
Table 1
Summary of cases needing the anchoring wire technique.
| Patient | Age (years) | Type ofintervention | Anchored vessel | Target vessel | Procedure time (minutes) | Fluoroscopy time (minutes) | DAP (Gy.cm2) |
|---|---|---|---|---|---|---|---|
| 1 | 54 | TACE | SMA | Right hepatic artery | 95 | 45 | 100 |
| 2 | 62 | TACE | SMA | Pancreatic arcad | 165 | 48 | 245 |
| 3 | 80 | TACE | Hepatic artery | Left gastric artery | 85 | 55 | 505 |
| 4 | 51 | TACE | Right renal artery | Right adrenal artery | 60 | 21 | 302 |
| 5 | 48 | Digestive bleeding embolization | SMA | Jejunal branches | 72 | 30 | 55 |
| 6 | 77 | Digestive bleeding embolization | SMA | SMA branch | 86 | 23 | 123 |
| 7 | 80 | Digestive bleeding embolization | SMA | DPA | NA | NA | NA |
| 8 | 49 | Duodenopancreatic artery pseudo-aneurysm embolization | Splenic artery | CHA | NA | 49 | 175 |
| 9 | 61 | Hepatic pseudo-aneurysm embolization | Splenic artery | CHA | 107 | 33 | 310 |
| 10 | 75 | Dorsal pancreatic artery aneurysm embolization | DPA | Dorsal pancreatic artery | 103 | 24 | 50 |
| 11 | 68 | Celiac trunk aneurysm angioplasty (with stent) | Splenic artery | CHA | 72 | 44 | 111 |
| 12 | 59 | Hepatic artery pseudo-aneurysm embolization | Splenic artery | Hepatic artery | 76 | NA | NA |
| 12 | 59 | Hepatic artery of the graft angioplasty (with stent) | Splenic artery | Hepatic artery | 53 | NA | NA |
| 13 | 70 | Hepatic artery of the graft angioplasty (without stent) | Splenic artery | Hepatic artery | 56 | 19 | 89 |
| 14 | 66 | Hepatic veins angioplasty and hepatic biopsy | Inferior vena cava | Hepatic veins | 56 | 20 | 123 |
| 15 | 52 | Renal angiomyolipoma embolization | Left renal artery | Left adrenal artery | 76 | 36 | 152 |
| 16 | 73 | Bone hypervascular metastasis embolization | Right femoral artery | Right profunda femoral artery | 256 | 49 | 148 |
[i] CHA: common hepatic artery; DAP: dose area product; DPA: duodenopancreatic arcad; NA: not available; SMA: superior mesenteric artery; TACE: transarterial chemoembolization.
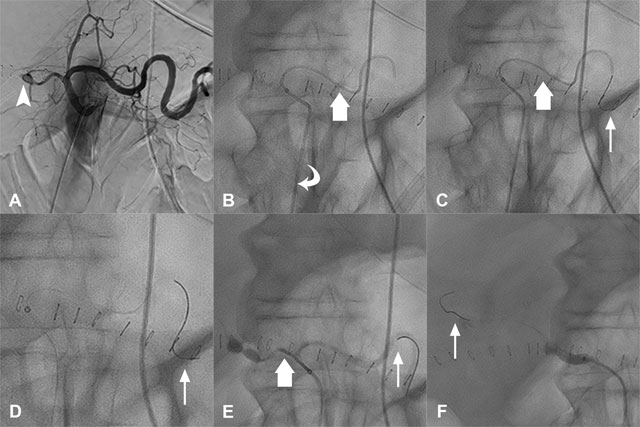
Figure 1
Details of the Parallel Guidewire Anchoring Technique. Angioplasty without stenting of the graft hepatic artery in a 70-year-old patient. A. Initial arteriography showed a graft hepatic artery stenosis (arrowhead). B. Catheterization was performed as distally as possible in the splenic artery with a catheter and a microcatheter (large arrow) through a long sheath (curved arrow). C. A stiff 0.014” guidewire (thin arrow) was introduced into the microcatheter (large arrow). D. The microcatheter and the catheter were completely removed. E. The catheter and the microcatheter (large arrow) were introduced in parallel of the stiff guidewire and used to catheterize the common hepatic artery. F. The stiff guidewire (thin arrow) was removed from the splenic artery to position the long sheath further into the graft hepatic artery.