
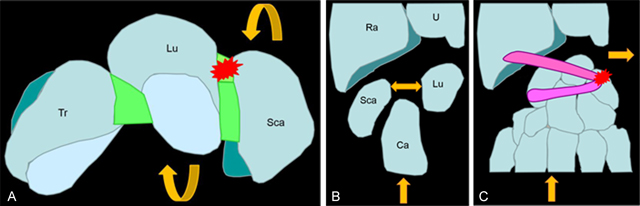
Figure 1
(A–B) The common mechanism leads to a stress of the scapholunar complex (red star) with a sudden horizontalization of the scaphoid increased by the compressive load induced by the capitates bone (rounded yellow arrow) with increased width of the scapholunate space (straight yellow arrow). (C) The sudden ulnar movement of the carpal bones during trauma explains the high frequency of triquetral avulsion (red star) of the dorsal sling.
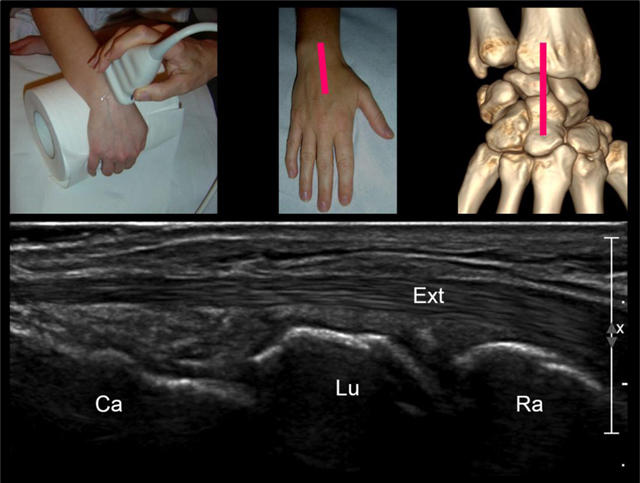
Figure 2
Step 1: sagittal view of the carpal bones along the long-axis of the third ray. (Ext = extensor digitorum tendon, Rad = radius, Lun = lunate, Sca = scaphoid).
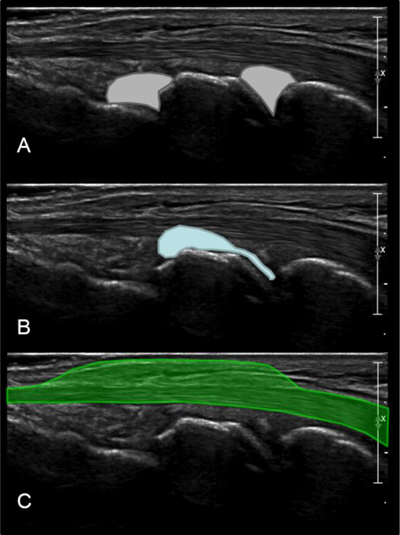
Figure 3
The role of the first sagittal view of carpal bones is to detect: (A) radiocarpal or mediocarpal joints effusions; (B) carpal ganglion cysts arising from the joint; (C) extensor tenosynovitis.
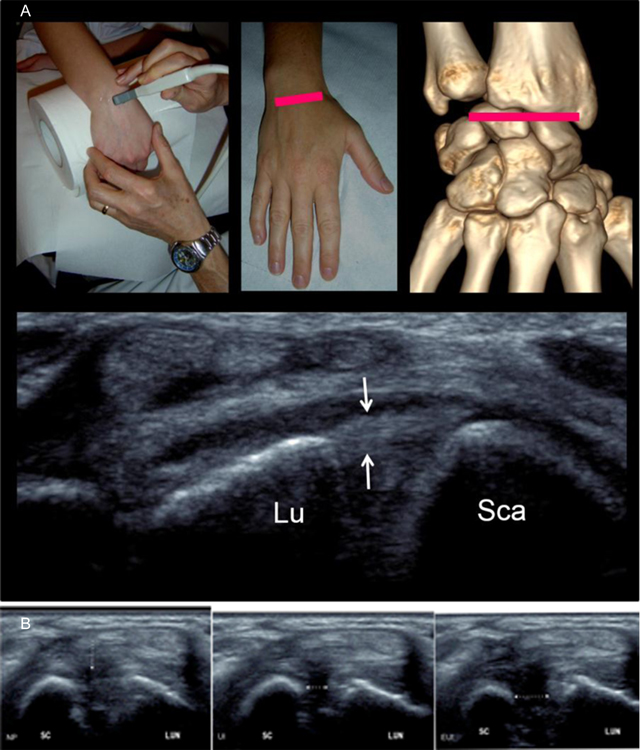
Figure 4
(A) Step 2 = axial view of the dorsal band of the scapholunate ligament. The scapholunate ligament (arrows) extends from the lunate (Lu) to the scaphoid (Sca) bones. (B) The aim of this second dynamic view is to look at: NP = a discontinuity of the dorsal scapholunate ligament in Neutral position (white arrow); UI = a nonvisualization of the ligament with an increased width of the scapholunate space in Ulnar Inclination (white arrow); EUI: a nonvisualization of the ligament with an increased width of the scapholunate space in Extreme Ulnar Inclination (white arrow).
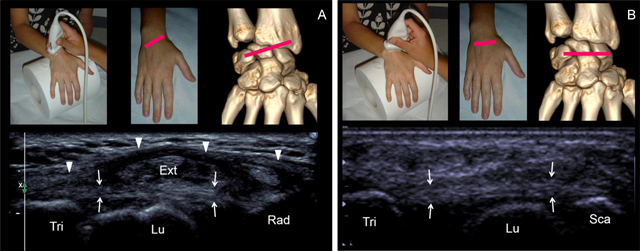
Figure 5
(A) Step 3 = Axial oblique view of the radiolunotriquetral ligament. The ligament (small arrows) extends from the radius (Rad) to the triquetrum (Tri), crossing over the lunate (Lu) without attaching. The radiolunotriquetral ligament is on continuation with the extensor retinaculum (Ext) (arrowhead). (B) Step 4 = Axial view of the scapholunotriquetral ligament. The ligament (arrows) extends from the scaphoid (Sca) to the triquetrum (Tri) crossing over the lunate (Lu) without attaching on.
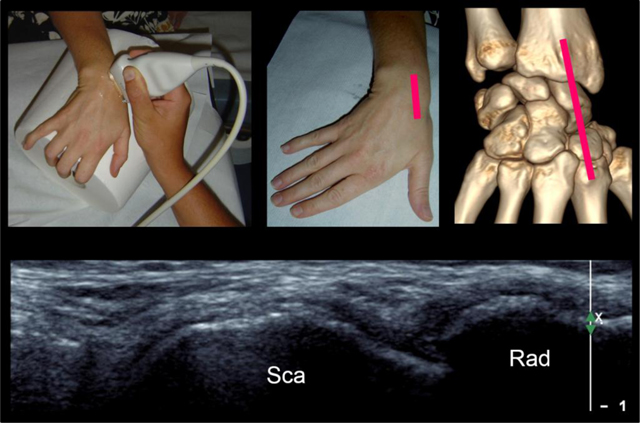
Figure 6
Step 5 = sagittal view of the dorsal cortex of the scaphoid with the wrist in ulnar deviation. Sca = scaphoid, Rad = radius.
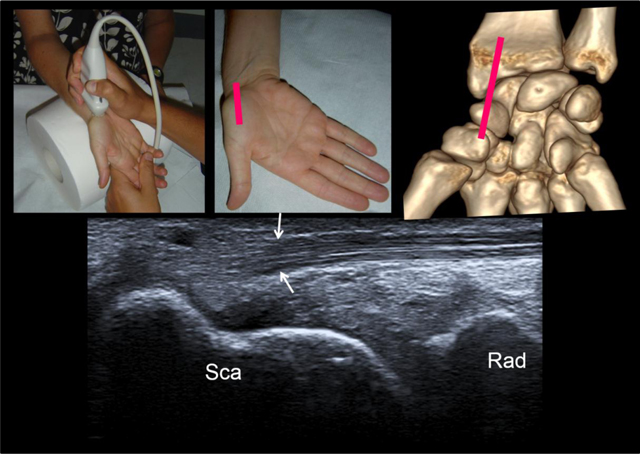
Figure 7
Step 6 = sagittal view of the palmar side of the scaphoid with the wrist in ulnar deviation. See the flexor carpi radialis tendon coursing anteriorly to the distal pole of scaphoid. This tendon then distally attaches on the base of the second and third metacarpals and the trapezium. Sca = scaphoid, Rad = radius.
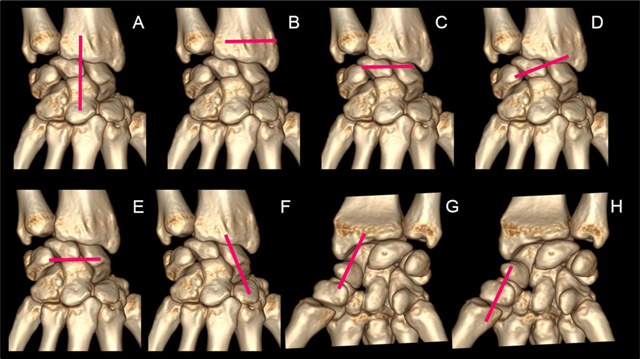
Figure 8
A 7-step standardized US examination framework for wrist injuries: (A) sagittal view of the carpal bones along the long-axis of the third ray. (B) localization of the Lister tubercle. (C) axial view of the dorsal band of the scapholunate ligament. (D) axial oblique view of the radiolunotriquetral ligament. (E) Axial view of the scapholunotriquetral ligament. (F) sagittal view of the dorsal cortex of the scaphoid with the wrist in ulnar deviation. (G) sagittal view of the palmar cortex of the scaphoid with the wrist in ulnar deviation. (H) sagittal view of the first ray (palmar aspect).
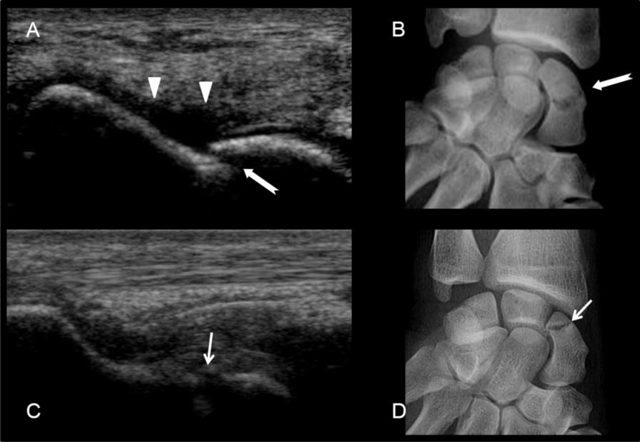
Figure 9
Scaphoid fractures. (A) and (B) transcortical fracture of the waist of the scaphoid. See the cortical disruption (white arrow) and the subperiosteal hematoma (arrow heads). (C) and (D) fracture of the proximal pole of the scaphoid with cortical disruption (small white arrow).
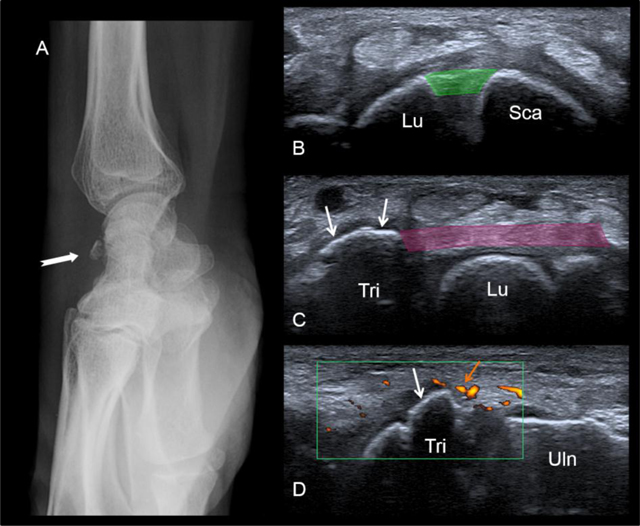
Figure 10
Bony avulsion of the dorsal sling (triquetral insertion). A fracture is seen on the lateral radiograph (A). At the US examination, the dorsal band of the scapholunate ligament (in green) is normal (B). In contrast US shows the bony avulsion of the triquetral insertion of the dorsal radiolunotriquetral ligament (white arrows). See the soft-tissue hyperemia surrounding the avulsion on the long-axis view (orange arrow). Lu = lunate, Sca = scaphoid, Tri = triquetrum, Uln = ulna.