
Figure 1.
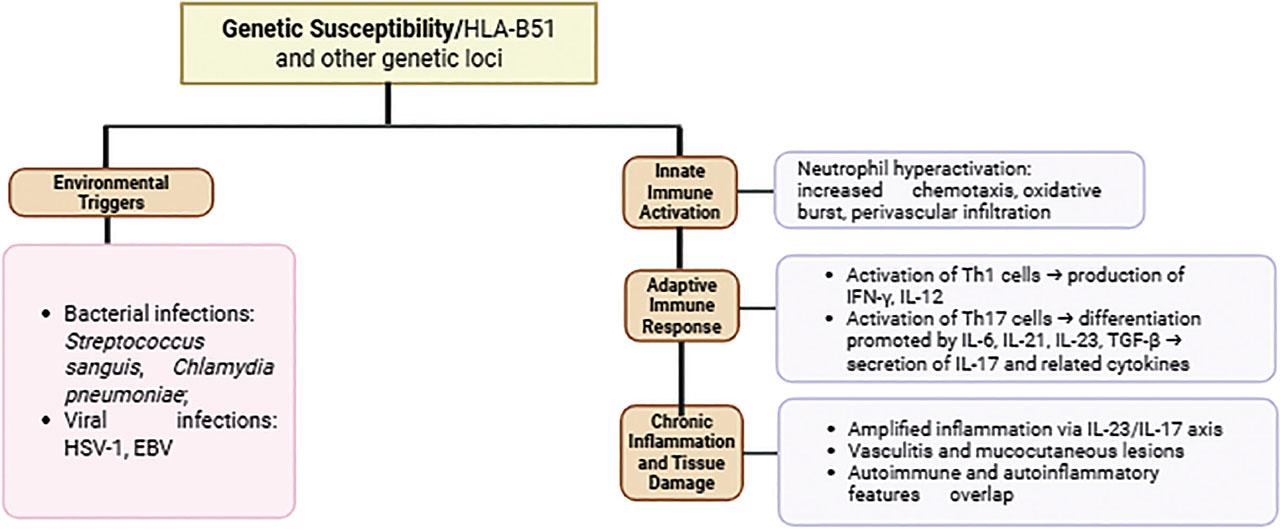
Figure 2.
Genetic Variants of HLA-B*51 and Their Clinical Implications in Behçet’s Disease_
| Gene | Mutation/variant | Associated role in BD | Clinical implications | Reference |
|---|---|---|---|---|
| HLA-B*51 | Polymorphic amino acid residues (e.g., Asp at position 63, Phe at position 67) | Primary genetic risk factor for BD worldwide | Strong association with genital ulcers, ocular involvement, and skin manifestations; lower gastrointestinal involvement | [20] |
| HLA-B*51:01 | Subtype of HLA-B*51 | Most common subtype associated with Behcet’s syndrome | Linked to ocular involvement and other inflammatory symptoms | [28] |
| HLA-B*51:08 | Subtype of HLA-B*51 | Common subtype associated with Behcet’s syndrome | Also associated with ocular involvement | [28] |
| ERAP1(Hap10) | Epistatic interaction with HLA-B*51 | Modifies the peptide repertoire presented by HLA-B*51, influencing immune response | Associated with altered trimming activity of MHC-Class I peptides, potentially contributing to pathogenesis | [20] |
Treatment Approaches for Behçet’s Disease by Manifestation_
| Manifestation | First-line treatments | Second-line treatments | Experimental treatments |
|---|---|---|---|
| Mucocutaneous |
|
|
|
| Articular |
|
| Tocilizumab |
| Ocular |
|
| |
| Vascular |
|
| Tocilizumab |
| Gastrointestinal | 5-Aminosalicylic acid derivatives | Glucocorticoids | Not extensively studied |
Circulating MicroRNA Profiles Associated with Behçet’s Disease: Potential Biomarkers and Their Roles_
| miRNA | Description | Reference |
|---|---|---|
| Hsa-miR-224-5p | Found to be significantly deregulated in patients with BS; this can potentially be used to discriminate BD from healthy controls and other diseases. | [29] |
| Hsa-miR-206 | Part of the unique circulating miRNA profile associated with BD, indicating its role in the disease’s pathophysiology. | [41] |
| Hsa-miR-653-5p | Another miRNA identified in the circulating profile that may serve as a biomarker for BS diagnosis and disease activity. | [41] |
| miR-21 | Associated with inflammation in BS; higher expression levels may correlate with disease activity and pathogenesis. | [43] |
| miR-155 | Increased expression may indicate disease remission, and could be useful for monitoring BS progression. | [44] |
| Hsa-miR-143-3p | Identified as part of miRNA expression profiling associated with active disease states in BS. | [42] |
| Hsa-miR-199a-5p | Targeting pathways relevant to BS, this miRNA is part of the signature associated with the disease’s inflammatory response. | [42] |
Genetic Mutations Associated with Behçet’s Disease and Their Clinical Features_
| Gene | Mutation | Associated condition | Frequency in Behcet’s Diseases Patients | Clinical features |
|---|---|---|---|---|
| MVK | V377I/V377I | Mevalonate kinase deficiency (MKD) | Found in two patients (2.06%) | Fever, chills, bipolar aphthosis, erythema nodosum, serve acne, transient arthraglia |
| MVK | V377I/S135L | Mevalonate kinase deficiency (MKD) | Found in one patient (1.03%) | Similar to above, with additional features like conjunctivitis and abdominal pain |
| MVK | V377I/- | Mevalonate kinase deficiency (MKD) | Found in one patient (1.03%) | Bipolar aphthosis, erythema nodosum, folliculitis, uveitis |
| CIAS1 | V198M | Cryopyrin-associated periodic syndromes (CAPS) | Found in one patient (1.03%) | Buccal and skin aphthosis, erythema nodosum, uveitis |
Male:Female ratio and age of onset [11, 12]_
| Region | Male: Female Ratio | Typical Age of Onset |
|---|---|---|
| Middle East | 3.4–5.3:1 (M>F) | 20–40 years (mean 25–30) |
| Europe, Japan | F>M or near equal | 20–40 years |
| United States | 1:5 (F>M) | 20–40 years |
Prevalence of BD by Country_
| Country | Prevalence (case per 100,000 inhabitants) | Reference |
|---|---|---|
| Turkey | 420 | [20] |
| Japan | 7.0 – 14.6 | [20] |
| Korea | 32.8 – 35.7 | [21] |
| China | 13.5 – 20 | [22] |
| Mongolia | 2.4 | [23] |
| Kazakhstan | 10 – 15 | [23] |
| Iran | 16.7 – 80.0 | [20] |
| Saudi Arabia | 19.5 | [20] |
| Israel | 15.2 | [24] |
| Egypt | 3.6 | [8] |
| USA | 5.2 | (24] |
| Brazil | 0.3 | (25] |
| Colombia | 1.10 – 2.2 | [25, 26] |
| Italy | 3.8 | [20] |
| Spain | 5.6 – 7.5 | [20] |
| Portugal | 1.5 – 2.4 | [23] |
| United Kingdom | 14.6 | [23] |
| Wales | 11.1 | [23] |
| France | 7.1 | [24] |
| Germany | 0.6 – 1.47 | [20] |
| Switzerland | 4.03 | [27] |
This table highlights recent advances in targeted therapies for Behçet’s disease, reflecting a shift toward biologics and small molecules that modulate specific immune pathways_
| Therapy | Study Type & Population | Efficacy Outcomes | Safety/Side Effects | Reference |
|---|---|---|---|---|
| Infliximab | Randomized, controlled head-to-head trial vs. IFN-α in refractory BD patients | Comparable improvement in Behçet’s Disease Activity Index (BDAI) at 12 and 24 weeks; steroid-sparing effect, with 20% stopping steroids | Generally well-tolerated; trend toward better persistence and tolerability vs. IFN-α | BIO-BEHÇET’s trial [32] |
| Interferon-α2a | Same as above | Similar clinical efficacy to infliximab; 44% steroid cessation rate | Side effects common but manageable; slightly less tolerable than infliximab | BIO-BEHÇET’S trial [32] |
| Apremilast | Phase 3 paediatric oral ulcers associated with BD | Significant reduction in oral ulcer frequency and severity compared to placebo | Generally mild side effects; good safety profile in children | Ongoing Phase 3 trials[23, 33] |
| Filgotinib (JAK inhibitor) | Multi-centre, open-label Phase 2 trial in BD and other IMIDs | Preliminary efficacy data expected; targets JAK-STAT pathway implicated in BD inflammation | Safety data pending; JAK inhibitors have known risks, including infections and lab abnormalities | DRIMID study protocol [34] |
| Lenalidomide | Clinical trial in refractory mucosal BD ulcers | Evaluating efficacy and safety; lenalidomide’s immunomodulatory effects may reduce ulcer severity | Safety profile under investigation; known risks include cytopenias and thromboembolism | ClinicalTrials.gov NCT05449548 |
| RAY121 (complement inhibitor) | Phase 1b basket trial including BD patients | Assessing safety, tolerability, and preliminary efficacy targeting classical complement pathway | Early phase; safety profile and efficacy data pending | ClinicalTrials.gov NCT06371417 |
| Adalimumab vs Tocilizumab | Multi-centre, randomized trial in severe BD uveitis | Comparing efficacy and safety in ocular involvement; results pending | Safety profiles differ; anti-TNF and anti-IL-6R agents have distinct side effect spectra | ClinicalTrials.gov NCT05874505 [35],[36] |
Comparison of ISG and ICBD Diagnostic Criteria for Behçet’s Disease: Sensitivity, Specificity, and Key Limitations_
| Criteria | Sensitivity | Specificity | Key limitations |
|---|---|---|---|
| ISG | 66–85% | 95–98% | Excludes major organ involvement; low pathergy positivity [37, 38]. |
| ICBD | 94–98% | 73–97% | Risk of overdiagnosis; lower specificity [37,38,39] |
| The ICBD demonstrates superior accuracy (97% vs. 85% for ISG) and better accommodates early or atypical cases. However, the ISG remains widely used for its high specificity in excluding mimics. | |||