
Antibiotic-resistant bacterial infections are a global public health threat, especially those caused by Gram-negative bacteria (Cheong et al. 2022; 2023). Carbapenem-resistant (CR) Acinetobacter baumannii, multidrug-resistant (MDR) Pseudomonas aeruginosa, CR Klebsiella pneumonia, and CR Escherichia coli present significant challenges worldwide (Tamma et al. 2023).
The opportunistic pathogen P. aeruginosa can cause severe infections in immunocompromised patients (Marashi et al. 2022). The primary mechanisms of imipenem resistance in P. aeruginosa involve alteration of porin channels and acquired carbapenemases, which are broad-spectrum β-lactamases capable of hydrolyzing carbapenems. Sometimes, reduced susceptibility or resistance to carbapenems results from the overexpression of operons encoding efflux pump systems. Low levels of chromosomal ampC β-lactamase generally do not hydrolyze carbapenems; however, overexpression of ampC can raise carbapenem MICs when it occurs in combination with reduced porin permeability or enhanced efflux pump activity (Santajit and Indrawattana 2016; Hammoudi Halat and Ayoub Moubareck 2022). Carbapenem resistance in P. aeruginosa is also mediated by various β-lactamases. These enzymes are grouped into two main categories. Serine carbapenemases correspond to Ambler classes A and D. Class A includes Guiana extended-spectrum (GES)-type β-lactamases such as GES-2 and GES-5, and some P. aeruginosa strains produce K. pneumoniae carbapenemases (KPC). Class D comprises oxacillin-hydrolyzing β-lactamase (OXA)-type carbapenemases. Intrinsic OXA-50 and its variants are highly prevalent but possess limited carbapenemase activity; by contrast, acquired OXA-2 and OXA-10 family enzymes are frequently detected and are clinically relevant for carbapenem resistance in P. aeruginosa (Mack et al. 2025). Metallo-β-lactamases are Ambler class B enzymes. They are represented mainly by the imipenem metallo-β-lactamase (IMP), Verona-integron-encoded metallo-β-lactamase (VIM), Sao Paulo metallo-β-lactamase (SPM), and German imipenemase (GIM) families. In addition, P. aeruginosa isolates producing New Delhi metallo-β-lactamase (NDM)-1 were first reported in 2011 (Potron et al. 2015; Hammoudi Halat and Ayoub Moubareck 2022). The prevalence of VIM-, IMP-, and NDM-type carbapenemases in P. aeruginosa has increased significantly worldwide over the past two decades (Mack et al. 2025).
Ceftazidime-avibactam is formulated as a combination of a third-generation cephalosporin and a recently developed non-β-lactam β-lactamase inhibitor, with a fixed ceftazidime-to-avibactam ratio of 4:1 (Daikos et al. 2021; Lee and Lee 2022). It is active against ESBL-, ampC-, KPC-, and OXA-48–producing Enterobacterales and MDR P. aeruginosa, but inactive against most Acinetobacter spp. and metallo-β-lactamase-producing isolates (Pogue et al. 2019).
In Korea, the recent introduction of ceftazidime-avibactam is a noteworthy development. However, data on its in vitro activity against P. aeruginosa in community hospitals prior to its clinical use remain limited. This study aimed to evaluate the antimicrobial resistance profiles of P. aeruginosa isolates collected in 2017–2018 from clinical specimens in a community-based hospital and to assess their in vitro susceptibility to ceftazidime-avibactam and other agents.
A total of 100 consecutive P. aeruginosa isolates were obtained from 100 patients at a community-based hospital in South Korea from October 2017 to March 2018. Isolates came from routine diagnostic samples of both outpatients and inpatients. Only the first positive culture per patient was included in the analysis. Surveillance cultures were not performed during the study period. Demographic and clinical data for the patients were obtained by retrospective chart review. This study was approved by the Institutional Review Board of Uijeongbu St. Mary’s Hospital (no. UC22RISI0108), and informed consent was waived due to the study’s retrospective design.
The minimum inhibitory concentrations (MICs) of ceftazidime, ceftazidime-avibactam, and colistin were determined for each isolate by the broth microdilution method. The bacteria were inoculated on Mueller–Hinton agar at a concentration of 0.5 McFarland standard. After incubation at 35 ± 2°C for 16–20 hours under aerobic conditions, susceptibilities were interpreted according to the 2018 CLSI guidelines. To assess the effects of ceftazidime-avibactam, the strains were incubated with increasing concentrations of ceftazidime in combination with a fixed concentration (4 mg/l) of avibactam (PF-06416494-02, Pfizer Inc., USA).
Six P. aeruginosa strains producing carbapenemases (one IMP-1, one IMP-6, and four VIM-2) were kindly provided by the Korea Disease Control and Prevention Agency (Korea) and were used as reference strains for antimicrobial susceptibility testing. The P. aeruginosa ATCC® 27853™ strain was used as a control strain in antimicrobial susceptibility testing.
Susceptibility to amikacin, aztreonam, cefepime, ciprofloxacin, gentamicin, imipenem, meropenem, and piperacillin/tazobactam was evaluated using the MicroScan system (Beckman Coulter, Inc., USA) according to the CLSI guidelines.
To identify β-lactamase genes, a modified multiplex polymerase chain reaction (PCR) for the detection of carbapenemase genes was performed as previously described (Poirel et al. 2011; Christophy et al. 2017). The presence of blaIMP, blaVIM, blaNDM-1, blaGES, blaSIM, blaKPC, and blaOXA-48 was investigated in MDR P. aeruginosa strains. A total of 27 CR P. aeruginosa isolates were subjected to PCR analysis.
An MDR P. aeruginosa strain was defined as non-susceptible to ≥ 1 agent in ≥ 3 antimicrobial categories, including penicillin combinations (piperacillin-tazobactam), cephalosporins (ceftazidime or cefepime), carbapenems (imipenem-cilastatin or meropenem), monobactams (aztreonam), aminoglycosides (amikacin or gentamicin), quinolones (levofloxacin or ciprofloxacin), and polymyxins (colistin) (Magiorakos et al. 2012). Difficult-to-treat (DTR) P. aeruginosa was defined as resistant or intermediately susceptible to all of the following antimicrobial agents: piperacillin-tazobactam, ceftazidime, cefepime, aztreonam, meropenem, imipenem-cilastatin, ciprofloxacin, and levofloxacin (Kadri et al. 2018). A P. aeruginosa strain was considered CR if it was not susceptible to meropenem or imipenem-cilastatin (Lee et al. 2022). ‘Intermediate’ and ‘resistant’ results were categorized as non-susceptible.
All antibiotic susceptibility results were determined based on the 2018 CLSI recommendations.
The data were expressed as a number (percentage) for categorical variables. Results were compared using a t-test for continuous variables and a chi-square test for categorical variables. All statistical analyses were performed using IBM® SPSS® Statistics for Windows, version 18 (IBM Corporation, USA), with statistical significance defined as a twotailed p-value < 0.05.
Between October 2017 and March 2018, 100 P. aeruginosa isolates were obtained from 100 patients at a community-based hospital in Korea. Of these, 37 were MDR, 27 were CR, and 9 were DTR. Table I presents the clinical characteristics of the patients with P. aeruginosa infections. Respiratory specimens were the predominant source (53%), followed by genitourinary specimens (25%). There were no statistically significant differences in the proportion of MDR P. aeruginosa strains between respiratory and non-respiratory samples (41.5% vs. 31.9%, p = 0.433).
Culture source and clinical characteristics of patients infected with multidrug-resistant and non-multidrug-resistant Pseudomonas aeruginosa.
| Demographic parameter | No. of isolates (%) | p-value | |
|---|---|---|---|
| Non-multidrug-resistant P. aeruginosa (n = 63) | Multidrug-resistant P. aeruginosa* (n = 37) | ||
| Male gender | 44 (69.8) | 27 (73.0) | 0.916 |
| Age groups (years) | 0.291 | ||
| < 18 | 7 (11.1) | 1 (2.7) | |
| 18–64 | 23 (36.5) | 13 (35.1) | |
| ≥ 65 | 33 (52.4) | 23 (62.2) | |
| ICU admission | 9 (14.3) | 8 (21.6) | 0.505 |
| Surgical department† | 25 (39.7) | 13 (35.1) | 0.811 |
| Clinical specimen | 1.000 | ||
| Respiratory | 31 (49.2) | 22 (59.5) | |
| Genitourinary | 16 (25.3) | 9 (24.3) | |
| Skin and soft tissue | 10 (15.9) | 6 (16.2) | |
| Gastrointestinal | 3 (4.8) | 0 (0) | |
| Blood | 1 (1.6) | 0 (0) | |
| Bone and joint | 2 (3.2) | 0 (0) | |
| Treatment characteristic | |||
| ≥ 1 active agentx‡ | 45 (71.4) | 21 (56.8) | 0.202 |
| Use of carbapenem | 11 (17.5) | 18 (48.6) | 0.002 |
| Use of colistin | 3 (4.8) | 10 (27.0) | 0.004 |
| Clinical success | 54 (85.7) | 24 (64.9) | 0.029 |
| Death attributable to P. aeruginosa | 6 (9.5) | 10 (27.0) | 0.043 |
Multidrug-resistant P. aeruginosa was defined as non-susceptible to ≥ 1 agent in ≥ 3 antimicrobial categories, which included penicillin combinations (piperacillin-tazobactam), cephalosporins (ceftazidime or cefepime), carbapenems (imipenem or meropenem), monobactams (aztreonam), aminoglycosides (amikacin or gentamicin), quinolones (levofloxacin or ciprofloxacin), and polymyxins (colistin).
The department of surgery includes orthopedic surgery, neurosurgery, thoracic surgery, trauma surgery, general surgery, plastic surgery, urology and otolaryngology.
Active agents were defined by in vitro susceptibility according to CLSI interpretive criteria.
Appropriate antibiotic use was observed in 71.4% of patients with non-MDR P. aeruginosa infections and 56.8% of those with MDR P. aeruginosa infections. Carbapenems and colistin were used significantly more frequently in the MDR group. Specifically, appropriate use of carbapenems was 100% in the non-MDR group and 38.9% in the MDR group (p = 0.001), while appropriate use of colistin was 100% in the non-MDR group and 90% in the MDR group (p = 1.000). Clinical success was more commonly achieved in the non-MDR group compared to the MDR group (85.7% vs. 64.9%, p = 0.029), and in-hospital death was less frequent (33.3% vs. 54.1%, p = 0.068) in the non-MDR group. Deaths attributable to P. aeruginosa infection were significantly more frequent in the MDR group than in the non-MDR group (9.5% vs. 27%, p = 0.043).
Tables II and III present the MICs and the percentage of P. aeruginosa isolates classified as susceptible or resistant to the antimicrobial agents. Overall, ceftazidime-avibactam was the most active antibiotic (MIC50/90 = 4/8 mg/l, 95% susceptible), followed by amikacin (93% susceptible) and colistin (91% susceptible). Ciprofloxacin exhibited the lowest activity (MIC50/90 = ≤ 0.25/≥ 4 mg/l, 68% susceptible).
In vitro antimicrobial activity against Pseudomonas aeruginosa isolates including total and multidrug-resistant strains.
| Organism/antimicrobial | MIC50 (mg/l) | MIC90 (mg/l) | MIC range (mg/l) | % S |
|---|---|---|---|---|
| P. aeruginosa (n = 100) | ||||
| Amikacin | ≤ 2 | 16 | ≤ 2 to ≥ 64 | 93 |
| Gentamicin | ≤ 1 | 8 | ≤ 1 to ≥ 16 | 87 |
| Aztreonam | 8 | ≥ 64 | ≤ 1 to ≥ 64 | 82 |
| Ciprofloxacin | ≤ 0.25 | ≥ 4 | ≤ 0.25 to ≥ 4 | 68 |
| Ceftazidime-avibactam | 4 | 8 | ≤ 1 to ≥ 128 | 95 |
| Ceftazidime | 4 | 32 | ≤ 1 to ≥ 128 | 76 |
| Cefepime | 2 | 32 | ≤ 1 to ≥ 64 | 82 |
| Imipenem | 2 | ≥ 16 | ≤ 0.25 to ≥ 16 | 76 |
| Meropenem | 0.5 | ≥ 16 | ≤ 0.25 to ≥ 16 | 75 |
| Piperacillin-tazobactam | 8 | ≥ 128 | ≤ 4 to ≥ 128 | 72 |
| Colistin | 1 | 2 | ≤ 0.5 to ≥ 128 | 91 |
| MDR P. aeruginosa (n = 37) | ||||
| Amikacin | 4 | ≥ 64 | ≤ 2 to ≥ 64 | 81.1 |
| Gentamicin | 4 | ≥ 16 | < 1 to ≥ 16 | 37.6 |
| Aztreonam | 16 | ≥ 64 | ≤ 1 to ≥ 64 | 21.6 |
| Ciprofloxacin | ≥ 4 | ≥ 4 | ≤ 0.25 to ≥ 4 | 24.3 |
| Ceftazidime-avibactam | 4 | 16 | ≤ 1 to ≥ 128 | 86.5 |
| Ceftazidime | 16 | 128 | 2 to ≥ 128 | 45.9 |
| Cefepime | 8 | ≥ 64 | ≤ 1 to ≥ 64 | 51.4 |
| Imipenem | ≥ 16 | ≥ 16 | 1 to ≥ 16 | 43.2 |
| Meropenem | 8 | ≥ 16 | ≤ 0.25 to ≥ 16 | 37.8 |
| Piperacillin-tazobactam | 64 | ≥ 128 | ≤ 4 to ≥ 128 | 27.0 |
| Colistin | 1 | 4 | ≤ 0.5 to ≥ 128 | 89.2 |
MDR - multidrug-resistant
In vitro antimicrobial activity against Pseudomonas aeruginosa isolates including carbapenem-resistant and difficult-to-treat strains.
| Organism/antimicrobial | MIC50 (mg/l) | MIC90 (mg/l) | MIC range (mg/l) | % S |
|---|---|---|---|---|
| CR P. aeruginosa (n = 27) | ||||
| Amikacin | 4 | ≥ 64 | ≤ 2 to ≥ 64 | 74.1 |
| Gentamicin | 2 | ≥ 16 | ≤ 1 to ≥ 16 | 66.7 |
| Aztreonam | 16 | ≥ 64 | ≤ 1 to ≥ 64 | 25.9 |
| Ciprofloxacin | ≥ 4 | ≥ 4 | ≤ 0.25 to ≥ 4 | 29.6 |
| Ceftazidime-avibactam | 4 | 16 | ≤ 1 to ≥ 128 | 85.2 |
| Ceftazidime | 8 | 64 | 2 to ≥ 128 | 51.9 |
| Cefepime | 8 | ≥ 64 | ≤ 1 to ≥ 64 | 51.9 |
| Imipenem | ≥ 16 | ≥ 16 | 2 to ≥ 16 | 11.1 |
| Meropenem | ≥ 16 | ≥ 16 | 0.5 to ≥ 16 | 7.4 |
| Piperacillin-tazobactam | 32 | ≥ 128 | ≤ 4 to ≥ 128 | 44.4 |
| Colistin | 1 | 4 | ≤ 0.5 to ≥ 128 | 88.9 |
| DTR P. aeruginosa (n = 9) | ||||
| Amikacin | ≥ 64 | ≥ 64 | ≤ 2 to ≥ 64 | 33.3 |
| Gentamicin | ≥ 16 | ≥ 16 | 2 to ≥ 16 | 33.3 |
| Aztreonam | 32 | ≥ 64 | 16 to ≥ 64 | 0 |
| Ciprofloxacin | ≥ 4 | ≥ 4 | ≥ 4 to ≥ 4 | 0 |
| Ceftazidime-avibactam | 4 | ≥ 128 | ≤ 1 to ≥ 128 | 66.7 |
| Ceftazidime | 64 | ≥ 128 | 16 to ≥ 128 | 0 |
| Cefepime | 32 | ≥ 64 | 16 to ≥ 64 | 0 |
| Imipenem | ≥ 16 | ≥ 16 | 8 to ≥ 16 | 0 |
| Meropenem | ≥ 16 | ≥ 16 | 8 to ≥ 16 | 0 |
| Piperacillin-tazobactam | ≥ 128 | ≥ 128 | 32 to ≥ 128 | 0 |
| Colistin | 1 | 8 | ≤ 0.5 to 8 | 77.8 |
CR - carbapenem-resistant, DTR - difficult-to-treat
In the MDR group of P. aeruginosa isolates, colistin was the most active antibiotic (MIC50/90 = 1/4 mg/l, 89.2% susceptible), followed by ceftazidime-avibactam (MIC50/90 = 4/16 mg/l, 86.5% susceptible) and amikacin (MIC50/90 = 4/≥ 64 mg/l, 81.1% susceptible). In the CR group, colistin was the most active antibiotic (MIC50/90 = 1/4 mg/l, 88.9% susceptible), followed by ceftazidime-avibactam (MIC50/90 = 4/16 mg/l, 85.2% susceptible) and amikacin (MIC50/90 = 4/≥ 64 mg/l, 74.1% susceptible). In the DTR group, ceftazidime-avibactam exhibited an MIC50/90 of 4/≥ 128 mg/l with a susceptibility rate of 66.7%. The MIC50/90 of colistin was 1/8 mg/l, and the susceptibility rate was 77.8%.
In Fig. 1, the susceptibility results for each antibiotic are presented relative to meropenem susceptibility. When meropenem was non-susceptible, colistin demonstrated the highest susceptibility rate (88%), followed by ceftazidime-avibactam (84%).
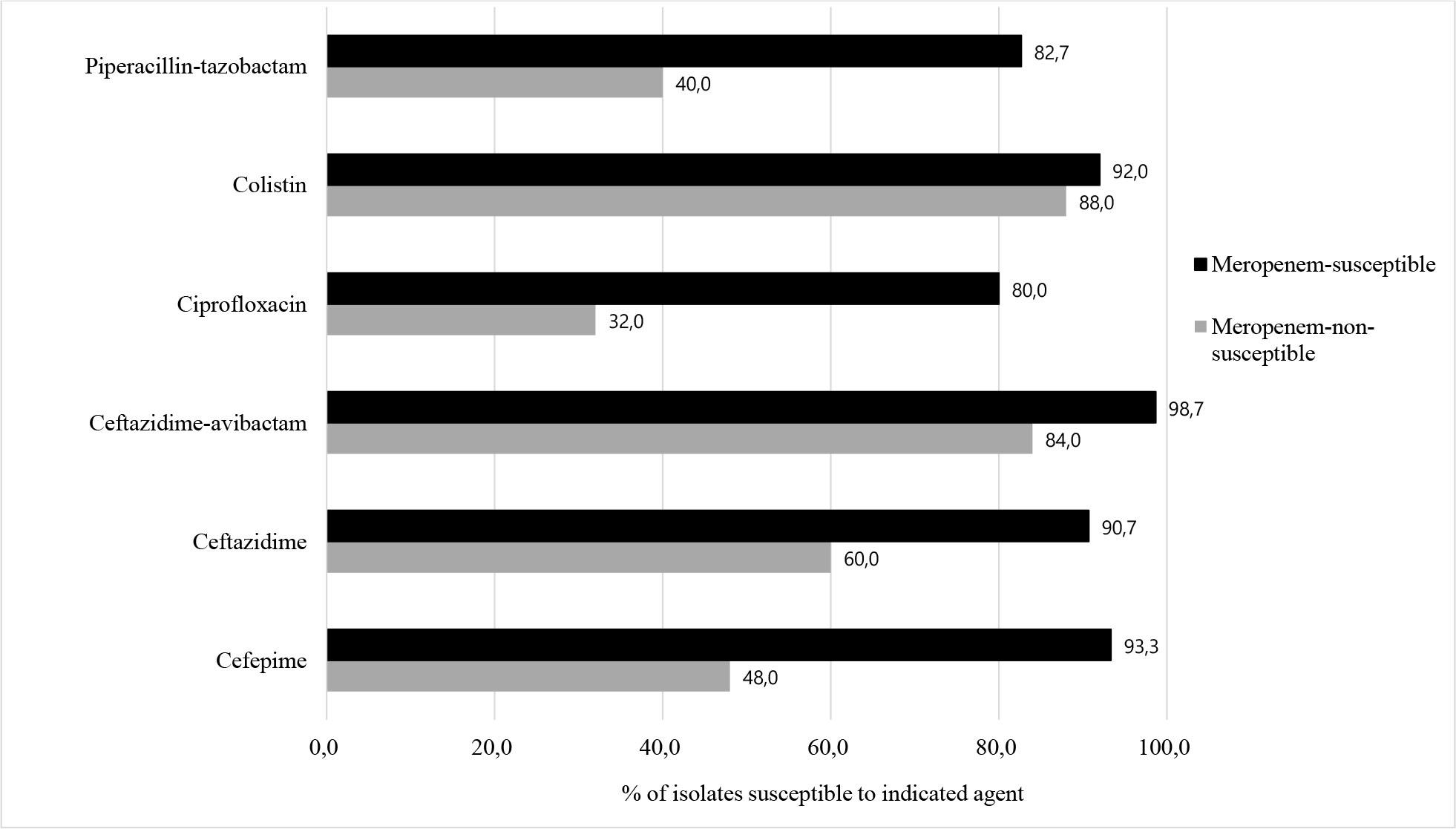
Comparisonof susceptibilitiesto selected agents between meropenem-susceptible and meropenem-non-susceptible Pseudomonas aeruginosa isolates. Black bars indicate meropenem-susceptible strains, while gray bars represent meropenem-non-susceptible strains.
Analysis of β-lactamases production in CR P. aeruginosa strains revealed that carbapenemase genes were detected in 4 of 27 isolates (14.8%), as summarized in Table IV. Specifically, one DTR strain produced an IMP-type carbapenemase, two DTR strains produced KPC-type carbapenemases, and one DTR strain co-produced both IMP- and KPC-type carbapenemases. All IMP-producing strains exhibited resistance to ceftazidime-avibactam. Among the two strains that produced only KPC-type carbapenemases, one was resistant to ceftazidime-avibactam, while the other had an MIC of 8 mg/l. The two KPC-producing strains demonstrated susceptibility to amikacin and gentamicin. In addition, one KPC-producing strain was non-susceptible to colistin, whereas the remaining three carbapenemase-producing strains were susceptible. Other β-lactamases, including VIM, SIM, GES, OXA-48, and NDM-1, were not detected.
Characteristics and antimicrobial susceptibility profiles of carbapenemase-producing Pseudomonas aeruginosa isolates.
| Characteristics | PA-57 | PA-16 | PA-28 | PA-40 |
|---|---|---|---|---|
| Carbapenemase | IMP | IMP + KPC | KPC | KPC |
| Clinical specimen | Genitourinary | Genitourinary | Genitourinary | Respiratory |
| MIC Values (mg/l) | ||||
| Amikacin | ≥ 64 | ≥ 64 | 4 | ≤ 2 |
| Gentamicin | ≥ 16 | ≥ 16 | 4 | 2 |
| Aztreonam | 32 | 32 | ≥ 64 | ≥ 64 |
| Ciprofloxacin | ≥ 4 | ≥ 4 | ≥ 4 | ≥ 4 |
| Ceftazidime-avibactam | ≥ 128 | ≥ 128 | 8 | 16 |
| Ceftazidime | ≥ 128 | ≥ 128 | 16 | 64 |
| Cefepime | ≥ 64 | 32 | ≥ 64 | 16 |
| Imipenem | ≥ 16 | ≥ 16 | ≥ 16 | ≥ 16 |
| Meropenem | ≥ 16 | ≥ 16 | ≥ 16 | ≥ 16 |
| Piperacillin-tazobactam | ≥ 128 | ≥ 128 | ≥ 128 | ≥ 128 |
| Colistin | ≤ 0.5 | 1 | 2 | 8 |
IMP - imipenem metallo-β-lactamase, KPC - Klebsiella pneumoniaae carbapenemases
This study analyzed antimicrobial susceptibility patterns, including susceptibility to ceftazidime-avibactam, in P. aeruginosa strains isolated from clinical specimens at a community-based hospital in Korea. The findings suggest that ceftazidime-avibactam holds promise as a viable alternative for the treatment of MDR P. aeruginosa infections.
We collected P. aeruginosa isolates from consecutive clinical samples obtained from both outpatients and hospitalized individuals. Of those isolates, 37% exhibited high-level resistance. The reported percentage of P. aeruginosa that were not susceptible to imipenem among samples obtained from Korean university hospitals was 14.6% in 1998 and 34.5% in 2016 (Bae et al. 2023). In a study on imipenem susceptibility in P. aeruginosa bacteremia at a Korean tertiary hospital, the percentage of imipenem-non-susceptible isolates was 18.4% (2009–2012), 30.9% (2013–2016), and 26.3% (2017–2020). Additionally, from 2017 to 2020, the prevalence of MDR P. aeruginosa was 38.6% and XDR P. aeruginosa was 21.1% (Kang et al. 2021). In our study, 24% of isolates were non-susceptible to imipenem, with MDR P. aeruginosa comprising 37% and DTR P. aeruginosa accounting for 9% of isolates. The frequency of antibiotic resistance observed in this study was comparable to or slightly lower than that reported by tertiary hospitals in Korea.
In a U.S. study of antibiotic resistance in P. aeruginosa isolates collected from 2012 to 2015, 15.4% of strains were MDR and 9.4% were XDR (Sader et al. 2017). In a study on P. aeruginosa resistance in the Asia-Pacific region between 2015 and 2019, 20.5% of the strains were MDR, 18.9% were CR, and 14.4% exhibited DTR. In Korea, 22.3% of P. aeruginosa isolates were MDR, with 16.7% resistant to carbapenems (Lee et al. 2022). In our study, the proportions of MDR and CR strains were higher than those reported in the United States or the Asia-Pacific region, although the percentage of DTR strains was lower.
Risk factors for MDR P. aeruginosa infection include prior hospitalization, intensive care unit (ICU) admission, previous antibiotic use, prior MDR P. aeruginosa colonization, and diabetes mellitus (Raman et al. 2018; Hernández-Jiménez et al. 2022). However, our study found no significant difference in antibiotic resistance between ICU and non-ICU isolates. Additionally, no statistically significant differences in MDR P. aeruginosa prevalence were observed concerning patient age, gender, or specimen source.
The Infectious Diseases Society of America recommends traditional non-carbapenem β-lactams over carbapenems when MDR P. aeruginosa is susceptible to both (Tamma et al. 2023). For DTR isolates resistant to fluoroquinolones and β-lactams, recommended options include ceftazidime-avibactam, ceftolozane-tazobactam, imipenem-cilastatin-relebactam, or cefiderocol (Tamma et al. 2023). In our study, 60% of MDR P. aeruginosa isolates were susceptible to imipenem and 52% to meropenem. Carbapenems were used in 29% of patients, with appropriate use in 100% of the non-MDR P. aeruginosa group and 38.9% in the MDR P. aeruginosa group. Since novel antibiotics were unavailable, colistin was used to treat MDR P. aeruginosa infections; 10 patients received colistin, and 90% used it appropriately. Colistin susceptibility was 91% overall, 89.2% in the MDR subgroup, 88.9% in the CR subgroup, and 77.8% in the DTR subgroup. These results indicate that colistin susceptibility remains relatively high. However, due to its limited therapeutic efficacy, colistin is recommended for use only when novel β-lactam/β-lactamase inhibitor combinations are unavailable (Aslan and Akova 2022). Moreover, the 2020 CLSI guidelines removed the “susceptible” category for colistin due to its various limitations (Satlin et al. 2020).
For ceftazidime-avibactam, susceptibility was observed in 95% of all isolates, 86.5% of the MDR P. aeruginosa group, 85.2% of the CR group, and 66.7% of the DTR group in this study. The MIC50 and MIC90 of ceftazidime-avibactam for all patients were 4 mg/l and 8 mg/l, respectively. In MDR and CR isolates, the MIC50 was 4 mg/l, and the MIC90 was 16 mg/l. For DTR isolates, the MIC50 was 4 mg/l, and the MIC90 was ≥128 mg/l. The susceptibility of P. aeruginosa collected in the Asia-Pacific region from 2012 to 2015 to ceftazidime-avibactam was 92.5%, with MIC50 and MIC90 of 2 mg/l and 8 mg/l, respectively (Karlowsky et al. 2018). In the Asia-Pacific region, from 2015 to 2019, the susceptibility of P. aeruginosa to ceftazidime-avibactam was 91.5%, with MIC50 of 2 mg/l and MIC90 of 8 mg/l. For MDR P. aeruginosa isolates, susceptibility was 60.9%, with respective MIC50/90 values of 8/256 mg/l. In the case of CR isolates, susceptibility was 59.7%, with MIC50/90 values of 8/256 mg/l, respectively. Additionally, for DTR isolates, the susceptibility was 48.7%, with MIC50/90 values of 16/256 mg/l, respectively (Lee et al. 2022). Our study found slightly higher susceptibility rates than previous studies, even among resistant isolates.
According to a 2018 report from the Centers for Disease Control and Prevention, 1.9% of CR P. aeruginosa isolates were identified as carbapenemase producers. Globally, metallo-β-lactamases are the predominant carbapenemases, with VIM and IMP among the most frequently detected. In contrast, KPC- and GES-producing P. aeruginosa strains have been reported more frequently in Europe and Asia. In contrast, carbapenemases such as GIM, NDM, and Florence imipenemase (FIM) are less commonly observed (Hammoudi Halat and Ayoub Moubareck 2022; Karruli et al. 2023). In a recent study conducted in South Korea, from 2015 to 2018, only IMP-type strains were detected among carbapenemase-producing P. aeruginosa. However, the prevalence of NDM-type strains has been increasing, accounting for 68% of the detected strains by 2020 (Jeong et al. 2024). In another nationwide surveillance study conducted in 2020, among 212 P. aeruginosa isolates detected in blood samples, 11 were identified as IMP-6 ST235 clones, and 10 were NDM-1 ST773 clones (Choi et al. 2023). A recent genomic analysis identified metallo-β-lactamase genes in approximately 13.6% of P. aeruginosa isolates, with blaVIM, blaNDM, and blaIMP variants being the most prevalent (Mack et al. 2025). The growing prevalence of metallo-β-lactamase-producing P. aeruginosa is expected to reduce ceftazidime-avibactam efficacy. To combat metallo-β-lactamases, treatment options include cefiderocol or a combination of aztreonam with avibactam. Additionally, other resistance mechanisms include efflux systems and changes in porins. In such cases, ceftolozane-tazobactam is more effective than ceftazidime-avibactam (Wi et al. 2018; Karruli et al. 2023). In this study, carbapenemase genes were detected in 14.8% of CR P. aeruginosa isolates collected between 2017 and 2018, including IMP- and KPC-type enzymes, while NDM-1 was not detected. All carbapenemase-producing isolates were classified as DTR P. aeruginosa and exhibited ceftazidime-avibactam MICs of ≥ 8 mg/l. The IMP-producing isolates were resistant to all tested antibiotics except colistin. Among the two isolates that produced only KPC-type carbapenemases, both demonstrated susceptibility to amikacin and gentamicin. With respect to colistin, one KPC-producing isolate was non-susceptible, whereas the remaining three carbapenemase-producing isolates were susceptible. Accurate identification of carbapenemase-producing strains and their resistance profiles is essential. The observed susceptibility to aminoglycosides in some KPC-producing isolates suggests potential therapeutic options, particularly in combination therapy. In settings where novel antibiotics are limited or unavailable, combination regimens including colistin may be considered a feasible treatment strategy despite its known adverse effects (Aslan and Akova 2022).
MDR P. aeruginosa infections are associated with poorer treatment outcomes than non-MDR infections, primarily due to limited therapeutic options (Huh et al. 2020; Hernández-Jiménez et al. 2022). In this study, the clinical success rate of patients infected with MDR P. aeruginosa was significantly lower than that of patients infected with non-MDR P. aeruginosa. Additionally, in-hospital mortality was greater among the MDR P. aeruginosa patients, with P. aeruginosa identified as the cause of death in 9.5% of the non-MDR P. aeruginosa patient group and 27% of the MDR P. aeruginosa patient group. These findings underscore the necessity of antibiotic administration for effective treatment of MDR P. aeruginosa in clinical practice. The emergence of MDR P. aeruginosa further highlights this concern, as these strains severely limit therapeutic options and can rapidly develop resistance, even to novel agents. In this context, the judicious use of new antibiotics, including ceftazidime-avibactam, is essential, with strict antimicrobial stewardship and infection control measures required to curb their spread and preserve treatment effectiveness (Tenover et al. 2022; Kim et al. 2024).
This study has several limitations. First, as the samples were obtained between 2017 and 2018, the resistance patterns and the epidemiology of β-lactamases observed here may not fully reflect current resistance trends. Second, the study was conducted at a single center, which may limit the generalizability of the findings. Third, susceptibility testing was limited to ceftazidime, ceftazidime-avibactam, and colistin using the broth microdilution method, while other antibiotics were tested using the MicroScan system. Finally, because the chart review was retrospective, it was not feasible to collect comprehensive data on all patients.
In conclusion, our findings indicate a high prevalence of antibiotic resistance among P. aeruginosa isolates from a community hospital, posing significant treatment challenges. Given the increasing prevalence of metallo-β-lactamase-producing P. aeruginosa, further studies are required to assess the clinical efficacy of ceftazidime-avibactam in real-world settings.