
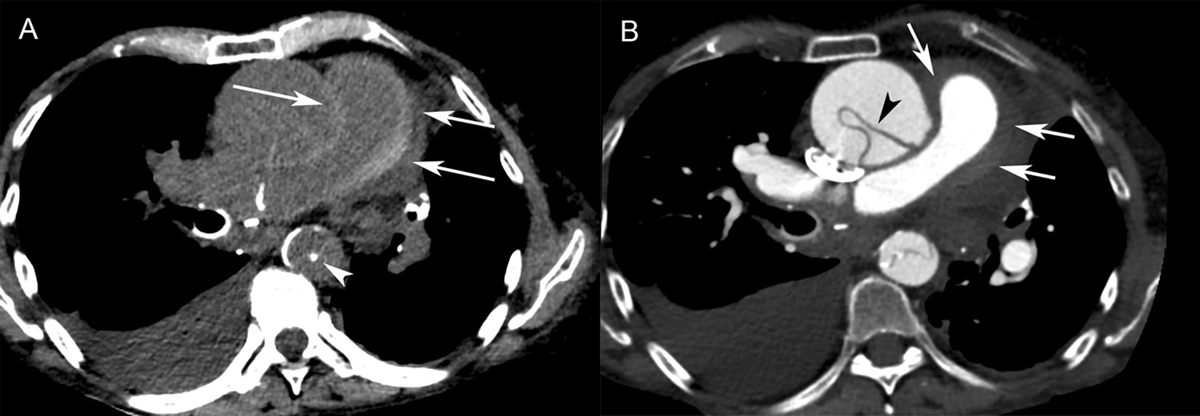
Figure 1
Patient 1. (A) Axial non-contrast-enhanced CT showed circumferential high attenuation along the walls of the pulmonary trunk (70 HU) and right pulmonary artery (arrows), consistent with an intramural hematoma. An ascending aortic aneurysm with displacement of atherosclerotic calcifications into the lumen of the descending aorta (arrowhead) was seen. Right pleural effusion was also visible. (B) Contrast-enhanced CT revealed Stanford type A aortic dissection. The intimal flap was seen in the ascending aorta (arrowhead) and descending aorta. The high attenuation area of the pulmonary arterial wall was non-contrast-enhancing (arrows), which was consistent with pulmonary artery intramural hematoma.
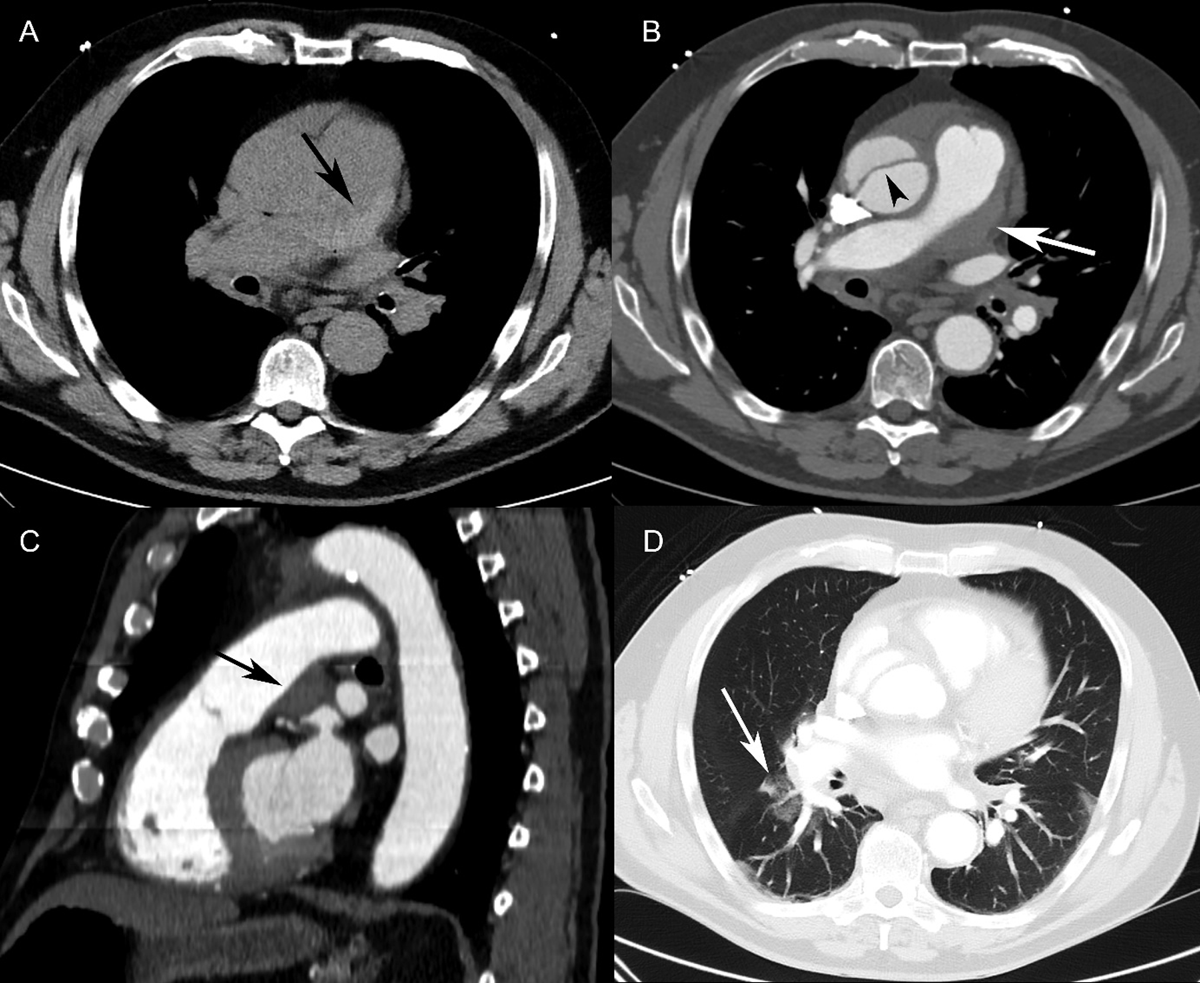
Figure 2
Patient 2. (A) Axial non-contrast-enhanced CT showed a hyperdense lesion along the pulmonary trunk wall (black arrow). (B) Contrast-enhanced CT (axial view) revealed an eccentric hypodense defect in the pulmonary trunk (white arrow), mimicking a mural thrombus. The intimal flap was seen in the ascending aorta (arrowhead). (C) Sagittal reformatting of a contrast-enhanced CT scan revealed a lesion with well-defined margins at an obtuse angle (black arrow) along the pulmonary trunk wall, resulting in a slight narrowing of the pulmonary trunk lumen. This was not enhancing, suggestive of an intramural hematoma. (D) Axial CT (lung window) showed patchy ground-glass opacities in the right lower lobe around the segmental pulmonary arteries, consistent with alveolar hemorrhage.
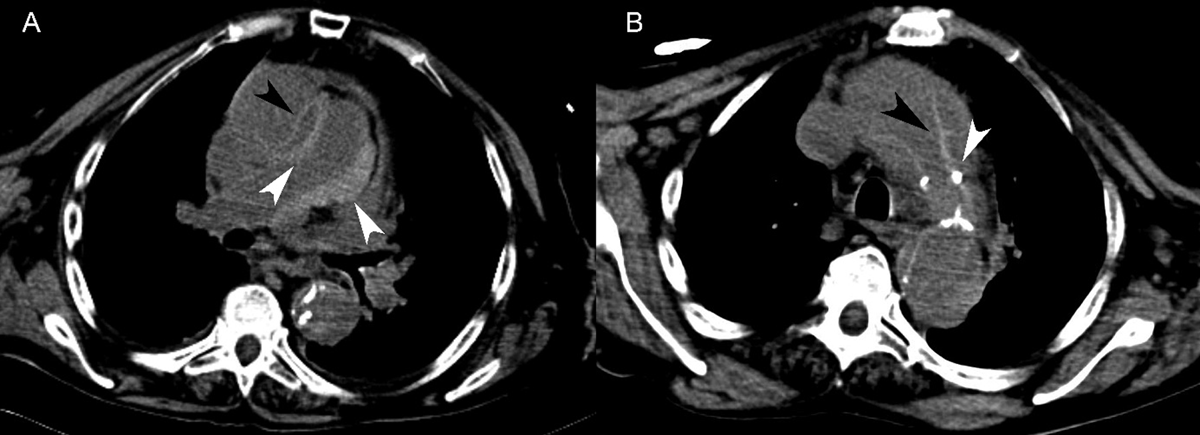
Figure 3
Patient 3. (A) Non-contrast-enhanced CT showed circumferential high attenuation along the walls of the main and right pulmonary arteries, consistent with pulmonary artery intramural hematoma (white arrowheads). Stanford type A aortic dissection with an intimal flap in the ascending aorta was also seen (black arrowhead). (B) Non-contrast-enhanced CT revealed an intimal flap of the thoracic aorta (black arrowhead) and displacement of atherosclerotic calcifications into the aortic lumen (white arrowhead).
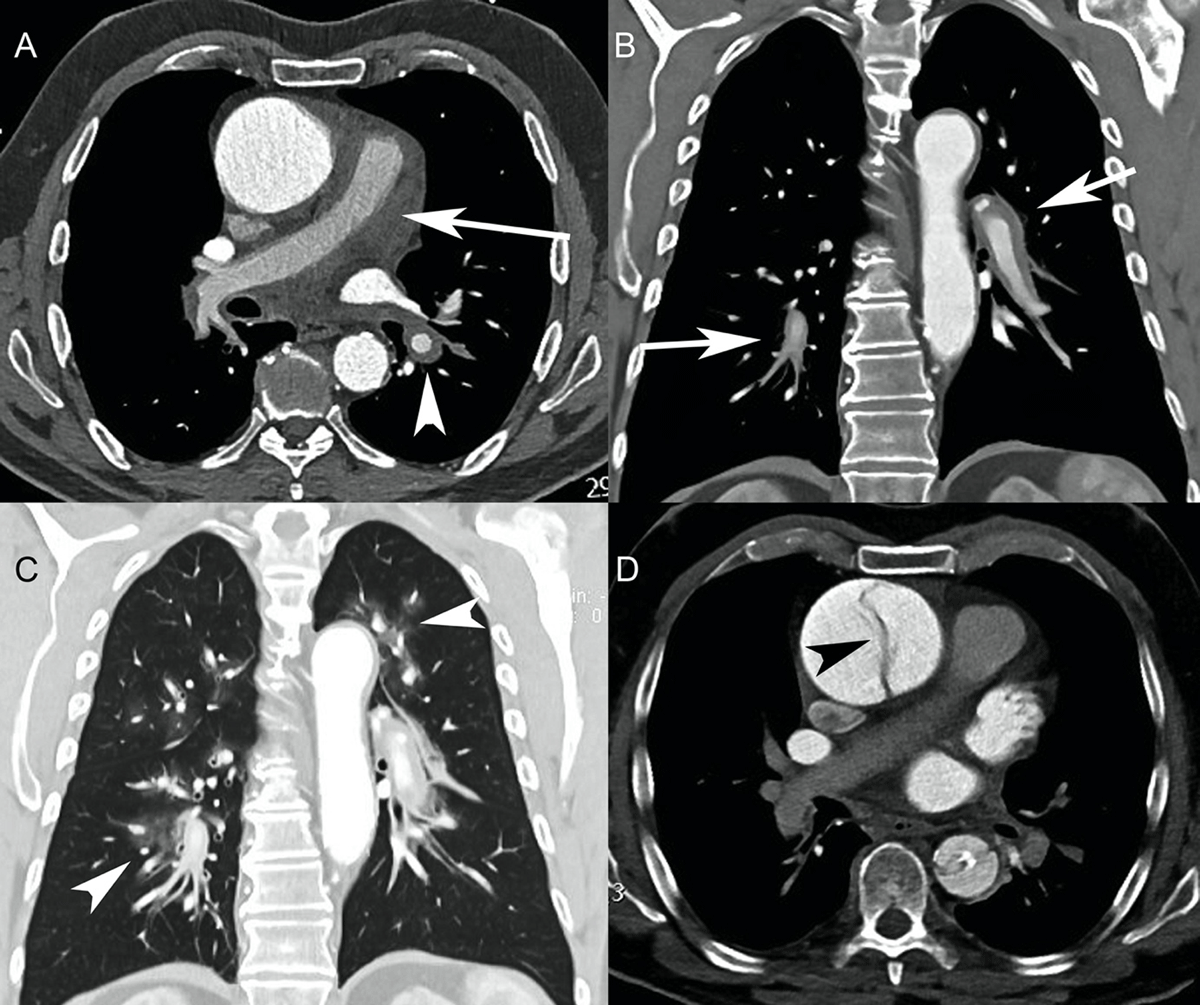
Figure 4
Patient 4. (A) Initial axial CT angiography (CTA) showed an aortic aneurysm. No intimal flap was seen. However, the contour of the ascending aorta was irregular. There was circumferential thickening of the pulmonary arterial wall (arrow), extending into the right and left pulmonary arteries (arrowhead), suggestive of pulmonary artery intramural hematoma. (B) Initial CTA (coronal reformation) showed the extension of the pulmonary artery intramural hematoma to the interlobar and segmental pulmonary arteries (arrows). (C) Initial CTA (coronal reformation, pulmonary window) revealed ground-glass opacities around the pulmonary arteries consistent with alveolar hemorrhage (arrowheads). (D) Second axial CTA performed two days later showed an intimal flap of the ascending aorta, suggestive of Stanford type A acute aortic dissection (arrowhead). Both the pulmonary artery intramural hematoma and alveolar hemorrhage had resolved.