
1. Introduction
Globally, smoking tobacco is a leading cause of preventable mortality and morbidity. In 2019, an estimated 7.69 million deaths annually were attributed to smoking (GBD 2019 Tobacco Collaborators, 2021). This death toll has been predicted to continue increasing due to growth in the global population and increasing smoking prevalence in some low-income regions (GBD, 2015).
The World Health Organization (WHO) Framework Convention on Tobacco Control (FCTC) (WHO, 2003) aimed to facilitate global, regional and country-level efforts to reduce tobacco-related harm. Ratified by 181 countries, the agreement compelled signatories to implement rules and standards to ‘protect present and future generations from the devastating health, social, environmental and economic consequences of tobacco consumption and exposure to tobacco smoke’.
The extent to which signatories have complied with the FCTC varies widely. Non-signatory countries have also implemented variations on the FCTC-directed tobacco control programme. Despite these efforts, smoking prevalence rates have fallen too slowly in many countries. Some regions, such as sub-Saharan Africa, are experiencing an increase in tobacco smoking prevalence (Brathwaite et al., 2015). Different strategies also appear to have differential effects by sex and for subgroups (Flor et al., 2021). For example, the WHO noted that people with mental health conditions, marginalised groups and Indigenous People appear to have been ‘left behind’ by the usual FCTC-directed programmes (Glover, Patwardhan and Selket, 2020).
Greater progress could be achieved if tobacco control programmes were better tailored to each country’s context. The FCTC acknowledges this; for example, Article 14 implementation guidelines recommend that when developing and disseminating ‘demand reduction measures concerning tobacco dependence and cessation’, each party takes ‘into account national circumstances and priorities’ (WHO, 2013a, p. 5).
1.1 FCTC alignment with United Nations Declaration on the Rights of Indigenous Peoples
Concern was expressed in the FCTC preamble about disproportionately high smoking prevalence and other methods of tobacco use among Indigenous Peoples. To address this concern, promoting ‘the participation of indigenous individuals and communities in the development, implementation and evaluation of tobacco control programmes that are socially and culturally appropriate to their needs and perspectives’ is recommended in the guiding principles for Article 4 (WHO, 2003, p. 6). Many FCTC signatories are also parties to the United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) passed by the General Assembly in 2007 (UN General Assembly, 2007). A total of 144 countries voted in favour of the UNDRIP, including many that have no recognised Indigenous populations. Australia, New Zealand, Canada and the United States initially voted against the declaration but have since adopted it.
The UN estimates that 6% of the world’s population, about 476 million people, are Indigenous (Dhir et al., 2020). Reducing inequalities in smoking prevalence between Indigenous and non-Indigenous populations should be a priority for all UNDRIP signatories, especially those with Indigenous People within their borders.
The UNDRIP states that Indigenous people have the right to maintain their traditional way of life and develop their culture. This includes protection of their cultural heritage, including tobacco and other nicotine-containing plants, which are used as part of a traditional practice among some Indigenous Peoples. To respect and support this right, tobacco control policies and interventions should focus on smoking and high-risk chewing tobacco products that are mass-manufactured by government-owned, multinational and supranational commercial companies (Fuller, 1983). Tobacco growing, manufacture and use that are part of an Indigenous Peoples’ traditional way of life should not be a target. Similarly, vaping, snus and other tobacco or nicotine products that present a significantly lower risk to health as compared with smoking tobacco (Royal College of Physicians, 2016; Fagerström, 2022) and which are effective smoking cessation aids (Lindson et al., 2024; Tuisku et al., 2024) should be supported to assist reduction in smoking prevalence.
One of the first steps for determining an effective and appropriate country-level tobacco control programme is to determine tobacco use across the population, including among subgroups (WHO, 2013b). The importance of data is supported by the UNDRIP, which affirms that Indigenous People have the same human rights and freedoms as anyone else, including the right to improvement in health care (UN General Assembly, 2007). Necessary to this, Indigenous Peoples ‘require information about their citizens, territories, and resources just like any other nation state’ (Walter and Rodriguez-Lonebear, 2019). Globally, Indigenous People bear a greater burden of disease and morbidity, and this is underpinned by the lack of knowledge on Indigenous health (Curtice and Choo, 2020), a phenomenon that has been labelled as ‘epidemiological invisibility’ (Rodrigues, 2018).
As a leading cause of illness and premature death, smoking is a key indicator of health that should be monitored and reported for Indigenous Peoples. This research aimed to identify the current state of that reporting and the smoking prevalence among all Indigenous Peoples.
2. Methods
2.1. Study design
The aims of this exploratory qualitative study were to identify 1) Indigenous Peoples living in recognised countries; 2) smoking prevalence data by ethnicity, specifically prevalence data for the resident Indigenous People; and 3) country economic status, FCTC party status and UNDRIP adoption status. An iterative investigative online search strategy was used to identify definitive, globally focused sources. Searches, including those conducted by a second research assistant to validate extracted data and a final search for updated data, were conducted from February 2019 to February 2021.
2.2. Defining Indigenous
While the term ‘indigenous’ has long been used as a generic term, there is no globally agreed-upon definition of Indigenous Peoples. The UN conceptualises Indigenous Peoples as those who self-identify as Indigenous at an individual level and are accepted by their community as members. Additionally, such communities have ‘historical continuity’ with strong links ‘to territories and surrounding natural resources’ that predate colonisation by a ‘settler’ society. They also possess ‘distinct social, economic, or political systems,’ as well as a distinct language, culture, and beliefs. Despite being a non-dominant group in society, they demonstrate a ‘resolve to maintain and reproduce their ancestral environments and systems as distinctive peoples and communities’ (UN Permanent Forum on Indigenous Issues, 2006).
Restricting identification as Indigenous to non-dominant groups in society has been challenged, as groups that are numerically dominant but meet all other criteria for indigeneity are excluded from claiming rights recognised in instruments such as the UNDRIP. Predicating a people’s status as Indigenous on their population size relative to their non-Indigenous counterparts shifts the focus away from the concept of being ‘first peoples’ and reframes it as a matter of minority status within a multi-ethnic society (O’Sullivan, 2017). However, indigeneity is not inherently tied to minority status. For example, postcolonial stability in Fiji has experienced challenges due partly to demographic changes that reduced the dominant proportion of the iTaukei (Indigenous) people relative to the Indo-Fijian population, leading to political demands that threatened the iTaukei way of life (O’Sullivan, 2017). Furthermore, the use of the collective term ‘Indigenous’ can obscure the fact that some groups prefer to be identified by the names they use for themselves (UN Permanent Forum on Indigenous Issues, 2006).
Our selection criteria for indigenous status were that Indigenous Peoples were ‘officially’ recognised in their country or at an international level, they self-identified as indigenous and they were or had been the predominant people resident and holding sovereignty in a geographical area prior to a different ethnic group moving in or taking over and gaining dominance over the governance of the area (restricted to colonisation and invasions that occurred around, and after, the time of expansion by the Ottoman Empire and by European powers c. 1500). In some places, the colonising group was a neighbouring group indigenous to their area. For example, the Sámi are an Indigenous People of the circumpolar region; their traditional land stretches across land now governed by four countries: Norway, Sweden, Finland and Russia. This definition corresponds to UN guidelines (Walter and Rodriguez-Lonebear, 2019). Descriptive characteristics of each country and a summary of the colonial history are available elsewhere (Glover and Selket, 2021).
2.3. Data searches
We started with The Indigenous World, which lists 62 countries with Indigenous Peoples (Berger, 2019). To identify more countries, we searched the International Work Group for Indigenous Affairs website, Indigenous-focused UN sites and Google using the search terms ‘indigenous’ and ’smoking’.
Searching online for smoking prevalence data by country is not unprecedented (Jha et al., 2002). For each country identified with Indigenous Peoples, we conducted English-language searches of Google Scholar (our main search engine) for the most recent determination of smoking prevalence among males and females in the general population and disaggregated by ethnicity. For comparability, we also searched WHO country data; where absent, we used the daily smoking rates provided by the Tobacco Atlas (https://tobaccoatlas.org/) or relevant national health authority reports. We focused only on tobacco smoking, as the majority of tobacco-related morbidity and mortality is caused by smoking (Nutt et al., 2014). Citations for statistics reported in articles and the reference lists were read to identify government-reported statistics and additional sources in order to identify the most robust source of data and data disaggregated by sex.
World Bank data (World Bank, 2024) was used to determine country economic status (high, upper-middle, lower-middle, low and financially dependent). The FCTC and UNDRIP websites were searched to determine current party and adoption status.
2.4. Data analysis
Extracted information was entered into Excel and used to create short country profiles (Glover and Selket, 2021). This paper presents additional results of an inductive content analysis of the existence (non-existent) and type of source of reporting (sporadic researcher-led studies, indicative, existing) on smoking prevalence among Indigenous Peoples. Some information on countries with non-existent data included that disaggregation of national statistics by ethnicity was not supported by the government. These were categorised as suppressed. The data file is available on Zenodo.org (https://zenodo.org/records/14626472).
3. Results
3.1. Reporting of smoking prevalence
One hundred and five countries had Indigenous populations within their current-day borders. Reporting of disaggregated data on smoking prevalence among the Indigenous Peoples ranged from there being no data to collection and reporting being FCTC and UNDRIP compliant. For example, one systematic review on health indicators for tuberculosis among Indigenous People (Cormier et al., 2018) had data for many Indigenous populations, but other studies were more anecdotal. We identified five categories of prevalence data reporting: non-existent, sporadic researcher-led studies, indicative, existing and suppressed. Supplementary Table 1 presents an alphabetised-by-country summary of the results.
Data on smoking among Indigenous Peoples was non-existent for 66 (62.9%) countries. Data on smoking prevalence was available, but this was not disaggregated by ethnicity. Many of these countries had a lower-middle-income or low-income economic status.
Eight (7.6%) countries had no identifiable official data on smoking among Indigenous Peoples, but searches of scientific literature found some researcher-led studies reporting on smoking prevalence among some Indigenous Peoples, though sporadically.
In 17 (16.1%) countries, the Indigenous People made up a substantial majority of the country. Although the officially collected smoking prevalence data was not reported by ethnic group, the national smoking prevalence was indicative of the smoking rate for the Indigenous majority.
The governments of only 5 (4.7%) countries—New Zealand, Australia, Canada, United States and Fiji—were routinely monitoring and reporting smoking prevalence by ethnicity. These countries had high economic status, except for Fiji (high-middle).
Eight (7.6%) countries actively suppressed either the collection of data by ethnicity or the reporting of it.
3.2. Smoking prevalence reported among Indigenous Peoples
We found smoking prevalence data reported for Indigenous Peoples in only five countries. In Canada, prevalence had been found to be significantly higher (2–3 times) for First Nations, Inuit and Métis community members than for non-Indigenous populations (Bougie and Kohen, 2017; Garner et al., 2010). The prevalence of daily smoking was similar among Inuit men and women. This contrasted with the national average in Canada, where men were more likely to smoke than women (Garner et al., 2010).
In the United States, current cigarette smoking prevalence was higher in non-Hispanic American Indians/Alaska Natives (20.9%) than in White (15.5%) or Black (14.9%) non-Hispanics in 2020 (Cornelius et al., 2020). There were, however, wide regional disparities. From 2000–2009, for example, cigarette smoking prevalence was more than twice as high in Northern Plains American Indians (42.1%) as in American Indians in the Southwest (18.8%) (Kunitz, 2016).
In Fiji, daily smoking rates in 2011 for iTaukei males (27.0%) and non-indigenous Indo-Fijian males (26.3%) were similar. However, iTaukei females (9.5%) had a higher smoking prevalence than Indo-Fijian females (1.3%) (Figure 1a; Linhart et al., 2017).
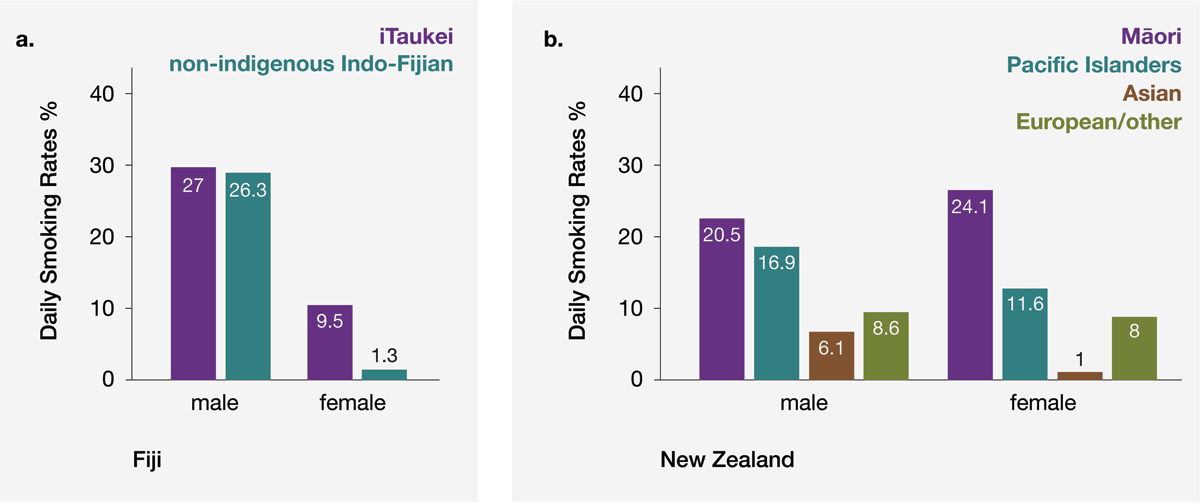
Figure 1
Examples of higher smoking prevalence in Indigenous People compared with the non-Indigenous population. a) Fiji with iTaukei people (Linhart et al., 2017). b) New Zealand Māori people compared with other ethnic groups (Ministry of Health NZ, 2021).
By contrast, Indigenous Australians were found to have a higher daily smoking prevalence than the national average (27% and 11.0%, respectively). However, the sample size was small, and the results were aggregated for all Indigenous Peoples represented (Australian Institute of Health and Welfare, 2019).
Lastly, New Zealand Māori were found to have a higher smoking prevalence than the national average for both males and females (Figure 1b). A higher percentage of Māori women than men smoke, which was unusual among non-Indigenous populations. Daily smoking rates in 2020 for men and women, respectively, were 20.5% and 24.1% among Māori, as compared with 16.9% and 11.6% among Pacific Islanders, 6.1% and 1.0% among Asians and 8.6% and 8% among Europeans/other (Ministry of Health NZ, 2021).
4. Discussion
The aim of this study was to determine tobacco smoking prevalence among all Indigenous Peoples across the world. Of 105 recognised countries identified to have Indigenous Peoples, only five routinely collected smoking prevalence data by ethnicity. Using inductive content analysis of our search results, we were able to identify five categories of smoking prevalence reporting for Indigenous Peoples: non-existent, sporadic researcher-led studies, indicative, existing and suppressed.
Among the eight countries with suppression of prevalence data, the type of suppression varied. Some countries actively opposed and subverted recognition of Indigenous Peoples (as is reportedly occurring in, for example, Algeria (Berger, 2019), Indonesia (Mamo, 2020), Myanmar (Berger, 2019) and the People’s Republic of China (Berger, 2019)). Some countries did not acknowledge the separate existence of Indigenous Peoples (for example, in Vietnam and Rwanda) (Berger, 2019). Finland (Statistics Finland, 2021) and Sweden (Public Health Agency of Sweden, 2018) acknowledged Indigenous People, but government agencies did not gather or report demographic data disaggregated by ethnicity. Consequently, it was not possible to obtain data on smoking prevalence among the Sámi people living in these nations. This contributes to a common issue in public policy, the silencing or discounting of Indigenous voices (Curtice and Choo, 2020; Rodrigues, 2018). Yet, all countries with active data suppression, except Rwanda, had adopted the UNDRIP.
Because government data were available for only five countries (Australia, Canada, Fiji, New Zealand and the United States), it was hard to draw clear conclusions on smoking prevalence among Indigenous Peoples, the original aim of the study. Overall, where reported, smoking prevalence was disproportionately higher among the Indigenous Peoples. Where more than one Indigenous People was surveyed, there were differences between ethnic groups. Among the general population in most countries, more men than women smoked. This can be contrasted with the case among Indigenous People who smoked, where there was a higher prevalence of women who smoked, and in some cases a higher prevalence of women than men who smoked. Our data are consistent with an Australian study on smoking prevalence specifically among secondary students (12–17 years), which found that both smoking and intent to smoke were more prevalent among Indigenous than among non-Indigenous students between 1996 and 2005 (White, Mason and Briggs, 2009).
Among countries with researcher-led data, it was difficult to come to any conclusions about the current smoking status among the Indigenous Peoples. A systematic review in English and Russian for Russia found 11 studies where the smoking prevalence of different Indigenous groups had been surveyed. However, all but three of these studies had limitations in methodology or sampling criteria (Merkin et al., 2021).
Similarly, a systematic review on low birth weights and maternal smoking among Indigenous People reported a similar difficulty in obtaining robust data (Baretto et al., 2019). Most of the studies came from Canada, the United States and Australia, with a few from Latin America, a region with a vast number and diversity of Indigenous Peoples. There were difficulties in accurately measuring smoking prevalence and numbers of cigarettes smoked due to the different ways people smoke tobacco. There was also a lack of consistency in the way that researchers recognised indigeneity.
Smoking prevalence rates for other countries for which comparative data were available (Baretto et al., 2019; Bong et al., 2020; Cormier et al., 2018) showed a higher smoking prevalence among small samples of Indigenous groups in most but not all cases. In some cases, the smoking prevalence was lower than the non-Indigenous population (Cormier et al., 2018).
Many of the countries for which data were non-existent or sporadic probably face challenges collecting or reporting data due to, for example, lack of resources and infrastructure (Adebisi and Lucero-Prisno, 2022), civil unrest, mass displacement and other factors (Hoogeveen and Pape, 2020).
4.1 Limitations
Our main aim to report smoking prevalence among Indigenous Peoples worldwide was hampered by the lack of data available in the relevant countries and other study limitations. The type of source of smoking prevalence data varied. Some prevalence rates were drawn from scientific studies, some from government WHO reports and some from the Tobacco Atlas, which reports daily smoking rates. As we and others have found, there is a lack of consistency in the regularity with which countries monitor smoking prevalence, the definitions used to categorise consumption, for example, daily versus ‘regular’ smoking and the type of smoked tobacco product used (Jha et al., 2002). How studies and governments collect data on smoking (nationally representative versus a specific area) and what age range they survey also vary (Storr et al., 2014). Some studies estimate country or world smoking prevalence rates (Storr et al., 2014). Caution is needed when comparing across countries, as regions vary in terms of which stage of the tobacco epidemic they are experiencing, the existence of government-owned tobacco companies and varied cultural contexts. Further, we conducted online searches only in the English language. Research data may be available in local languages, and some of it may not be available online. More comprehensive and robust data on smoking prevalence, especially for the majority of Indigenous Peoples, is needed before generalised statements about smoking among Indigenous Peoples are made. Such statements could encourage stereotyping of Indigenous Peoples and minimise the diversity that exists between them.
In the five countries where regular disaggregated data collection was reported, the Indigenous People had a disproportionately high smoking prevalence (in women only in the case of Fiji). Of these, New Zealand, Australia and Fiji were colonised by the British. In the United States, the regional disparities in Indigenous communities in the north and the southwest have been attributed to more aggressive policies supporting the growth of the tobacco trade by the French in the north compared with the Spanish colonial powers in the south. As a result, northern populations more quickly switched from the traditional pipe to commercially produced cigarettes (Kunitz, 2016). To enable adaptation of the FCTC to local cultures and socio-political environments, it might be useful to understand how different colonisation histories and economic factors over the 20 years of the FCTC have influenced tobacco harm reduction policies and resulting smoking prevalence among the affected indigenous populations. To inform this, future research could investigate the evolution from traditional tobacco use (Pereira et al., 2022) to the more ubiquitous Western commercialised tobacco products in places such as the Americas and Australia, where Pituri, a nicotine-containing plant, was used by Aboriginal tribes (Ratsch, Steadman and Bogossian, 2010).
4.2 Recommendations
Reliable data on health disparities and colonisation history would help to lessen the epidemiological invisibility of Indigenous Peoples (Rodrigues, 2018; Curtice and Choo, 2020). Responsible use of data on Indigenous Peoples is a cornerstone of the CARE principles for Indigenous data governance by The International Indigenous Data Sovereignty Interest Group (Carroll et al., 2020). Regular collection and reporting of these data should be commissioned or led by government agencies using standardised methods to determine smoking consumption and indigeneity (Baretto et al., 2019) and disaggregated to reflect all Indigenous Peoples. Because there are interactions between sex, indigeneity, regional history and smoking prevalence (Linhart et al., 2017; Ministry of Health New Zealand, 2021; Rodrigues, 2018), data should be collected and reported in different regions for males and females separately. For countries that have signed both the FCTC and UNDRIP, this would align with the expectation that they will recognise the existence of different Indigenous Peoples when monitoring health and that they will collect disaggregated data on smoking.
Higher-income countries with stable governments that have signed the UNDRIP and FCTC need to ensure that they collect reliable disaggregated data for each of the Indigenous Peoples living in the country. The FCTC also requires all country signatories, whether or not they have Indigenous communities within the current nation borders, to provide technical and financial assistance to lower-income countries to enable the collection of such data.
In the 17 countries with a high proportion of Indigenous People, national average smoking prevalence provides a useful first approximation of smoking prevalence for the Indigenous People. However, in countries with a large number of distinct Indigenous Peoples, such as Somalia and Papua New Guinea, more detailed collection of data and analysis would be needed.
Culturally tailored smoking reduction interventions may be more effective for Indigenous Peoples than programmes designed for the often politically and numerically dominant non-Indigenous groups (Leinberger-Jabari, et al., 2023). In support of the FCTC’s guidance to consider national circumstances and priorities, evidence that this should be heeded may be found in New Zealand (Rutter and Walker, 2021), Fiji (Groth-Marnet, Leslie and Renneker, 1996), Taiwan (Lin et al., 2013), the United States, and Australia (Minichiello et al., 2016).
As a first step towards designing effective smoking cessation programmes to reduce use of harmful tobacco products, robust data on smoking prevalence in indigenous populations is needed. Such data require a broad geographical reach that includes all Indigenous People present in urban and rural areas. The data need to have a sufficient population size to detect differences by sex, age, income level, rurality, region and access to culturally effective smoking reduction interventions or treatments.
Data accessibility statement
The Supplementary Table 1 data file is available at: https://zenodo.org/records/14626472.
Acknowledgements
I am grateful to the Centre staff and many casual research assistants who assisted with online searches, extraction of information and development of the data used in this study.
Funding Information
This study was funded with a grant [COE1–009] from Global Action to End Smoking (formerly known as Foundation for Smoke-Free World), an independent U.S. nonprofit 501(c)(3) grantmaking organisation, accelerating science-based efforts worldwide to end the smoking epidemic. Global Action played no role in designing, implementing, data analysis, or interpretation of the study results, nor did Global Action edit or approve any presentations or publications from the study. Through September 2023, the organisation received charitable gifts from PMI Global Services, Inc. (PMI) while operating as an entirely independent entity. In October 2023, the organisation ended its prior funding agreement with PMI. Global Action has since adopted a formal policy that it will not seek or accept funding from any industry that manufactures tobacco products or non-medicinal nicotine products. The contents, selection and presentation of facts, as well as any opinions expressed, are the sole responsibility of the authors and should not be regarded as reflecting the positions of Global Action to End Smoking.
Neither the author nor the Centre has any commercial interests in any smoking cessation programs or aids or nicotine or tobacco products.
Competing Interests
This study was conducted by the Centre of Research Excellence: Indigenous Sovereignty & Smoking, an independent research company, as part of a wider programme of research aimed at building scientific knowledge on how to reduce tobacco-related harms among Indigenous Peoples. The funding for that programme of work was obtained following submission of a researcher-initiated application for funding from Global Action to End Smoking (formerly known as Foundation for Smoke-Free World). Global Action to End Smoking had no involvement in the conception, design, analysis or writing of the study results, nor did they have any input into the decision to publish. That is, this study was not commissioned by Global Action to End Smoking. Neither the author nor the Centre of Research Excellence: Indigenous Sovereignty & Smoking has any commercial interests in vaping, snus, oral nicotine, tobacco or cannabis products. Dr. Glover has, over 10 years ago, received fees from pharmaceutical companies for consultancy regarding cessation medicines.
Author Contributions
Marewa Glover: Conceptualization, Funding Acquisition, Methodology, Project Administration, Analysis, Writing – Original Draft, Writing – Review & Editing.
Author Information
Marewa Glover is an Indigenous Māori professor of public health. She has worked across several roles as a government policy analyst, national Smokefree Co-ordinator and academic for 30 years to reduce smoking among the Indigenous People of New Zealand. Professor Glover has over 100 scientific journal articles. In 2019, she was a finalist for the prestigious New Zealander of the Year Award in recognition of her contribution to improving Māori health.