
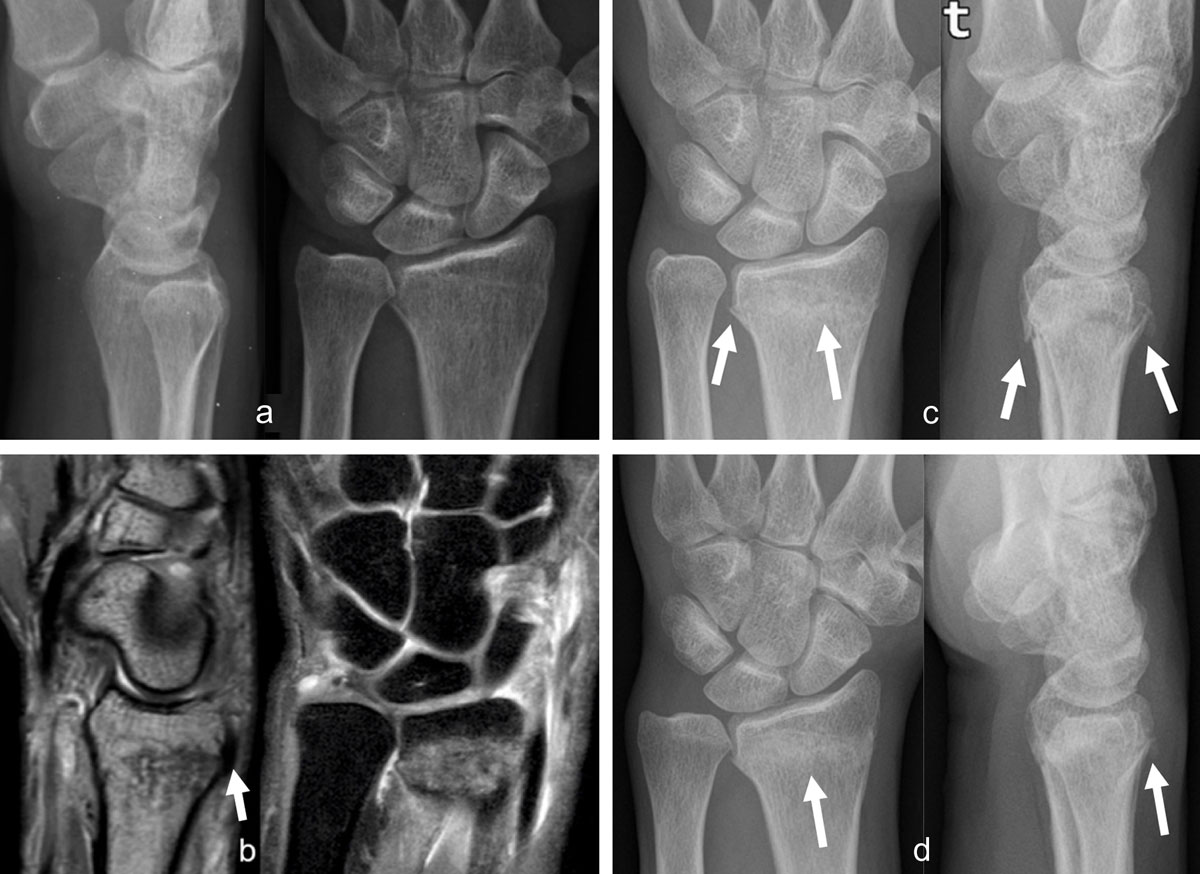
Figure 1
Occult radius fracture detected by MRI. The radiographs, (a) lateral and anteroposterior views, obtained the day after trauma were negative. Three days later, sagittal PD and coronal PDFS, (b) MR images revealed a nondisplaced radius fracture with extensive bone marrow edema and posterior cortical irregularity on the sagittal view (arrow). Control radiographs (AP and lateral views) obtained one month (c, arrows) and two months (d, arrows) post trauma depict consolidation signs, better seen on d (arrow).
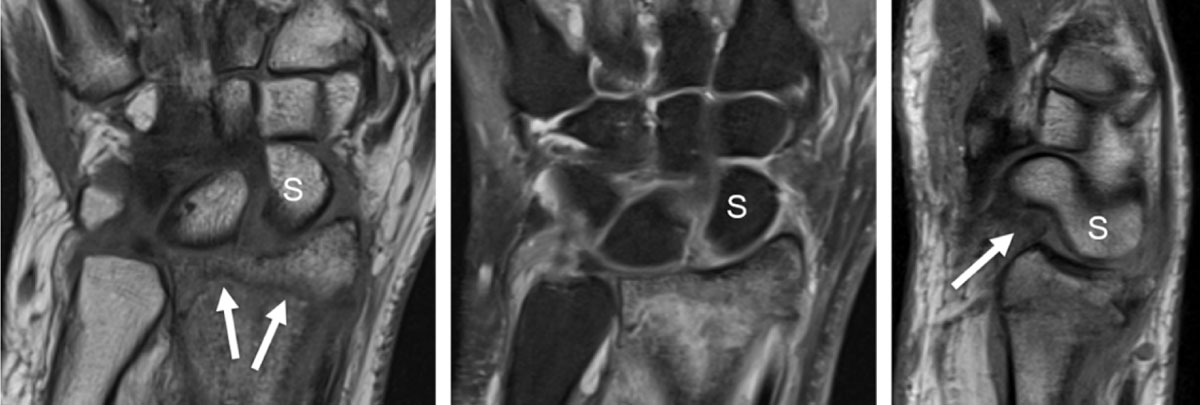
Figure 2
Distal radius fracture with associated intrinsic scapholunate (SL) and extrinsic palmar radiocarpal ligament rupture (RSC, radioscaphocapitate) detected by MRI. T1 coronal slice (a) shows the fracture line (arrows) and the increased SL space. Proton-density fat saturated coronal slice (b) demonstrates high signal surrounding bone marrow edema and increased signal of the SL space. Sagittal proton-density slice (c) detects a dorsal avulsion of the distal radius and a torn palmar RSC ligament (arrow) with rotatory subluxation of the scaphoid (S).

Figure 3
Evolution of scaphoid fracture with pseudarthrosis in a 17-year-old male. Radiograph obtained in AP view with ulnar deviation (a) one month after trauma discloses an evident fracture of the scaphoid middle third (which was not visible on the first radiographs performed on the day of trauma). As the wrist remaining painful and bone scintigraphy performed one year after trauma was positive at the level of the scaphoid, MRI was obtained to exclude an avascular necrosis at the proximal pole of the scaphoid. Coronal proton-density slice (b) and sagittal fat saturated proton-density slice (c) revealed pseudarthrosis without osteonecrosis and an extensive bone marrow edema of the whole scaphoid with surrounding soft tissue edema and elongation of the palmar RSC ligament (arrow) on c.
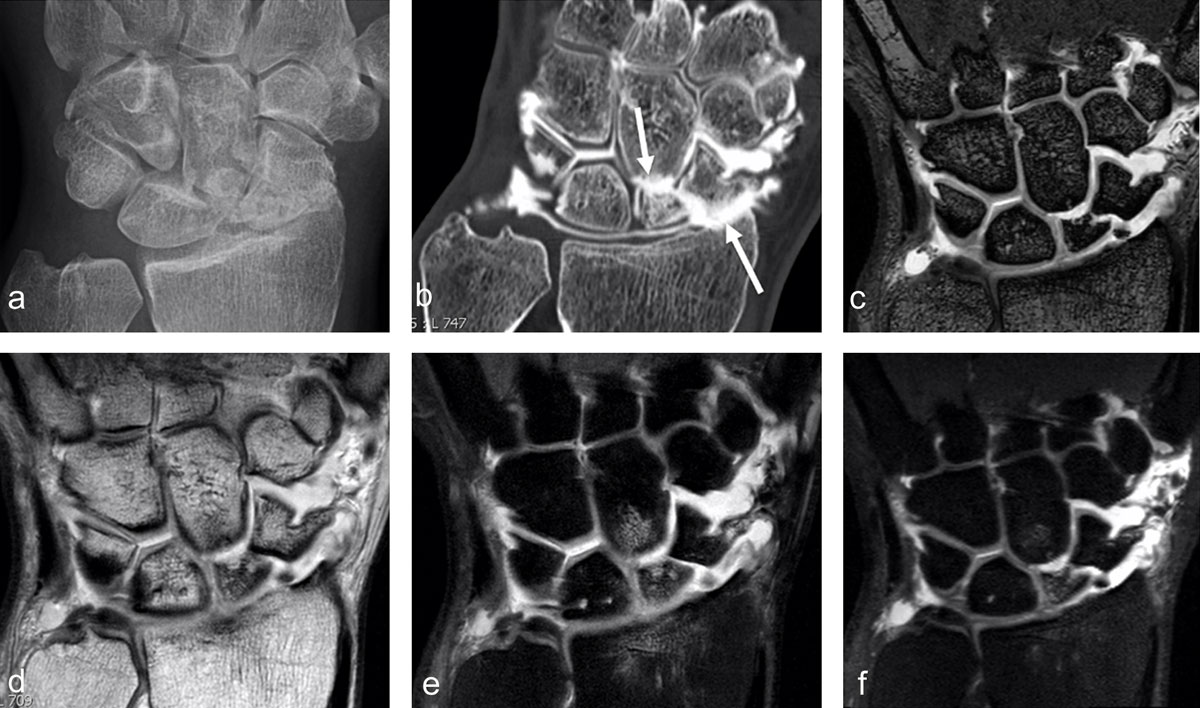
Figure 4
SNAC 2 wrist after scaphoid fracture with nonunion in a 41-year-old man. Secondary cartilage degeneration is first seen in the radioscaphoid compartment (b, arrow pointing up) and later in the scaphocapitate midcarpal joint space (b, arrow pointing down) on conventional radiograph and much better on CT-arthrography (b). MRI well demonstrates the nonunion (on 3D DESS with 0.4mm sections) and increased signal in the proximal scaphoid pole on 2D (e) and 3D (f) proton-density fat-saturated images, corresponding to edema and indicating that the separated fragment might be unstable (and painful). Subchondral bone marrow edema is also detected in the proximal pole of the capitate under the cartilage loss and in the distal radius (e).
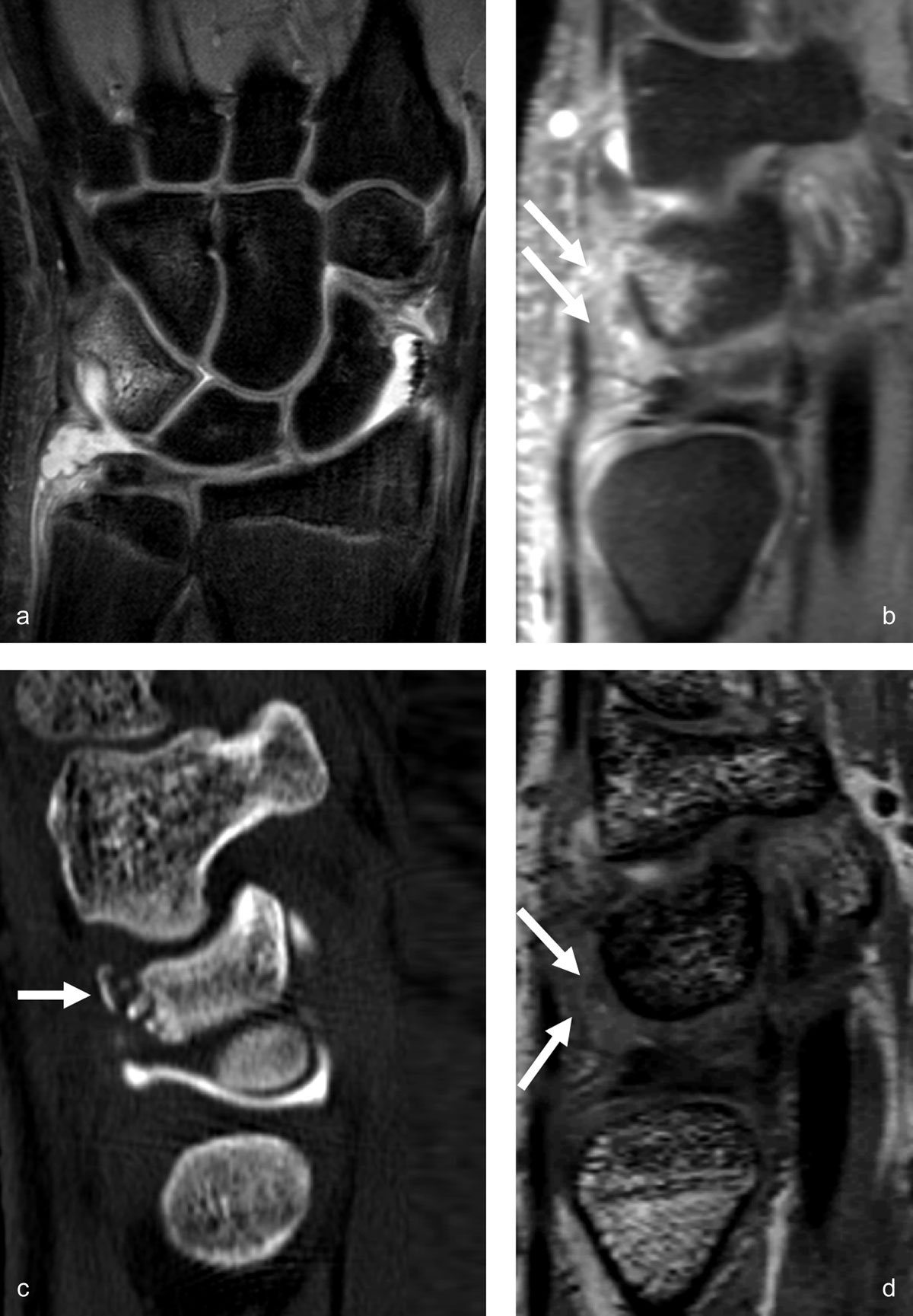
Figure 5
Triquetrum occult fracture with synovitis in the prestyloid recess and traumatic bone avulsion with subacute edematous infiltration of the dorsal capsular ligaments. MR arthrography performed 12 days after a fall on an outstrechted hand allows detection of bone marrow edema in the dorsal part of the triquetrum on coronal proton-density fat-saturated images (a) and sagittal 0.4mm reconstruction from a 3D proton-density fat-saturated sequence (b), as well as edematous infiltration of the surrounding dorsal soft tissues (arrows on b). The dorsally avulsed bony fragments are better seen on CT (arrow on c). The dorsal capsular infiltration (mostly the extrinsic dorsal radiotriquetral ligament) with low to intermediate signal intensity is also depicted on the sagittal reconstruction from the 3D DESS sequence (arrows on d).
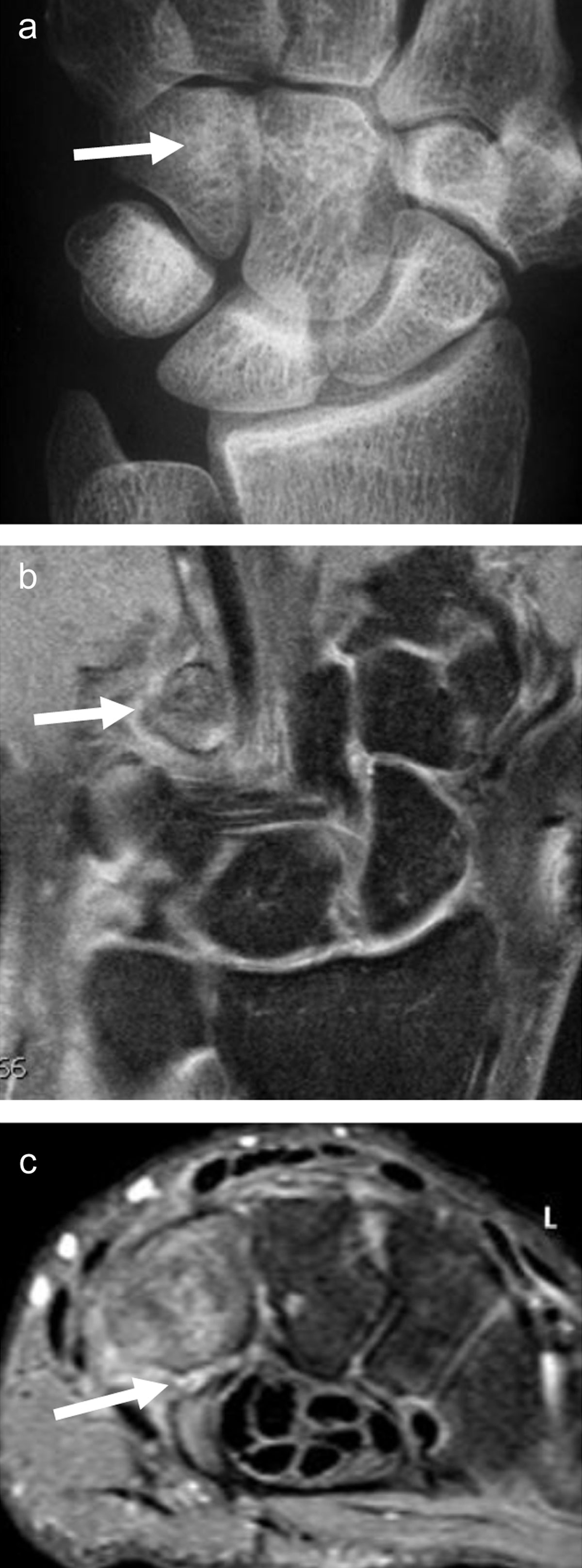
Figure 6
Fracture of the hook of the hamatum, easily missed on conventional radiographs and on fat-saturated MR images. The AP X-ray (a, arrow) demonstrates the absence of the ring sign (normally present at the level of the hamulus) on the hamate bone. On palmar proton-density fat-saturated coronal image (b, arrow), the presence of BME within the hamulus may be obscured because of the close signal intensity of the surrounding muscles. The fracture line at the base of the hamulus could also be missed on the axial proton-density fat-saturated sequence (c, arrow).

Figure 7
Another case of direct compression of the hook of the hamate. Axial CT (a) and sagittal reconstruction (c) disclose the avulsion fracture, much easier than the corresponding axial (b, arrow) and sagittal (d, arrow) proton-density fat-saturated MR images.
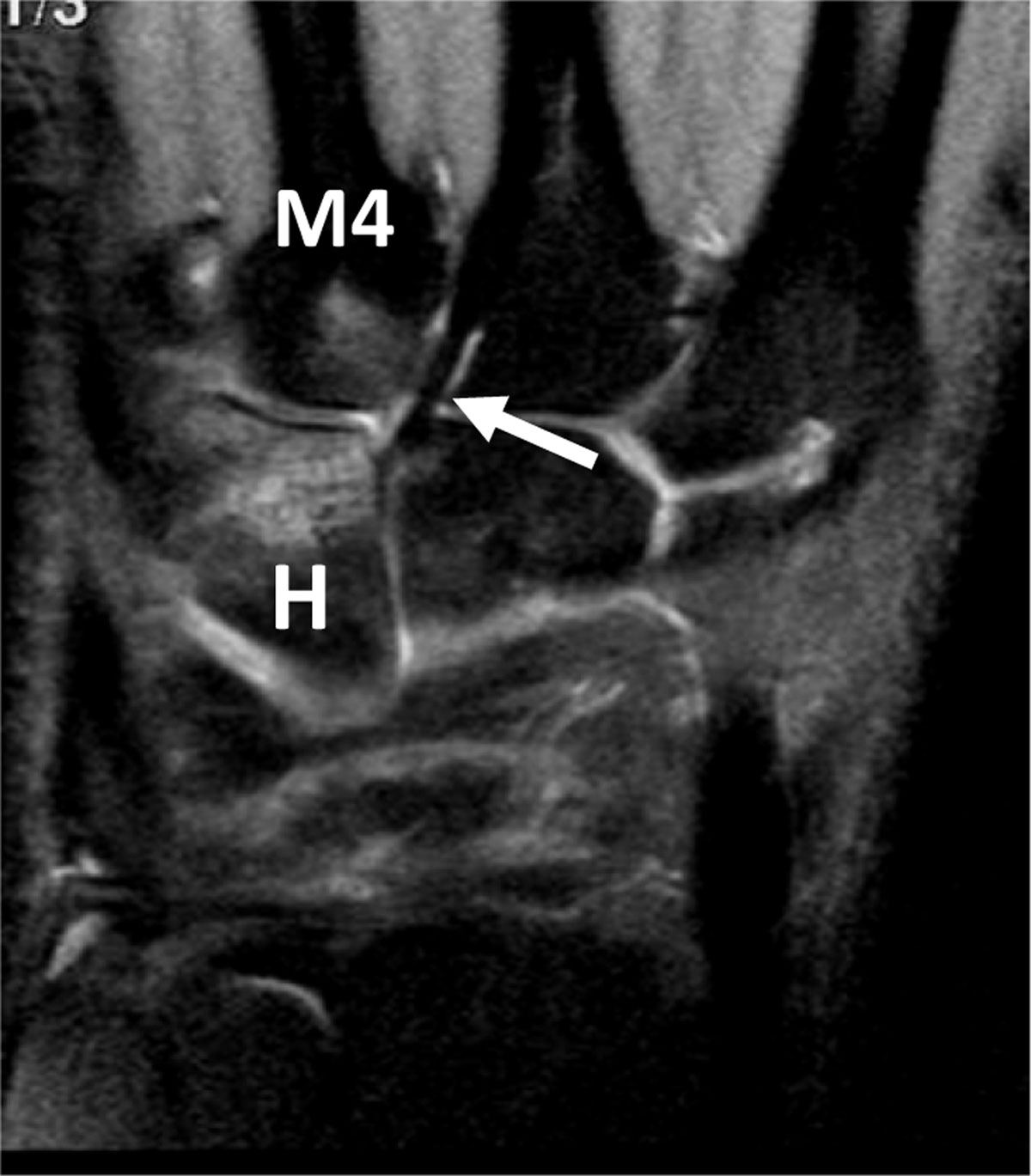
Figure 8
Hamate BME and associated BME of the fourth metacarpal base in an overused pianist hand. Coronal proton-density fat-saturated MR image depicts high signal bone marrow infiltration of the distal half of the hamatum (H) and proximal base of the fourth metacarpal (M4) nearby the capito-third metacarpal ligament (arrow) which is strong in this professional piano player.