

Figure 1
Initial axial non-enhanced CT. A. Soft tissue and B. bone window show a slightly hyperdense mass to gray matter (arrow) located at the right frontal bone causing scalloping of the internal and external table (arrowhead). There is focal discontinuity of the external and internal table. Remnants of the expanded frontal bone (thin arrow) can be seen medially.
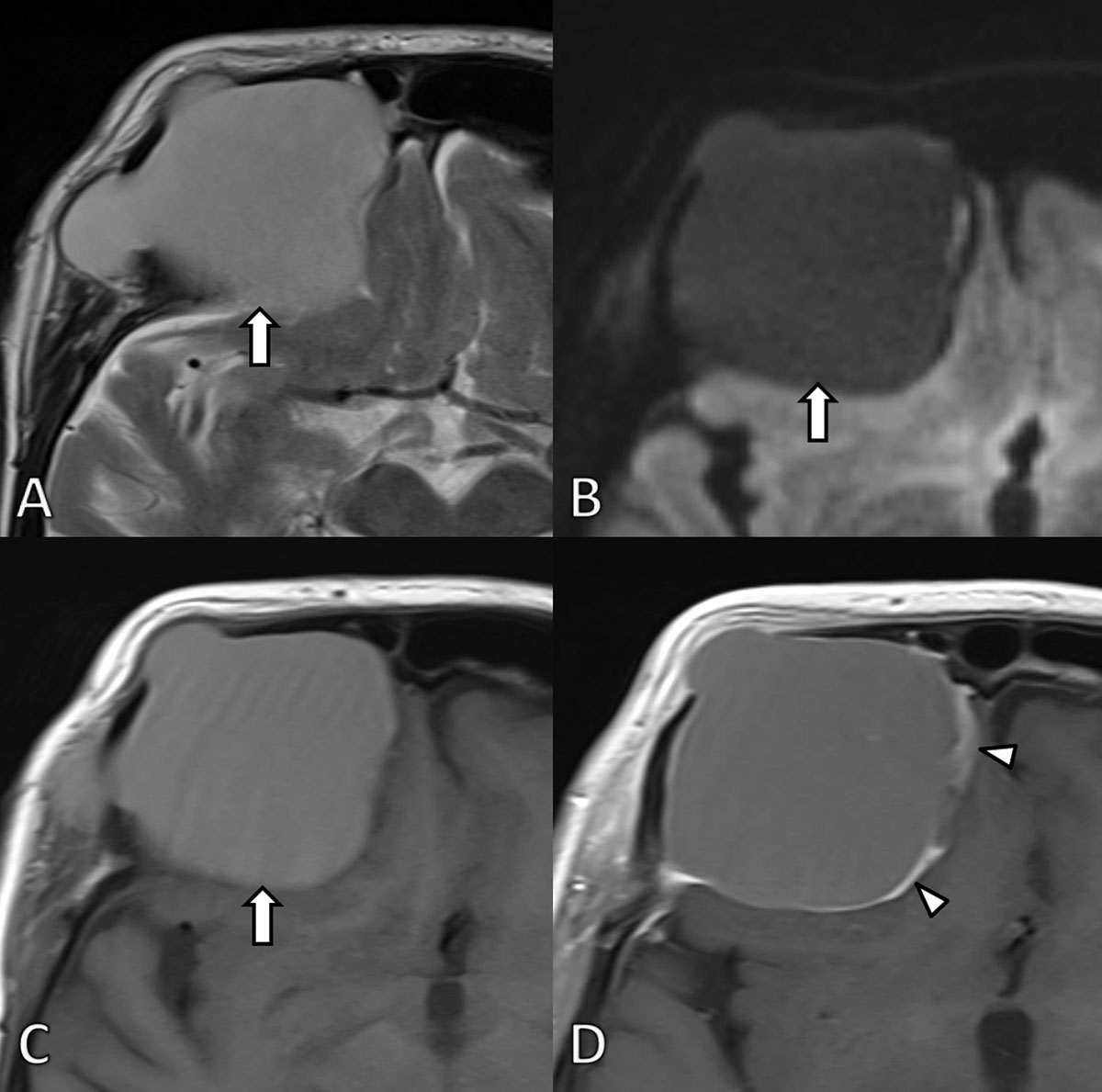
Figure 2
MRI at first admission. A. Axial T2-WI. B. Diffusion weighted image (b1000) and C. T1-WI before and D. after gadolinium contrast administration confirm the presence of a well-defined expansile mass (arrow) at the frontal bone. The signal is homogenously hyperintense on T2 and T1-WI images in keeping with high protein content. The lesion did not demonstrate restricted diffusion. After administration of gadolinium contrast the lesion shows subtle peripheral contrast enhancement (arrowheads). The lesion exerts mass effect on the frontal lobe.
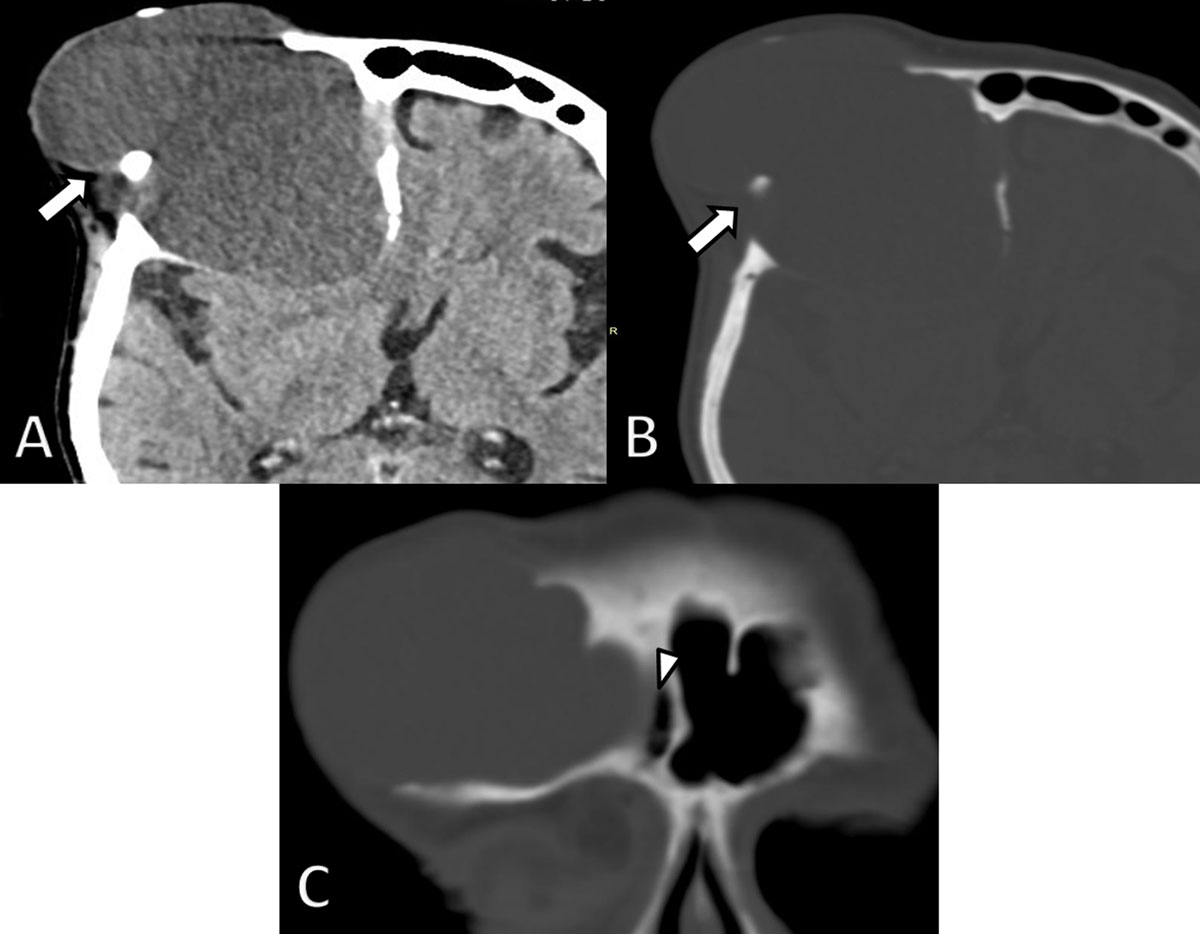
Figure 3
Axial non-enhanced CT images four years later. A. Soft tissue and B. bone window demonstrate considerable growth of the lesion (arrows) and a decrease in density. There is increased osteolytic destruction of the frontal bone and progressive extra-axial extension into the brain with mass effect on the frontal horn of the lateral ventricle. C. Coronal reformatted CT image shows an intimate relationship of the lesion with the right frontal sinus (arrowhead).

Figure 4
MRI scan 4 years later. A. Axial T2-WI. B. Diffusion weighted image (b1000) and C T1-WI and D. subtraction image of T1-WI before and after gadolinium contrast administration. The lesion (arrows) is slightly more hyperintense on T2-WI and slightly less intense on T1-WI compared to the previous examination due to a higher fluid content. There is no diffusion restriction and persistent subtle peripheral contrast enhancement (arrowheads).
Table 1
Predisposing factors for mucocele formation.
| – Chronic sinusitis |
| – Craniofacial malformations |
| – Systemic diseases (Cystic fibrosis, Granulomatosis with polyangiitis, …) |
| – Obstruction by neoplasia |
| – Surgery |
| – Facial trauma |
Table 2
Imaging characteristics of giant frontal sinus mucoceles described in previous case reports.
| Authors | Size (cm) | General characteristics | Density compared to grey matter on NECT | Enhancement on CECT | MR findings | |||
|---|---|---|---|---|---|---|---|---|
| T1-WI SI* | T2-WI SI* | Enhancement | Other | |||||
| Singh et al. (2019) Case report [5] | 8 × 8 × 7 | Expansion and thinning of the frontal bone | Hypodense with peripheral calcifications | N/A | Intermediate | High | Peripheral enhancement | No diffusion restriction. Focal organized hemorrhage inside the lesion |
| Alshoabi, Gameraddin. (2018) Case report [1] | 10 × 9 | Isodense | Peripheral enhancement | Intermediate | High | N/A | N/A | |
| Carmichael, Kang. (2015) Case report [4] | 4 × 6.5 | Intermediate density | N/A | N/A | N/A | N/A | N/A | |
| Kawaguchi et al. (2002) Case report [2] | N/A | Isodense with peripheral calcifications | N/A | Intermediate-Low | High | Peripheral enhancement | N/A | |
| Saki et al. (2000) Case report [6] | 6.6 × 8.5 | Heterogenous iso- and hypodense | N/A | N/A | N/A | N/A | N/A | |
[i] NECT: Non-enhanced CT, CECT, contrast-enhanced CT, N/A: Data not available. * Signal intensity compared to grey matter.