
Figure 1
Characteristics of the sample: Respondents by their gender.
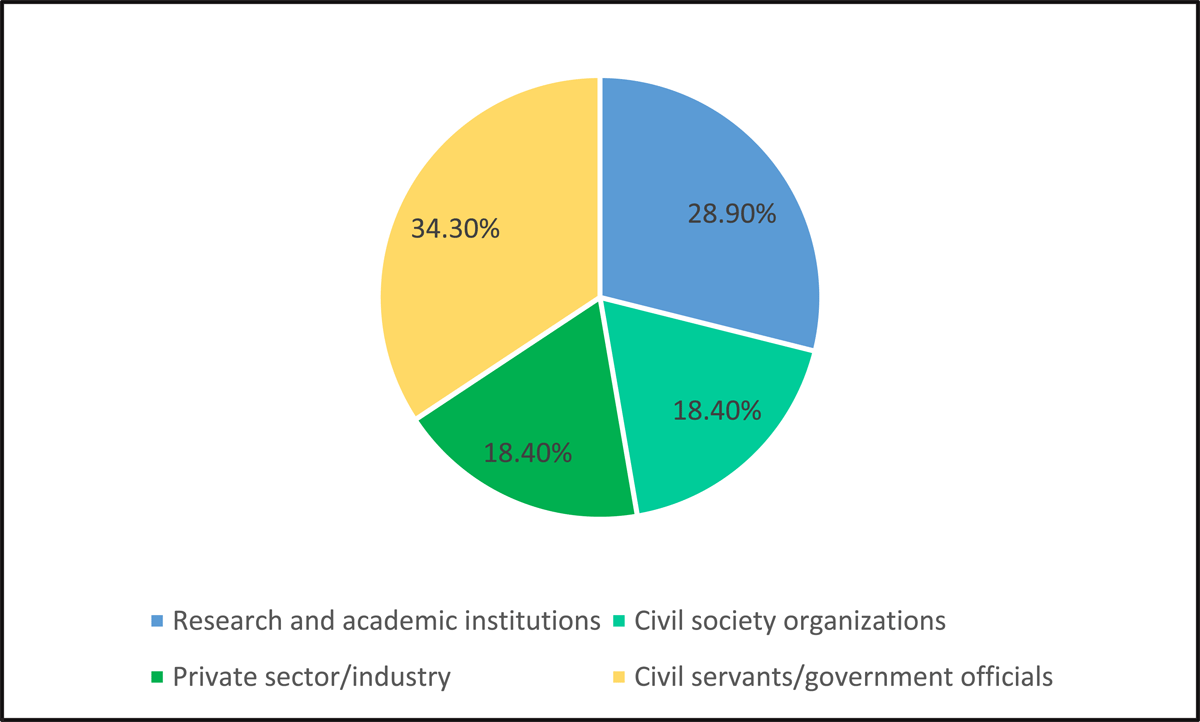
Figure 2
Characteristics of the sample: Respondents by their primary professional affiliations.
Table 1
Interview quotes about policy actors’ conceptualization of UHC.
| SUB-THEMES | INTERVIEW QUOTES (RESPONDENT CODE IN PARENTHESES) |
|---|---|
| 1.1 Quality of care | The goal of universal healthcare would be access to good quality healthcare services. Quality being a very important, what I would call a multiplicative factor not an additive factor. Without quality, you can provide good clinics, but you have to multiply by zero if the quality is not there and therefore you have to assume access is not there. It is like the subcenters that you see of government establishments, there is no quality at all, so they might as well not be there. (ID7, research/academic institution) |
| 1.2 Equity | Equity is the most important thing in universal coverage. As I said, “last mile first.” That is equity… SDGs [Sustainable Development Goals], they call it nobody should be left behind. You know, that is the slogan for this. Ultimately…you have to reach the underprivileged, [they] are the ones who need it the most, and you have to provide services to them. That is the real litmus test for the UHC. (ID27, civil servant/government official) |
| 1.3 Financial risk protection | We can’t have this kind of free for all going on where people are [paying] such high out of pocket [costs] and are being exploited…many of the private players and even public people take money from poor people. We’ve seen how they got in debt…They have spent like two-three lakhs trying to save their family members. You know mortgaging their land and that’s just not acceptable. That’s just a travesty in this day and age. We know what we have to do, we need to do it…the costs should be within [a certain] range, not explode exponentially. (ID4, civil society organization) |
| 1.4 Comprehensive set of services | Universal health coverage firstly is coverage to every Indian, and every resident of the country and it should be comprehensive. Universal suggests both universalities of coverage, that means everybody is included, as well as universal in the sense that it covers all the conditions that are caused by diseases and other medical conditions. (ID26, private sector/industry) |
Table 2
Interview quotes about policy actors’ perception of barriers to UHC.
| SUB-THEMES | INTERVIEW QUOTES (RESPONDENT CODE IN PARENTHESES) |
|---|---|
| 2.1 The lack of a “systems” approach to health reform | We are still trapped in our verticals. Like verticals of TB, verticals of maternal child health… So these all have to be integrated. That kind of discussion has to be routinely happening at the political level, political leadership level in health, as well as administrators, so that is not happening… So alignment has to be there. The second thing is that the integration, so you know, all these verticals coming together to deliver universal health care, so that has to happen. (ID24, civil society organization) |
| 2.2 (a) Barriers related to health financing | It has to also do with financial accountability. How are we getting the most optimal return on our investments?… With whatever money is invested in the health sector, are we getting the best return on that investment? And the answer is no. Because a large amount of public funds are underutilized. I mean they’re sitting there in the state kitties, and they’re not used. So that’s one problem. The money that is used is not necessarily used well. So, therefore, that is another reason that you’re not getting the most optimal results and all of this is because the capacities are low, and accountability is largely absent. (ID29, research/academic institution) |
| 2.2 (b) need for expanded insurance coverage | First, would be the poorest of the poor or the people who just can’t afford any spending on health care. So that would probably be the bottom 40 to 50% population that has been tried to be covered through…the PMJAY scheme [India’s government insurance program] of the government of India. And there’s a top 10 to 15% population of the country that…can spend out of pocket and can very well take care of their healthcare needs. Now comes the missing middle 20 to 30% plus population that remains to be covered… They would require some sort of coverage because as we see these other people from the unorganized sector, they might be workers, they might be earning a wage, they might not come into the category of poor people, but they are not so rich that they can afford the health care expenses on their own and not having any dent on their pockets. (ID33, civil servant/government official) |
| 2.3 (a) Barriers related to the organization of healthcare delivery | There are plenty of instances where basic economic reasoning would need you to think that somethings should be done more with the private sector than by the public sector… So in those cases we should consider privatization. But I think those who vociferously […] oppose privatization also have a point, because the private sector in India has plenty of instances of misbehavior, taking advantage of the consumer, overcharging, over-treating, unsavory collection practices, you know contaminated medication…there’s a long list of things where the private sector is implicated… I don’t find this debate very productive because there’s…[a] similarly long list of things in the public sector where you could find problems. So there’s no point demonizing [a] way of economic organization. (ID5, research/academic institution) |
| 2.3 (b) Hospital-centric design of the health system and bypassing of primary care | Our system is more robust than any other, but we need to take it to the…lower level… So preventive and promotive care, basic NCD care, and along with antenatal care some kind of population-based coverage and screening gives the promotive aspect as well as an understanding of the community… Then linking this nicely and integrating this with the secondary and tertiary care referral mechanisms which we have not succeeded in our country at all. We don’t have gatekeeping everybody goes for [a] cough and cold to the specialist in the government hospital. (ID19, civil servant/government official) |
| 2.3 (c) Need for task shifting | There’s this [human resource] imbalance…how resistant India has been for delegating functions to midwives, for example, when the whole world has acknowledged, the role of midwives…the need for delegating more responsibilities and powers of treatment, diagnosis, and prescription practices from the doctors to other non-medical professions. But only India tightly holds on to the doctor led system… It is not possible to have…30,000 medical colleges and 3,000,000 doctors…it’s not possible. So you have to use a whole lot of a team approach and have more skills and marry the skills available at each level of care with the kind of disease burden that is there, rather than have a prescriptive formula. (ID21, civil servant/government official) |
| 2.4 Regulation, stewardship, and decentralization | I think at the center there is definitely poor political commitment…for some reason, it’s not a winning political issue… People underestimate their likelihood of falling sick and needing health care…or at least serious healthcare, you know, hospital stays, or expensive surgeries… And so the masses apparently don’t reward this as a political issue and that translates into a lack of political will at the center. It’s also expensive and I think…we have to have a serious discussion about the trade-off. If you want to provide health care coverage to anything close to universal, you know, it’s going to be expensive, and obviously, in a country like India there, that means that money that can be used for other things will have to be used for healthcare. (ID22, research/academic institution) |
Table 3
Interview quotes about policy actors’ suggestions for strategies for addressing barriers to UHC.
| SUB-THEMES | INTERVIEW QUOTES (RESPONDENT CODES IN PARENTHESES) |
|---|---|
| 3.1 (a) Strategies for health financing -inefficiencies in resource use | First and foremost is finance. It’s the lack of actual investment… government has borrowed money you know, but for it to actually translate into investments into primary secondary care, and to certain extent tertiary care. It’s a long road ahead…are they being appropriately allocated?…are they being efficient? There’s a lot of wastage and leakage, of course, there’s a lot of wastage, but first we have to invest… This is like two opposite ends of the spectrum. One says, “no, no, you stop the wastage” and [one says,] “no, no, you have to invest more.” So there is that problem. And I am not arguing that there is no wastage or leakage. But we’ve never tried…to say, “let them be self-sufficient.” (ID28, civil servant/government official) |
| 3.1 (b) Strategies for health financing -pooling and catastrophic payments | Every country has very very desperately poor people. They should be offered health care for a small premium by the government. And for people who can afford to pay, there should be different tiers of…health insurance with different premiums. So essentially, hospitals shouldn’t have a cash counter. There has to be a financial intermediary paying for the healthcare and there should be a culture of paying a small amount of money by everyone, every family when they are all well so that when somebody is unwell they don’t need to pay… So essentially all I’m trying to say, in a nutshell, is that every country should concentrate on creating a financial intermediary…but if you say that, “government has to offer health care, it has to be free,” that is a very utopian dream. (ID25, private sector/industry) |
| 3.1 (c) Strategies for health financing – insurance premium collection | They should create a mechanism to collect the premium from the members. Now, when you collect the premium from the members, there is again a mental block… If you…tell them that you have to pay 50 rupees or 100 rupees…every month to this entity. Most people won’t bother. But if you tell them… Okay, you need the electricity connection to your house. Okay, with your electricity bill we are going to charge you extra 100 rupees or 200 rupees, that they don’t mind… Okay, so that is one option. Another one is a mobile phone. Every month they have to pay the mobile bills… Otherwise, the cost of collecting money will be more than the cost of the premium. (ID25, private sector/industry) |
| 3.1 (d) Strategies for health financing – expand insurance | PMJAY [India’s GHI program] provides insurance for…40% of India’s population and not the entire population. Secondly, it is only for secondary and tertiary care. So what is universal health?… PMJAY doesn’t do either. It’s not all citizens, and it is not all [care]… And because it doesn’t cover primary care that whole lack of quality out-of-pocket expenditure is spent… So that’s a large part of the middle-income groups of India are actually not covered by any insurance, because PMJAY will cover your 40% and then the higher levels buy their own private insurance, but there is this huge portion in the middle who actually are not covered at all. (ID29, research/academic institution) |
| 3.1 (e) Strategies for health financing – essential services package | Universal health coverage in India’s context should be…that everyone, rich or poor, in whichever part of the country they live in,…be eligible for certain essential services…you know those which are absolutely life-saving. I don’t think India is in a fiscally in a position to be able to ensure and guarantee that all services under health, complete total health care,… can be provided free of cost…it’s just not possible. And so I think even if India could in the short run, limit itself to say essential health services, and essential can be well defined in accordance with the disease burden and the most common ailments and those which are contributing to disproportionately higher out-of-pocket expenditures…there has to be…fiscal affordability in mind. (ID21, civil servant/government official) |
| 3.1 (f) Strategies for health financing – provider payment mechanisms | At the level of policy and programming, I think we need a conceptual shift from disease-based programming to per capita based or population-based programming. Universal health coverage is about a unit of population, whether it’s a city, a ward, a village district, whatever it might be. And the goal is that you are improving the health of the entire population in an equitable way, rather than basically treating disease one, disease two, disease three. (ID1, research/academic institution) |
| 3.2 (a) Strategies for organization of the healthcare delivery system | It’s a healthy competition. Fifty percent of the market has to be with us in the public sector, 50% “you do what you want”, leave it to the private sector…with the assumption that you cater to the well-off and the rich who can afford you. But at least 50% we provide in the public sector. And these both…also see a strong public sector as essential to have a healthy private sector for keeping the prices under control. So [if] you remove the public sector totally or weaken it,…then you’ll find the private sector becoming extremely predatory and exploitative resorting to irrational care, resorting to unethical conduct, and all the ills of our market, commodifying their product… Only Kerala and Tamil Nadu are trying to find their balance… In any other state, it is either brazenly pro-private…or it is…trying to be strengthening the public sector and not necessarily working with the private sector to come along… It’s not going to be possible for the government to provide all services. It is not possible for us to do away with the private sector, but it is certainly possible for us to come up with appropriate policies to see that the private sector is a responsible partner and not exploitative. (ID21, civil servant/government official) |
| 3.2 (b) Strategies for organization of the healthcare delivery system | I suggested to them “get out of primary care.” You cannot execute it if you don’t have the money. Even the ASHA worker…was able to deliver it to only three and a half per cent of pregnant women. So she might as well not be there… Right so I said to them to focus on the two other things. One is public health. Get your vaccinations done, think about you know social determinants, think about one health, think about that, think about zoonoses, surveillance…education, etc. And then we’ll do secondary. (ID7, research/academic institution) |
| 3.2 (c) Strategies for organization of the healthcare delivery system – human resources for health | It’s these grassroots workers, community-based workers who can make that difference. But they need training, they need supervision, they need motivation and holding, and the systems for them have to be strengthened, because it was formed in 1970… They’ve been umpteen reports, which have said [this], none of those recommendations has been implemented. (ID8, civil society organization) |
| 3.3 (a) Using digital technologies and data systems | There are many applications of digital health. Some of them are very, very useful. For instance, teleconsultation between a medical officer and a specialist is very, very good…so that is fantastic use of digital health… [But] this is not happening. First of all, in the village, you won’t have connectivity… So I think to choose technologies and the use of technology that best serve the interests of the people as well as the system are important. Digital technology as a way of training is really benefit. Right?… But it all has to be linked up. (ID28, civil servant/government official) |
| 3.3 (b) Using digital technologies and data systems – EHR and digital health | I think digital health will play an important role in facilitating universal health coverage. But you know, digital health can’t be a substitute for the provision of services. So you first have to have services available and focus on those and once that happens, in terms of ensuring the quality of services, it’s also making them transparent in terms of ensuring interoperability in terms of ensuring that there is a longitudinal record available, so that both patients and providers have full information about their health records and so that they will [not] repeat unnecessary diagnostics. (ID15, civil servant/government official) |
| 3.3 (c) Using digital technologies and data systems – limitations | I think digital is very good, and frontline workers now they must be trained in its use. They must be given equipment that works well. First, make sure there’s internet connectivity… So to me all the citizen-facing digital things will come slowly to India’s poorer states. So that’s why I’m saying urban areas is where we can do a lot of things […]. It is a very different equation than in a rural areas… So there is disparity and the digital disparity in terms of where you live, if you live in a remote area. (ID28, civil servant/government official) |
| 3.4 (a) Improving regulation and decentralization | So what happens is actually a vicious circle, that if you don’t have the capacity, you can’t utilize it. And you don’t apply this capacity. Also, there is an issue of lack of flexibility, because if you are giving funds to states which are divided into say 900 subjects and you don’t have the flexibility of shifting money from one subject to another subject. So that of course is a recipe for non-utilization because by definition, in some of the surveys, you will not be able to use money. Therefore, giving more flexible, strengthening capacity, strengthening the capacity to absorb resources, together with some accountability and monitoring mechanism. (ID15, civil servant/government official) |
| 3.4 (b) Improving regulation and decentralization – role of central leadership | The center [needs] to take…on…the role of ensuring that there are regulatory structures again…they will be you know regulatory standards and so on which are centralized mechanisms which are there, and yet [they] allow the flexibility on state levels, depending on the level of development that’s happened in the state itself… But they could lay out some basic principles and mechanisms that must be instituted. It [has] shown enough capacity to take strong-arm action when it wants to, certainly therefore [this is] an area where it should show that. (ID34, civil society organization) |