
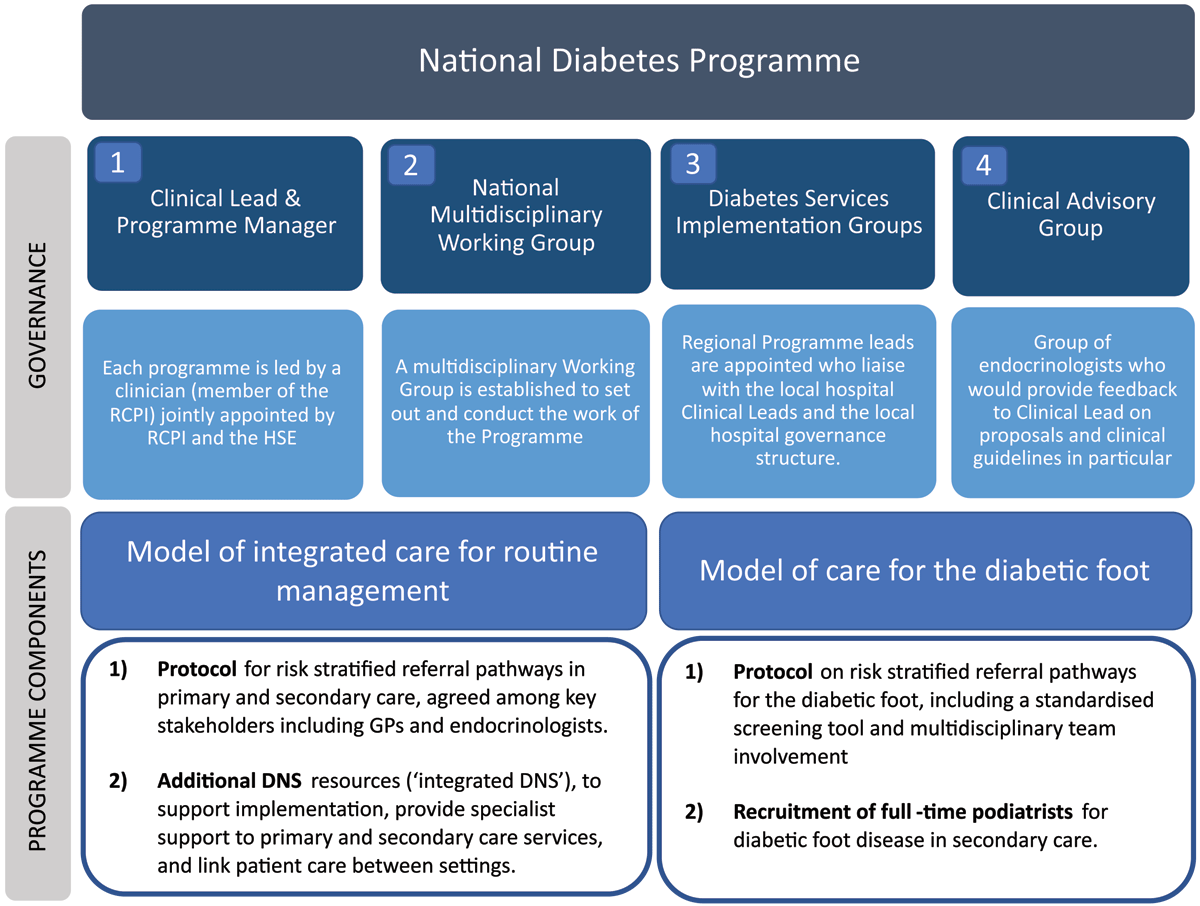
Figure 1
National Diabetes Programme.

Figure 2
Realist research cycle adapted with permission from Marchal et al. [34].
Table 1
Summary of CMOs.
| Overarching CMOC Varying levels of awareness about the programme (C), no planned approach to implementation (C), and professional oversight (C), and resource demands within the primary and secondary care health system (C) meant that it was more likely HCPs used their own professional judgment (M) to implement the models of care in ways that matched their priorities (O) with varying degrees of engagement (O) and implementation (O). | |
| CMOC 1: Weighing up the advantage of engagement in primary care | |
| Depending on their experience delivering diabetes care (C) and resource demands at each primary care practice (C), HCPs weighed up the relative advantage of the programme over their current approach to diabetes care (M) which led to variability in their willingness to engage with the programme (O). | |
| CMOC 2: Legitimising a new role in secondary care | |
| Given different levels of familiarity with the role of integrated DNS and podiatrists among existing HCPs (C), and depending on the availability of published protocols which provided guidance on the new roles (C), new HCPs recruited through the programme made judgements about how to legitimise their role (M) to engage HCPs with the programme and establish role boundaries (O). | |
| CMOC 3: Implementation; adjusting to fulfil immediate local need | |
| 3.1 Implementation in primary care Depending on HCP’s resources (C) or experience in diabetes (C), they felt more or less supported by the programme (M) and therefore, adapted the programme components to meet their immediate needs (O). | 3.2 Implementation in secondary care Depending on familiarity with the role of integrated DNS and podiatrists among existing HCPs (C), resources (C) and existing professional boundaries in secondary care (C), new HCPs recruited by the programme and secondary care HCPs made judgements about how to best adapt the role (M) to meet immediate service needs (O). |