
Table 1
Summary of shoulder neuropathy.
| Nerve involved | Sensory innervation | Motor innervation | Usual site of entrapment | Etiology |
|---|---|---|---|---|
| Suprascapular (C4)–C5–C6 roots | Acromioclavicular joint Glenohumeral joint Subacromial bursa | Supraspinatus and Infraspinatus | Suprascapular notch | Trauma, Microtrauma, Surgery, Extrinsic compression (cyst, tumour, varicose, etc.), Rotator cuff tears |
| Isolated Infraspinatus | Distal from suprascapular notch: spinoglenoid notch | |||
| Axillar C5–C6 roots | Glenohumeral joint Superior lateral brachial cutaneous nerve | Teres Minor and Deltoid | Quadrilateral space | Trauma (shoulder dislocation, humeral surgical neck fracture), Microtrauma, Surgery, Extrinsic compression (hematoma, posteroinferior labral cyst, bony callus, tumour, etc.) |
| Isolated Deltoid (anterior and middle heads) | Anterior branch | |||
| Isolated Teres Minor | ||||
| Isolated Deltoid (posterior head) | Posterior branch | |||
| Musculocutaneous (C4)–C5–C6 (C7) roots | Lateral antebrachial cutaneous nerve | Biceps Brachii- Coracobrachialis-Brachialis | Proximal coracobrachialis | Trauma, Microtrauma, Anterior shoulder surgery (Latarjet) |
| Long thoracic nerve (C4) C5–C6–C7 roots | / | Serratus Anterior (Winging scapula) | Scalenus medius muscle Second rib | Trauma, Microtrauma, Surgery (mastectomy, scalenectomy) Extrinsic compression (hematoma, tumour, etc) |
| Spinal accessory nerve (Cranial nerve XI–C1–C5) | / | Trapezus Sternocleidomastoid (Droopy Shoulder) | Posterior triangle of the neck | Trauma Microtrauma Surgery (radical neck tumour dissection, etc) Extrinsic compression (hematoma, tumour, etc) |
| Trapezus | Posterior to sternocleidomastoid muscle |
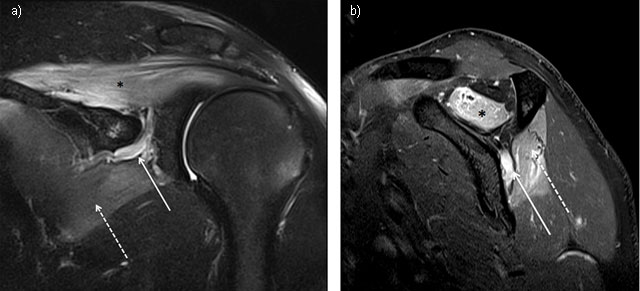
Figure 1
Suprascapular neuropathy at the scapular notch in a young judoka athlete showing typical edema denervation pattern of acute neuropathy on MRI. High signal intensity fluid is observed in fluid-sensitive sequences of both supraspinatus (star) and infraspinatus (dashed arrow). Notice the dilatation of suprascapular veins satellite (arrow). (1a = FIGURE 1 uploaded online manuscript) – Coronal (1b = FIGURE 2 uploaded online manuscript) – sagittal Short Tau Inversion recovery MRI (STIR) images.
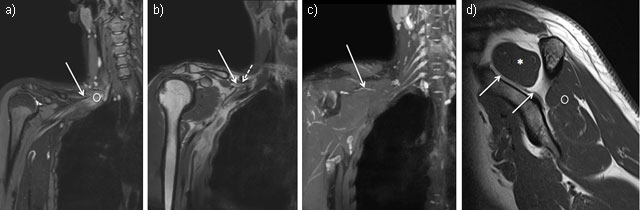
Figure 2
Coronal MR Neurography sections showing the right suprascapular nerve (solid arrow) arising from the upper trunk of the plexus brachial (circle) (2a = FIGURE 3 uploaded online manuscript) then, crossing the posterior cervical triangle in the supraclavicular fossa, deep to the omohyoid muscle (dashed arrow) (2b = FIGURE 4 uploaded online manuscript), before traveling through the suprascapular notch (2c = FIGURE 5 uploaded online manuscript). Sagittal MRI T1-weighted sequence shows the nerve inside the supraspinatus fossa where it provides motor innervation to the supraspinatus muscle (star) followed by infraspinatus muscle (circle) (2d = FIGURE 6 uploaded online manuscript).
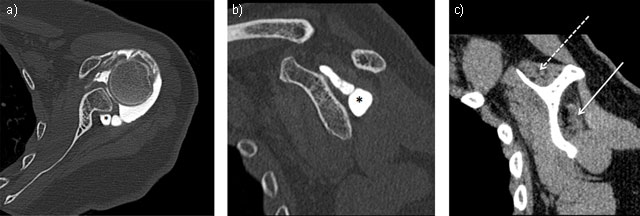
Figure 3
Neuropathy of suprascapular nerve by voluminous labral cyst (star) sited in spinoglenoid notch extending to supraspinatus fossa inducing a severe atrophy and fatty degeneration of infraspinatus (solid arrow) whereas the supraspinatus muscle is less involved (dashed arrow). Axial (3a = FIGURE 7 uploaded online manuscript) – sagittal (3b = FIGURE 8 uploaded online manuscript – 3c = FIGURE 9 uploaded online manuscript) CT Arthrography.
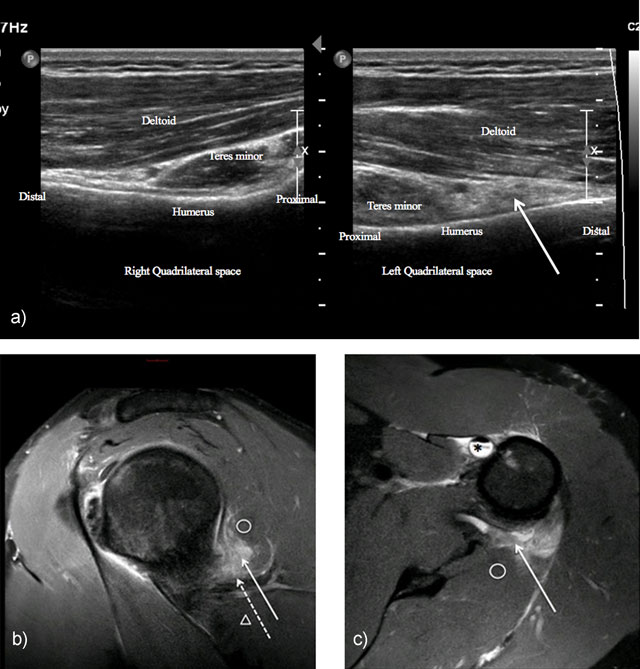
Figure 4
Neuropathy of axillary nerve after skiboard fall leading to injury of the shoulder capsule. Ultrasound showed infiltration of the axillary nerve (dashed arrow) in quadrilateral space (solid arrow) compared to normal side (4a = FIGURE 10 uploaded online manuscript), confirming by sagittal (4b = FIGURE 11 uploaded online manuscript), axial (4c = FIGURE 12 uploaded online manuscript) Proton Density with Fat Saturation MRI images. Note the concomitant Biceps brachii tendon injury (star). Teres minor muscle (circle) – Teres major muscle (arrowhead).
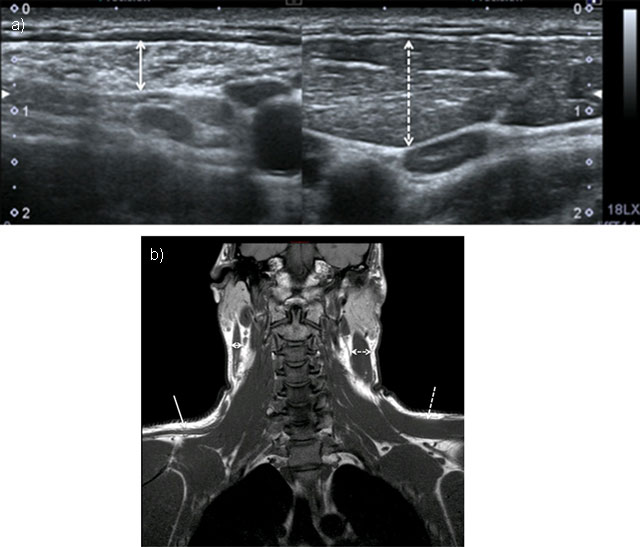
Figure 5
Chronic neuropathy of spinal accessory nerve. Ultrasound showed atrophy of sternocleidomastoid muscle (double solid arrow) compared to normal side (doubled dashed arrow) (5a = FIGURE 13 uploaded online manuscript), confirmed by coronal T1-weighted MRI showing both atrophy of trapezus (solid arrow) and sternocleidomastoid muscles compared to normal side (dashed arrow) (5b = FIGURE 14 uploaded online manuscript).