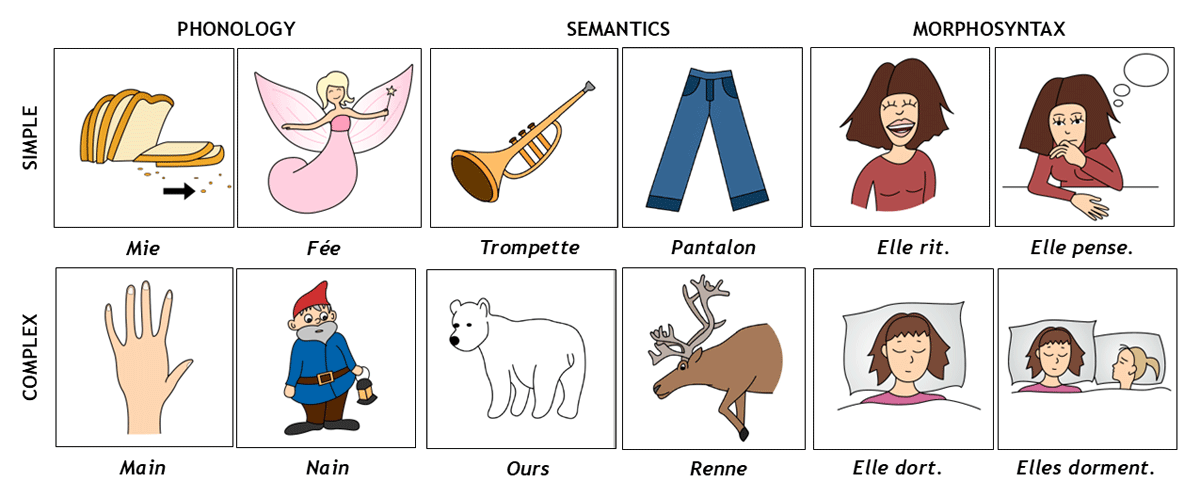
Figure 3
Examples of items from the French version of the Brief Evaluation of Receptive Aphasia tool. Simple phonological items require the discrimination of monosyllabic words that do not share any phonemes, while complex phonological items involve minimal pairs (i.e., monosyllabic words differing by only one of two phonemes). Simple semantic items involve distinguishing words from two different semantic categories, whereas complex semantic items contrast words belonging to the same semantic category. This semantic subscale also controls for word frequency. Finally, simple morphosyntactic items consist of two sentences with different meanings but sharing the same morphosyntactic structure, while complex morphosyntactic items contrast sentences that differ across multiple morphosyntactic features (e.g., number, gender, active vs. passive voice…).
Table 1
Neuroimaging and electrophysiological signs suggestive of covert consciousness.
| RESTING BRAIN ACTIVITY | PASSIVE PARADIGMS | ACTIVE PARADIGMS | |
|---|---|---|---|
| FDG-PET | Preservation of brain metabolism in the frontoparietal cortex (Thibaut etal., 2021) | Preserved association cortices activation to patients’ own name (Laureys et al., 2004) | / |
| fMRI | Preserved functional connectivity in auditory and default mode networks (Demertzi et al., 2015) | Preserved brain activity associated with higher-order processing of linguistic stimuli, including activation in the temporal lobe (Coleman et al., 2009) | Brain activation consistent with command-following in motor imagery or silent naming tasks (Owen et al., 2006; Rodriguez Moreno et al., 2010) |
| EEG | Global functional connectivity and power spectrum preservation (Duszyk-Bogorodzka et al., 2022; Thibaut et al., 2021) | Preserved event-related potentials (e.g., N400 wave) to linguistic stimuli(Balconi et al., 2013; Balconi & Arangio, 2015; Formisano et al., 2019) or speech-tracking responses (Braiman et al., 2018; Gui et al., 2020; Sokoliuk et al., 2020) | Command-following capacity reflected by power spectrum changes during motor imagery (Claassen et al., 2019) or preserved event-related potentials (e.g., P300) during counting tasks (Guger et al., 2018) |
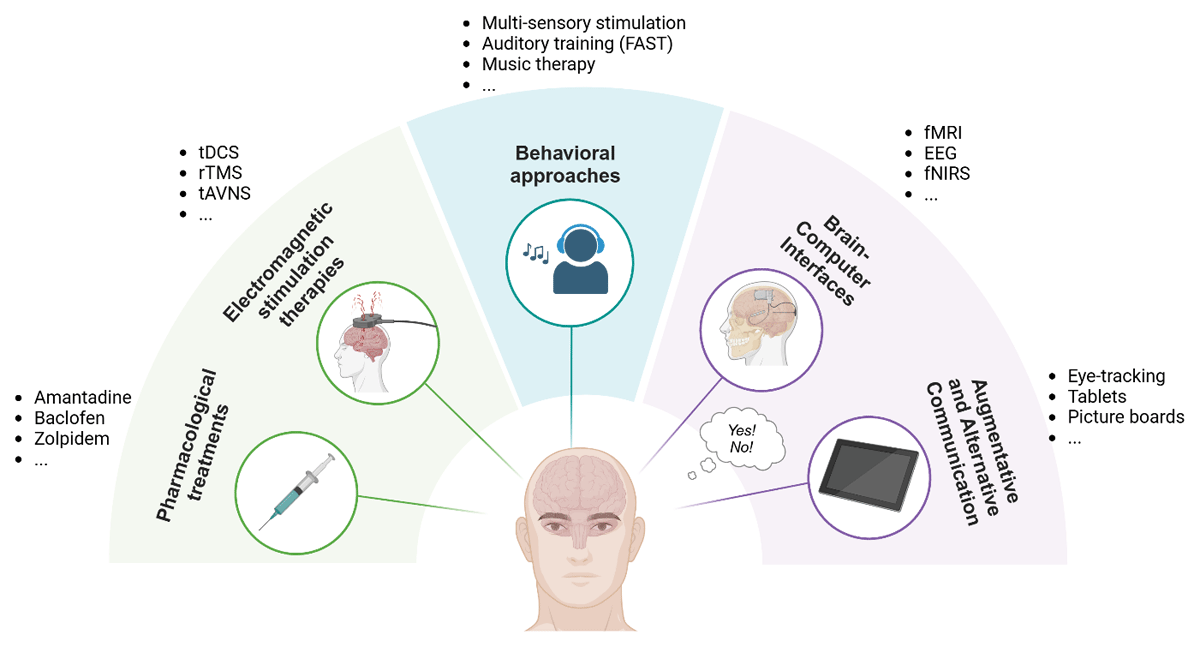
Figure 4
Overview of current interventions for consciousness, language and communication recovery. While pharmacological and electromagnetic therapies show promise in consciousness recovery (including language function and communication), behavioral approaches involve sensory, language or music stimulation. BCIs and AAC provide tools for reestablishing and optimizing communication skills in DoC and EMCS patients, respectively. Created with Biorender.com.