
Figure 1.
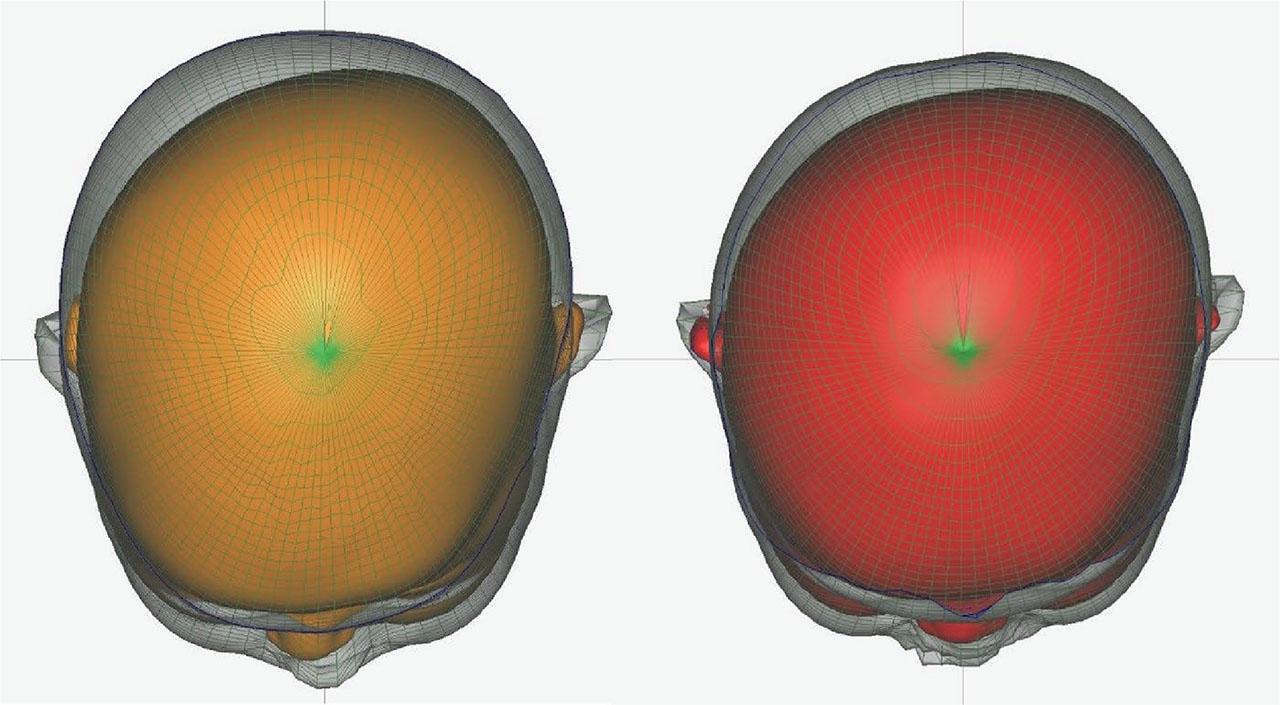
Figure 2.
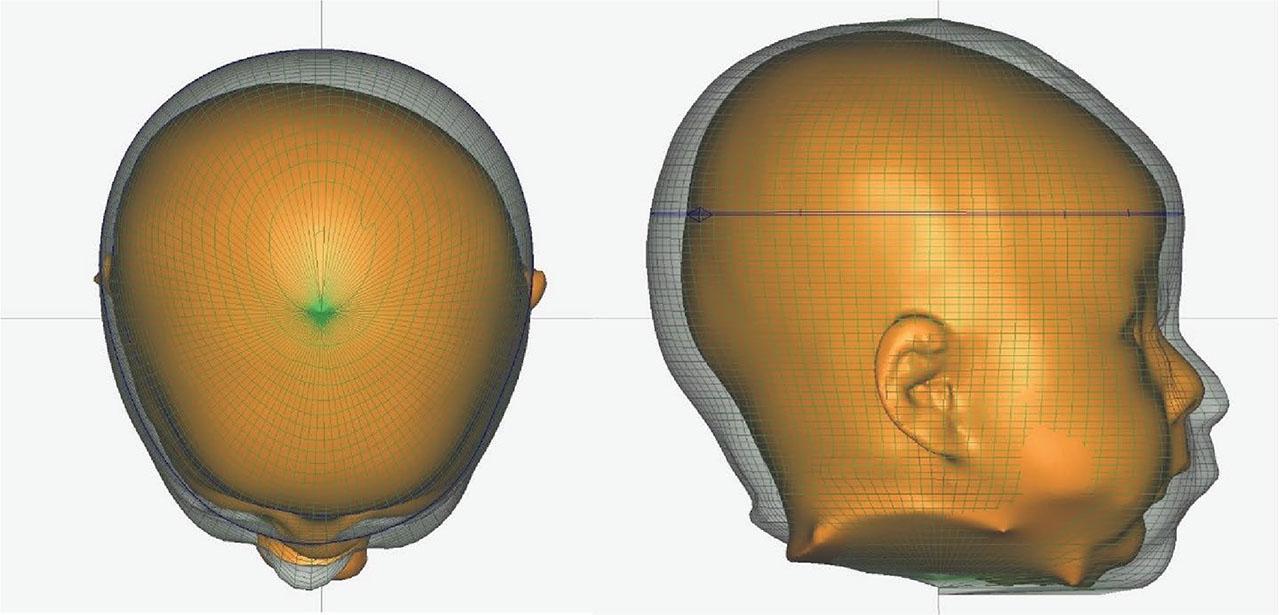
Figure 3.
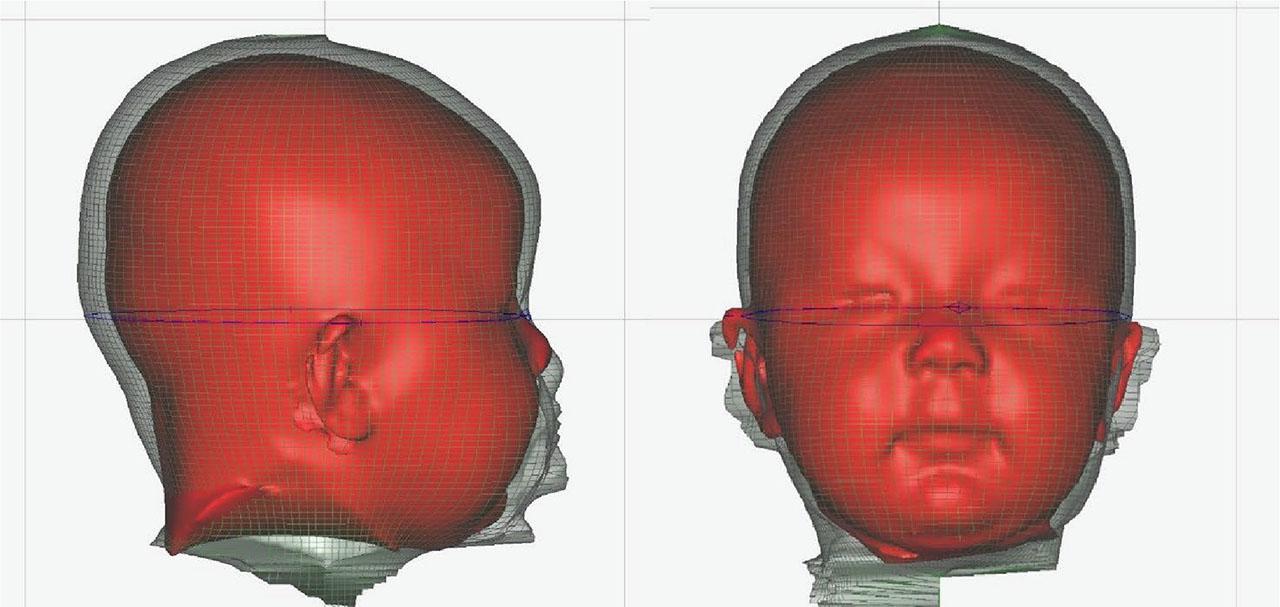
Figure 4.
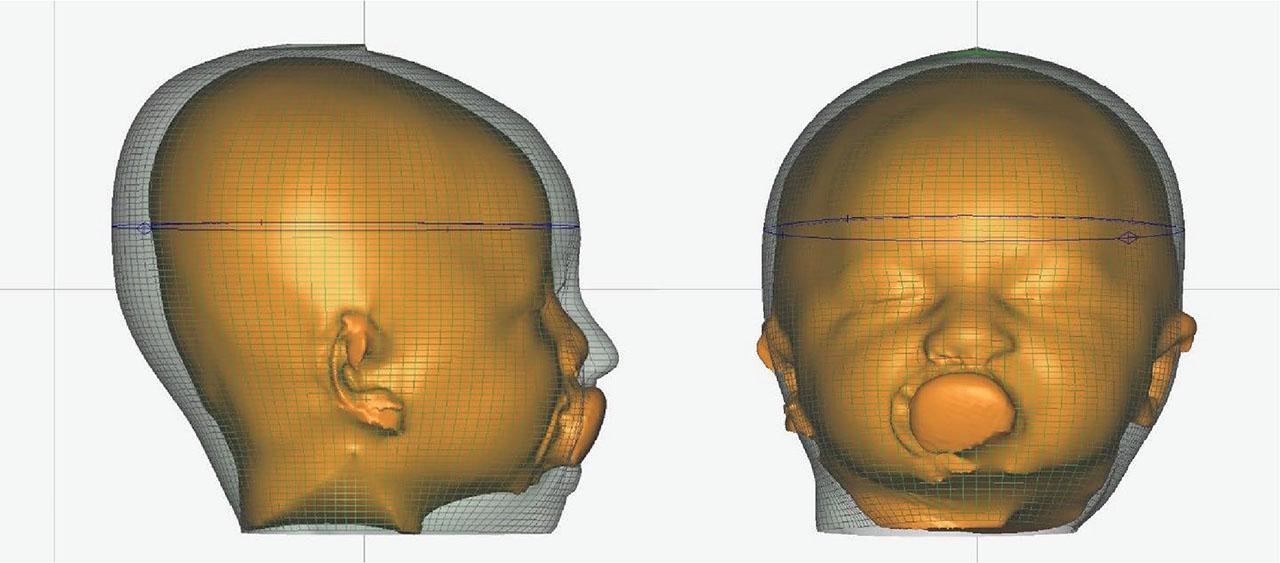
Figure 5.

Figure 6.

Figure 7.

Figure 8.

Figure 9.

Figure 10.

Figure 11.

Initial measurements of skull parameters (average values)
| Area | Value |
|---|---|
| Anterior-posterior skull size (AP), mm | 129 |
| Lateral, mm | 123 |
| Right anterior size (RA), mm | 136 |
| Left anterior size (LA), mm | 127 |
| Circumference, cm | 41.5 |
Final measurements of skull parameters (average values)
| Area | Value |
|---|---|
| AP, mm | 142 |
| Side, mm | 129 |
| RA, mm | 139 |
| LA, mm | 136 |
| Circumference, cm | 43.5 |
Parents’ responses regarding the comfort and effectiveness of corrective helmets
| Question 1: How easily did your child adapt to wearing a helmet, and did you have any difficulties caring for them? | |
| Very easy, there were no difficulties | 21 people |
| It took some time to adapt, but there were no problems | 7 people |
| The adaptation was difficult, but we managed | 2 people |
| There were many difficulties, the child never got used to it | 0 people |
| Question 2: Do you feel an improvement in the shape of your child’s head from the very beginning of using the helmet? | |
| Noticeable improvement, the shape of the head has become more symmetrical | 18 people |
| Moderate improvement, positive changes are observed | 10 people |
| Minor improvement, but still hard to notice the result | 2 people |
| No improvements are noticeable, and the shape of the head has hardly changed | 0 people |
| Question 3: How comfortable is it for a child to wear a helmet in everyday life (considering sleep time, eating, and activity)? | |
| Very comfortable, the helmet does not interfere with the child | 15 people |
| Quite comfortable, but sometimes there is discomfort | 12 people |
| It is not always comfortable, but the child gets used to it | 3 people |
| The child is uncomfortable, the helmet interferes with everyday life | 0 people |
Modern methods for diagnosing cranial deformities
| Method name | Characteristics |
|---|---|
| 3D computed tomography with low radiation dose | Provides high-quality three-dimensional images of the skull with minimal radiation exposure. Allows assessing bone structures in detail and planning surgical intervention for complex deformities. |
| EOS-imaging | Innovative system for obtaining two- and three-dimensional images in an upright position of the patient using ultra-low radiation doses. Allows simultaneously assessing deformities of the skull and spine |
| Functional magnetic resonance imaging | Displays brain activity in real time, helping to assess the impact of skull deformities on functional areas of the brain. Useful for treatment planning that preserves important neural pathways. |
| Diffusion tensor imaging | Specialised type of magnetic resonance imaging (MRI) that visualises the pathways of the brain’s white matter. Helps to identify possible violations of neuronal connections due to deformities of the skull. |
| Three-dimensional ultrasound examination | Non-invasive radiation-free method that creates a 3D image of the skull. Ideal for diagnosis in infants and young children with soft bones. |
| Optical 3D scanning | Uses light technologies to create high-precision three-dimensional models of the skull surface. Fast and safe method for evaluating external deformations. |
| Virtual surgical planning and 3D printing | Uses light technologies to create high-precision three-dimensional models of the skull surface. Fast and safe method for evaluating external deformations. |
| Stereophotogrammetry | Technology for obtaining three-dimensional images using photos from different angles. Allows non-contact assessment of the shape and symmetry of the skull. |
| Ultrasonic holography | New method that uses ultrasound waves to create holographic images of the internal structures of the skull. Provides a safe alternative to X-rays for diagnosis. |
| 4D visualisation | Combines three-dimensional images with time measurement, helping to observe dynamic changes in the skull during movement or growth. It is useful for studying the functional aspects of deformations. |
Questionnaire text
| No. | Question | Answers |
|---|---|---|
| 1. | How easily did your child adapt to wearing a helmet, and did you have any difficulties caring for them? | Very easy, there were no difficulties |
| It took some time to adapt, but there were no problems | ||
| The adaptation was difficult, but we managed | ||
| There were many difficulties, the child never got used to it | ||
| 2. | Do you feel an improvement in the shape of your child’s head from the very beginning of using the helmet? | Noticeable improvement, the shape of the head has become more symmetrical |
| Moderate improvement, positive changes are observed | ||
| Minor improvement, but still hard to notice the result | ||
| No improvements are noticeable, and the shape of the head has hardly changed | ||
| 3. | How comfortable is it for a child to wear a helmet in everyday life (considering sleep time, eating, and activity)? | Very comfortable, the helmet does not interfere with the child |
| Quite comfortable, but sometimes there is discomfort | ||
| It is not always comfortable, but the child gets used to it | ||
| The child is uncomfortable, the helmet interferes with everyday life |
Methods of treatment of cranial deformities and their characteristics
| Method of non-surgical treatment of skull deformity | Characteristics |
|---|---|
| Corrective helmet | The use of specially made helmets that gradually correct the shape of the infant’s skull. It is effective in the treatment of positional plagiocephaly, brachycephaly, and scoliocephaly. The method consists of directing the growth of the skull bones by lightly pressing on the protruding areas and creating space in the flattened regions to allow natural symmetrical growth. |
| Positional therapy | A non-constructive intervention that involves changing the position of the child’s head during sleep and activity to reduce pressure on flattened areas. It is effective for mild forms of positional plagiocephaly. It includes recommendations for lying on the stomach under supervision, changing the position of the crib, and stimulating head turns. |
| Physical therapy | Using 3D printing technology to create individual orthopaedic devices that correct the shape of the skull. Provides precise compliance with the patient’s anatomy and comfort in use. It is effective for various types of deformities, in particular, plagiocephaly and brachycephaly. |
| Dynamic helmet (orthosis) therapy | The use of dynamic orthoses that adapt to the child’s growth and provide a constant corrective effect. It is effective in the treatment of asymmetric deformities. The method allows controlling the correction process and reduces the need for frequent replacement of orthoses. |
| Non-invasive laser therapy | The use of low-intensity laser radiation to stimulate cellular metabolism and improve blood circulation in areas of deformity. It can help to accelerate the natural correction of the shape of the skull in case of mild deformities. |
| Kinesiotaping | Application of special elastic tapes to the scalp and neck to correct muscle tone and head position. It is used as an auxiliary method for mild deformities or in combination with physical therapy. Helps to improve the symmetry of movements and head position. |
| Electrical muscle stimulation | The use of electrical impulses to stimulate the muscles of the neck and shoulder girdle to correct positional deformities. It is useful for muscle weakness or an imbalance that leads to skull asymmetry. It is carried out under the supervision of a specialist in physical rehabilitation. |
| Biofeedback therapy | The use of biofeedback technologies to train the patient to control muscle activity. Helps in correcting the position of the head and neck, is effective for functional deformities. The method is non-invasive and safe, suitable for older children. |