
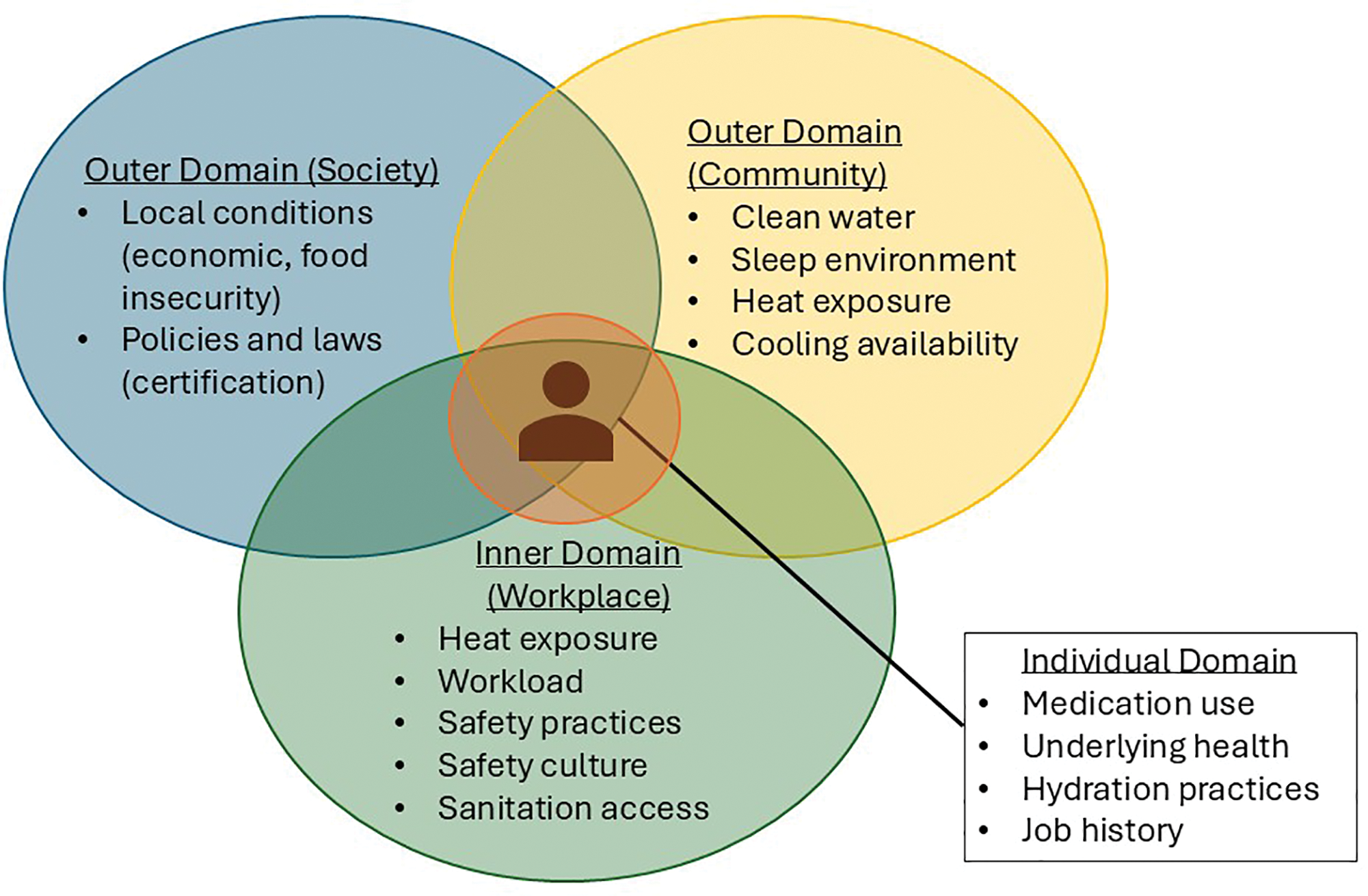
Figure 1
Framework for developing heat‑associated CKDnt interventions for the workplace using the Total Worker Health approach.
Table 1
Individuals and roles involved in the delivery of TWH interventions to address CKDnt in the workplace.
| INDIVIDUALS | ROLE |
|---|---|
| Corporate leadership (sustainability, HR, C‑level) | Decision‑making Resource allocation Establishing health and safety as a corporate priority Communications Logistical support |
| Local leadership (on‑site company leadership, occupational safety and health) | Decision‑making, implementation leads, innovation deliverers, Interpretation of results |
| Centers for Health, Work & Environment researchers | Research design leadership Innovation deliverers Logistical support Implementation team members Collaboration building Workforce capacity building Evaluation and identification of evidence base Data analysis and interpretation Communication of results to partners, leadership, stakeholders |
| Local research staff | Other implementation support |
| Field managers (field worker supervisors) | Innovation deliverers, problem‑solving Local communications Integration of health and safety priority into work processes |
| Local medical staff | Innovation deliverers Communication with workers Research design contributors Implementation deliverers |
| Field workers (sugarcane harvesters) | Innovation recipients Contributors to design elements (e.g., choices of personal protective equipment, types of electrolyte solution) |
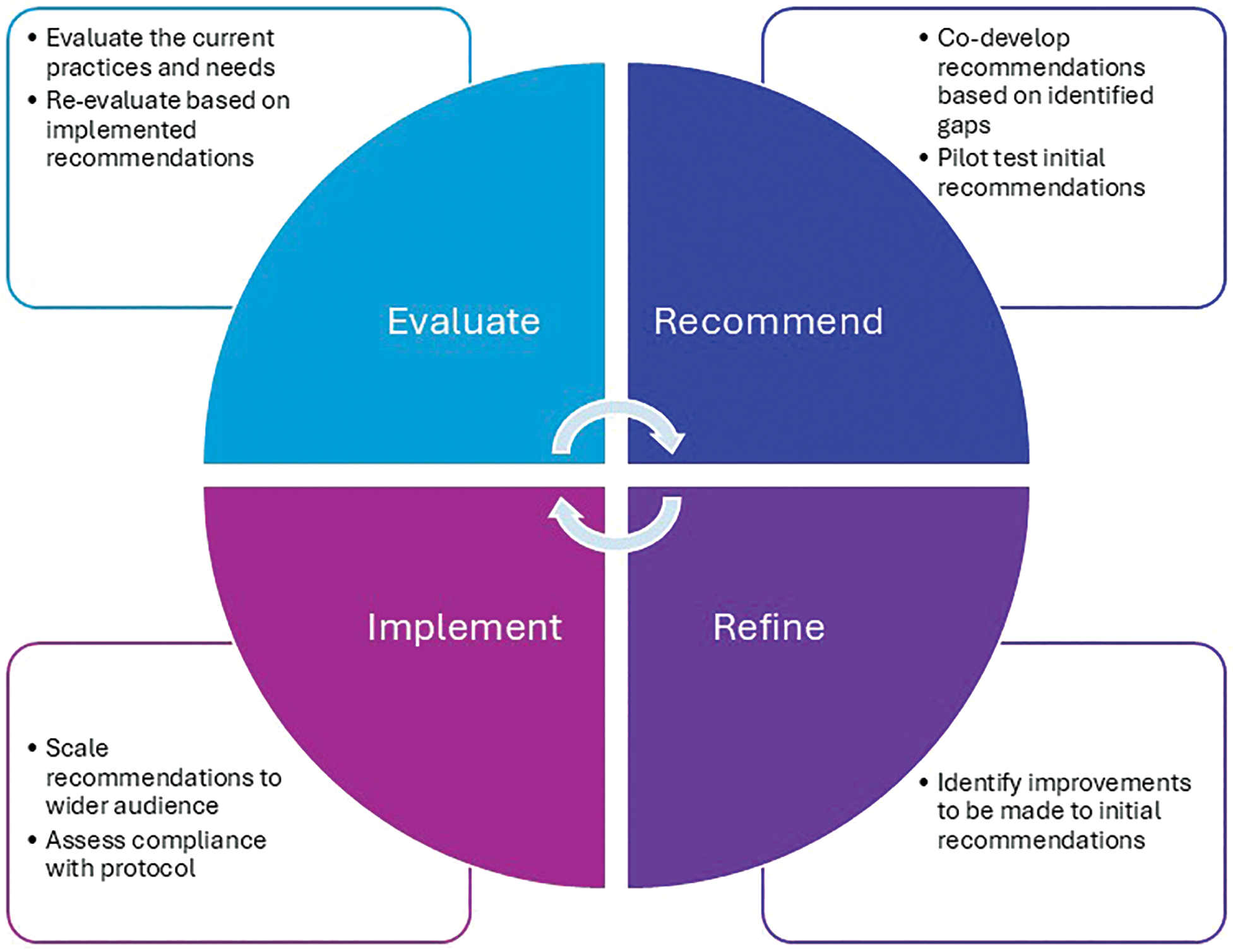
Figure 2
Approach to continual CKDnt intervention improvement.
Table 2
Summary and results of TWH interventions to address CKDnt prevention strategies focused on the individual, workplace, community, and societal domains.
| TWH INTERVENTION* (HARVEST SEASON) | DESCRIPTION/INTERVENTION DESIGN (TWH DOMAIN) | INTERVENTION SELECTION | IMPLEMENTATION OUTCOMES |
|---|---|---|---|
| Worker heat stress education program (2016–2017) | Augmented current worker education program to include the importance of hydration, rest, and shade and the need to moderate their use of NSAID. Trained Pantaleon nurses to provide education through face‑to‑face communication, posters, and pocket urine color charts for hydration status self‑evaluation in Spanish and adapted to low literacy. (Individual) | Evidence Base: OSHA Water, Rest and Shade program Relative Advantage: Workers and supervisors have knowledge of the importance of hydration and shaded rest breaks. Adaptability: Educational materials were adapted for low literacy. Trialability: Straightforward Complexity: Straightforward Cost: Minimal; printing costs and time for education delivery (< 5 minutes) Organizational behavior change: Transactional | Reach: 517 sugarcane workers participated in the initial study. Implementation: Delivery of the intervention was driven by field nurses, as it was integrated within their existing educational program. Therefore, the approach was designed to be feasible and culturally acceptable in this setting from the outset. Effectiveness: Workers demonstrated greater understanding of the signs and symptoms of dehydration [40]. Adoption: The program was rolled out company‑wide to also include workers inside the processing mill and in other heat‑exposed, non‑field operations. Maintenance: Health and safety personnel at the company conduct random urine checks with workers throughout the harvest. The heat stress education program continues to be an integral component of the education program delivered daily by the nurses. |
| Wellness Incentive (2016–2017) | Workers who started the shift hydrated (urinary specific gravity was ≤ 1.020) or who maintained or improved their hydration across the shift (< 1% body weight loss) were entered into a raffle to win prizes (e.g., soap, socks, soccer balls). Those not considered hydrated received additional education to drink more water and take more rest. (Individual) | Evidence Base: Incentives are an effective way of affecting healthy behavior in workplace settings. Relative Advantage: Promotes hydration among workers, both on and off‑work Adaptability: Ability to adjust to the number of workers and their needs of water and electrolyte consumption. The incentive raffle is a useful employee engagement tool that was later adapted for use in other projects in this setting given its success here. Trialability: Was carried out with 10 working groups Complexity: Straightforward Design: Cross‑sectional and longitudinal Cost: Costs minimal; dependent on local pricing of incentives Organizational behavior change: Transactional | Reach: 517 workers Implementation: The raffle was popular and well‑accepted by participants Effectiveness: The percentage of workers who were dehydrated at the beginning of the workday was reduced [41]. The percentage of those dehydrated at the end of the shift was already low (2%) and remained unchanged. Adoption: Workers were consuming too much plain water and not enough electrolytes, indicating a need to refine the intervention [42]. Maintenance: The incentives were not continued after the intervention, but the company continues to invest resources in hydration programs. |
| Electrolyte Study (2017 –2018) | A three‑week study that progressively increased the recommended volume of electrolyte solution for workers to consume. Pantaleon was responsible for providing workers with the recommended volume of electrolyte solution. (Individual, Workplace) | Evidence base: NIOSH recommendations Relative advantage: Workers were able to replace needed electrolytes lost in sweat. Adaptability: WHO rehydration solution formula was followed and produced locally for the intervention. Trialability: Was able to be piloted with a single work group Complexity: Straightforward Design: Longitudinal (3 weeks including baseline) Costs: Laboratory costs associated with health monitoring (blood and urine), pre‑ and post‑intervention, survey development | Reach: 50 of the workers participated in the intervention (1 complete work group/turma) Implementation: Dislike of certain flavorings expressed among workers Effectiveness: When workers increased electrolyte solution consumption, they experienced less muscle damage and less self‑reported weakness [43]. Kidney function was maintained. Serum electrolyte balance achieved. Adoption: The electrolyte solution was provided to workers in powder form to facilitate widespread distribution of larger quantities of electrolytes across the company’s farms (previously the solution had been pre‑mixed in 500 ml pouches) Maintenance: Continuous evaluation is needed to ensure access to the recommended quantities of electrolytes, and that expected health effects are maintained. |
| 6‑Hour Workday Study (2017–2018) | A three‑week study that reduced the number of hours a group of harvesters worked. Daily hours were reduced from 8 to 6. Supervisors at Pantaleon were responsible for ensuring the recommended schedule was adhered to. (Workplace) | Evidence Base: OSHA recommendations [44] Relative Advantage: Reduces the number of hours workers are exposed to heat Adaptability: Ability to adjust the number of reduced hours to meet the needs of the company. Trialability: Was able to be piloted with a single work group Complexity: Straightforward Design: Comparative effectiveness trial Cost: Laboratory costs associated with health monitoring (blood and urine), pre‑ and post‑intervention, survey development; may result in reduced productivity. Organizational behavior change: Transactional | Reach: 50 of the workers participated in the intervention (92% of eligible, 1.6% of the total workforce) Implementation: Potential issues with adherence to the recommended schedules. Effectiveness: No observed effect on post‑shift measurements of kidney function or incidence of acute kidney injury. Less muscle breakdown was observed during the weeks with the shortened shift. Workers on average produced less sugarcane during the shorter shifts. Adoption: The pilot intervention was trialed in one of 49 workgroups (2%). Maintenance: Was not continued after pilot. Pantaleon is currently considering schedule refinements and re‑evaluation of reduced schedules and/or earlier shift start times to avoid the hottest times of day. |
| Mid‑Harvest Season Screening (2017–2018) | Workers’ kidney function was evaluated mid‑way through the harvest to identify: (1) abnormal kidney function group, (2) reduced kidney function group, and (3) normal kidney function group. Those with reduced or abnormal kidney function were referred to the occupational medicine physician employed by Pantaleon. Based on the severity of the abnormal kidney function reading, workers either received consultation and one‑on‑one education and were re‑tested 2 weeks later, or they were referred to the local nephrologist or hospital and removed from work. The company continued to pay their wages for the rest of the season. Those with stable or improving kidney function continued to work in jobs with lower physical demands and lower heat exposure (Workplace, Society). | Evidence Base: Occupational health surveillance Relative Advantage: Identifies health conditions closer to onset to identify preclinical decline of kidney function and allow for work modification and clinical care for affected workers Adaptability: Can modify the timing of screening Trialability: Dependent on the incidence of disease Complexity: Straightforward Design: Cross‑sectional Cost: Equipment costs for point‑of‑care testing, personnel to conduct screenings and review results. Costs increase with severity and number of cases identified. Potential impact on job assignments and productivity Organizational behavior change: Transactional | Reach: 483 of 517 eligible workers Implementation: Some workers were not present on days when screening occurred. Effectiveness: Over three quarters of those with abnormal or reduced kidney function at mid‑season had kidney functions that improved by the end of the harvest. Those with early indications of kidney function decline received early clinical attention and modification of work duties [45]. Adoption: The company developed a protocol for mid‑harvest screening. Maintenance: Continuous evaluation to ensure protocol is adhered to. |
| TWH Leadership Training (2019–2020) | Health, safety, and well‑being culture survey was distributed to a representative sample of workers across the workforce. Ten TWH leadership trainings were provided across three countries (four sites) of Pantaleon operations, reaching 121 leaders. A study of 1,861 workers showed that field workers with physically demanding jobs and administrative workers both reported more work‑related stress. (Workplace) | Evidence Base: SSWell Study [46, 47] Complexity: Moderate Design: Cross‑sectional Cost: Company contracted with CHWE to collect and analyze health and safety data, create training materials, and deliver trainings. Costs to the company include allocating work time for occupational safety and health staff to help co‑develop the training, allocating work time for leaders to participate in pre‑training interviews and surveys, attending 8‑ hour in‑person training, completing follow‑up surveys. Advantage: Reached leadership at all levels and provided leadership training including feedback from employees and top management Adaptability: Ability to adjust the training to all leadership levels. Training was also adapted to the needs of the company and diverse countries. Trialability: Can be tested in individual work units Organizational behavior change: Transformational | Reach: A total of 120 leaders participated in the Total Worker Health (TWH) training, informed by a Needs Assessment. We surveyed a 20% convenience sample from each department, except Agriculture, where we sampled 297 workers (3% of the 9,744 Agriculture employees), totaling 1,541 surveys [48, 49]. Implementation: Some challenges with follow‑up were identified, which may affect sustainability. Effectiveness: Leaders reported improved leadership practices immediately post‑training, sustained during the 3‑month follow‑up. Health indicators showed reduced stress and improved well‑being. High job demands were linked to poorer health among field and administrative workers, prompting recommendations for adjustments. [48, 49] Adoption: The training was delivered at one timepoint, with a 3‑month follow‑up. Maintenance: Pantaleon continues to focus on the key areas identified in the training and has trained clinical staff through additional national and international programs. Principles taught in these sessions have been incorporated into the formal training received during the employee onboarding process for all new and returning Pantaleon workers. |
[i] *Ethical approvals for these projects were obtained from the Colorado Multiple Institutional Review Board (COMIRB). Informed consent was obtained from study participants for all studies considered as human subjects research. Studies deemed human subjects research also received approval in Guatemala from either the Comite de Etica, Facultad de Medicina, Universidad Francisco Marroquin‑Hospital Universitario Esperanza or ZUGUEME Comité Ética Independiente.