Phyllodes tumors are very rare breast neoplasms and account for less than 1% of all tumors. To date, no genetic predisposition has been identified for the development of this type of tumor except in individuals with Li-Fraumeni syndrome (1). Some studies cite trauma, pregnancy, and hormonal imbalance as possible risk factors, based on the stimulation of endothelin1 as a mediator of breast fibroblast growth (1). Biologically and histologically, they are classified as benign (most common), borderline and malignant types (very rare) (1). 5–15% of malignant cases metastasize hematogenously, most commonly to the lungs, bones, and brain (1). Clinically, they are presented as fast-growing, mobile, painless masses, over 5 cm in size, in women between 40–50 years of age. Ultrasound and mammography show sharp-edged, oval or round changes, with clear contours, which most often resemble fibroadenomas (1,2). Magnetic resonance imaging (MR) with basic and advanced sequences allows a more detailed evaluation of the phyllodes tumor. These are most often lobulated masses, clear contours, mixed structures, with internal septations and bleeding foci, hypointense on T1W, heterogeneous SI on T2W and STIR sequences, dynamic characteristics in the form of fast initial “wash in” and TIC curve by plateau type or “wash out”. MRI spectroscopy with choline quantification is very important as an indicator of malignant type (2). Ultrasound-guided core needle biopsy (CNB) is the next step in diagnosis and is a minimally invasive biopsy technique for palpable suspicious changes in the breast. Pathohistological analysis of the obtained samples shows the epithelial and stromal component, whose stroma determines the malignant potential of the tumor (2,3). Analysis of immunohistochemical markers p53, Ki67, EGFR has not been shown to be of the clinical significance for this type of neoplasm in previous studies (3).
Because of the rarity of this tumor there is a lack of sufficient prospective study data, especially for border and malignant tumors. 5-year disease-free survival rates of 96% is for benign and 66% for malignant types, while median survival after metastatic disease is poor, ranging from 4 to 17 months (4). The malignant type most often metastasizes to the lungs (66%), bones (28%) and brain (9%) (4,5).
According to the National Comprehensive Cancer Network (NCCN) guidelines for breast cancer, the management of phyllodes tumor dimension over 3.0 cm is a wide surgical excision with clean margins (≥ 1.0 cm) in the form of tumorectomy or mastectomy without axillary staging (6). The surgical approach is the method of choice in the treatment of phyllodes tumors in the form of tumorectomy or radical mastectomy with axillary dissection. The use of radiotherapy and chemotherapy depends exclusively on the extensiveness and biological nature of the tumor itself. Malignant phyllodes tumors do not respond to hormone therapy and chemotherapy, which are standard in the treatment of breast cancer. After postoperative treatment these patients should be closely followed up with regular clinical and ultrasound examinations (7,8).
We present the case of a 30-year-old patient in good general condition who noted a fast-growing, painless, clearly limited mass in her left breast. She had no other symptoms, no comorbidities and no data on trauma. Also, she had regular menstrual cycles, did not give birth and no family history of breast cancer. Anamnestic without other ailments and comorbidities, she did not give birth, regular menstrual cycles, no data on trauma, negative family history of breast cancer. The previous ultrasound examination peformed a year ago was unremarkable. Clinical examination revealed a palpabile formation measuring about 3 cm without significant axillary lymphadenopathy. Ultrasound examination detected a lobulated tumor mass dimension 35x28x11mm, heteroechoic structure, horizontally oriented with few oval shaped axillary lymph nodes up to 9 mm, mostly like reactive type, which is classified as BIRADS 4a (Figure 1).

Ultrasound axial plane showing lobulated, heteroechoic tumor mass
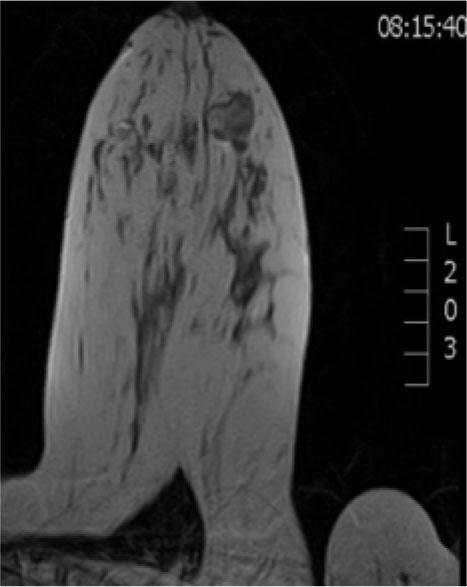
Axial MRI T2W section showing heterointense tumor mass
The review was supplemented by MRI examination, which showed retro and paramamilar tumor mass, in the lower outer quadrant, mixed signal intensity (SI) in T2W / STIR sequences, decreased SI in T1W sequence, postcontrast elevated SI, dynamic characteristics of rapid “wash in”, with a curve of plateau type with few oval shaped lymph up to 10 mm, classified as BIRADS 4 (Figures 2,3,4). Differential diagnostic could correspond to fibroadenoma or fibroadenoma like lesions (FA like lesion). CNB was performed under ultrasound control under local anesthesia and three samples were taken.
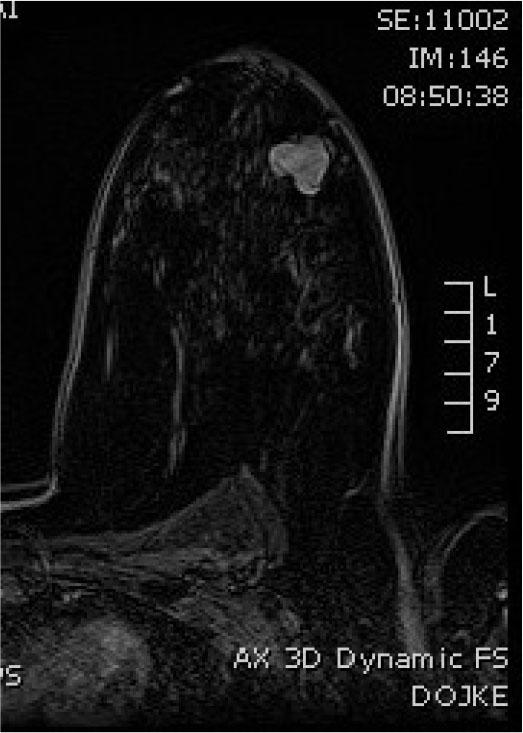
Axial poscontrast T1W section showing hiperintense, lobulated tumor mass

MIP poscontrast reconstruction axial plane showing tumor mass neovascularisation
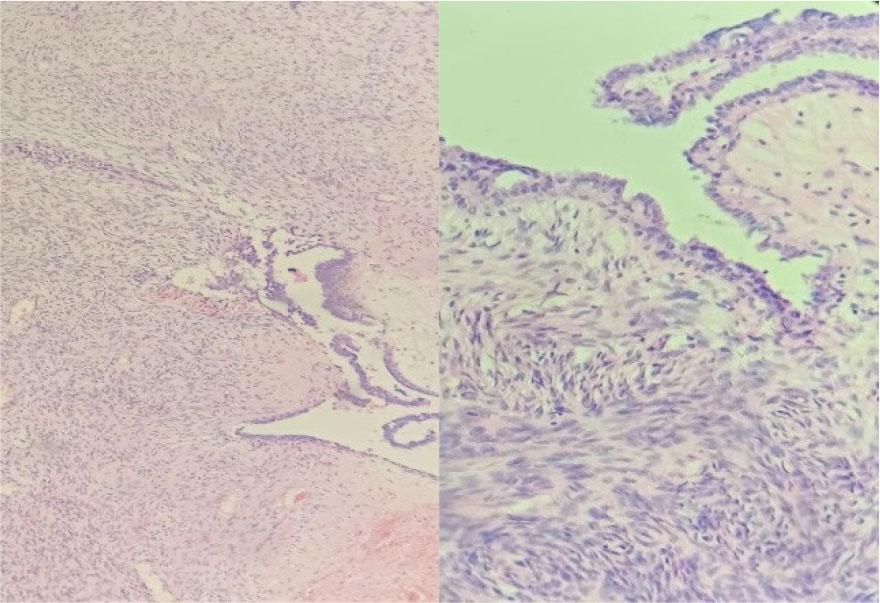
Pathohistological findings showing extensive stromal component, moderate to pronounced cellularity, focally high degree of atypia, with visible mitosis and minor foci of necrosis

Pathohistological findings showing moderate cellularity, focal moderate atypia, stromal component dominance
A pathohistological finding of malignant phyllodes tumor low grade was obtained, where two component tumor proliferation is observed in the analyzed tissue biopsy samples, in which the stromal component dominates in relation to the epithelial one. The epithelial component is sparse, leaf-like type of growth without signs of atypia. The stromal component is extensive, moderate to pronounced cellularity, moderate, focally high degree of atypia, with visible mitosis and minor foci of necrosis (Figure 5,6).
The case was presented in the oncologic consilium and taking into consideration the ultrasound, MRI examination and the pathohistological findings the surgical treatment was indicated. Retro and paramamilar tumor localization, and required wide excision margins could have limited the surgeon to achieve a good cosmetic result. Also, patient preference resulted in decision for radical mastectomy instead of breast sparing surgery as a preferable treatment of choice. Patient underwent a left radical modified mastectomy (Madden). Postoperative pathohistological findings confirmed the diagnosis of malignant phyllodes tumor low grade in which cellularity was moderate, atypia focal moderate, epithelial/mesenchymal component not monitored, dominance of stromal component, mitotic index focal about 5/10 HPF, necrosis: presents in about 10% of tumor tissue, growth mode mostly expansive, focally infiltrative, with negative resection margins and no significant morphological changes of the surrounding breast tissue. An immunohistochemical analysis was not performed. The presence of secondary tumor deposits (0 + / 9) were not observed in any of the nine histologically verified, reactively altered lymph nodes (figure 7).
The patient postoperative recovery was uneventful with well healed wound. She was referred to the oncologic consilium, where postoperative adjuvant radiotherapy was indicated. During her follow up for the first 11 months, the first clinical and ultrasound examination in 3 month and the second in 6 month showed no signs of local recurrence and metastasis.
Phyllodes tumors are very rarely mentioned in daily routine work. The great ultrasound resemblance to benign changes, primarily fibroadenomas, can lead a radiologist to misdiagnosis. An important anamnestic data on the rapid growth of changes in the breast, usually within a few months, as in the case of our patient, should lead an experienced clinician to suspect a phyllodes tumor with the need for further diagnostic procedures (4,5).
Ultrasound is the first diagnostic modality of evaluation of pathological changes, high sensitivity and specificity with the possibility of distinguishing cystic and solid lesions, but as a method it is very subjective and dependent on the experience of clinicians (3). Ultrasound characteristics that may indicate a malignant form are: dominant hypoechoic structure, irregular contours, and detectable vascularization. In our patient, based on the heteroechoic structure and pronounced vascularization of the pathological change, a suspicion of a phyllodes tumor was established, with an indication for MRI examination (4). Mammography was not performed in our case, due to the pronounced glandular structure of the breast and reduced diagnostic sensitivity.
MRI represents a unique combination of non-invasiveness and the possibility of precise visualization of anatomy, localization, characterization of pathological changes, assessment of disease extent, planning of adequate surgical treatment, as well as regular monitoring (4,5). In the case of our patient, there is a change in lobular contours, mixed structures with foci of necrosis, markedly vascularized without axillary lymphadenopathy, postcontrast dynamically rapid wash in and plateau-type curve. In previous studies, such dynamic characteristics indicate the possibility of benign change in 32% and malignancy in 68% of cases (5). Minimally invasive CNB under ultrasound control is indicated.
Ultrasound guided CNB under local anesthesia is the gold standard in the diagnosis of palpable breast masses. The method is fast, painless, minimally invasive and enables obtaining quality pathohistological samples for the purpose of efficient diagnosis. In the case of our patient, the obtained samples were sufficiently representative to diagnose a malignant phyllodes tumor.
According to the National Comprehensive Cancer Network (NCCN) guidelines for breast cancer, the management of phyllodes tumor dimension over 3.0 cm is a surgical wide excision with clean margins (≥ 1.0 cm) in the form of tumorectomy or mastectomy without axillary staging (6). Our patient underwent a radical mastectomy with axillary dissection, with postoperative radiotherapy. In terms of comparision breast conserving surgery and mastectomy for the treatment of borderline and malignant phyllodes tumors previous studies have shown conflicting results (9,10,11). Local recurrence appears to be related to the extent of the initial surgery. Providing clear margins are maintained than breast conservation is preferable, but even with wide surgical resection, the local recurrence rate remains high 8 to 36% (11,12). Some studies showed no significant difference between breast conserving surgery and mastectomy regarding overall survival, although the patients who underwent breast conserving surgery had higher recurrence rate. Phyllodes tumors grow radially, compress the adjacent breast parenchyma and create a pseudo-capsule through which tongues of phyllodes stroma may protrude and grow into adjacent breast tissue. For this reason, many authors support that mastectomy may be the best surgical procedure for the borderline or malignant phyllodes tumor. In our case localization, required wide excision margins, pathohistological findings and patient preference resulted in decision for radical modified mastectomy instead of breast conserving surgery as a treatment of choice (10,12).
The rate of local recurrence in the first 2 years is high ranging from 10 to 40% in all three histological types and directly depends on the size and the hystological grade of the primary operated tumor (8,11,13). Compared to benign and borderline, malignant phyllodes types regardless tumor size have a higher rate of disease recurrence, decreased overall survival and distant metastasis. It is well documented that recurrent phyllodes tumors can progress to a more malignant phenotype comparing to the the initial tumor. Also, it was showed that stromal overgrowth, high stromal cellularity, large tumor size and mitotic rate are histological features associated with high risk of recurrence. Specifically, data support that stromal overgrowth is a key predictor of disease relapse, while stromal cellularity and high mitotic rate are less consistently (8,13). To date, no single immunomarker can reliably distinguish between benign and borderline phyllodes and also to accurately predict clinical behavior in all cases. Further studies are required to establish the correct combination of immunomarkers (14). In our case pathohistological findings showed dominance of tumor stromal component, stromal cellularity, atypia and mitotic rate, whereby this tumor could be classified as a tumor with high reccurence risk.
The incidence of axillary lymph node involvement in malignant form is low, ranging from 1.1% to 3.8% (8). In spite of the lack of supporting data for lymph node dissection review of current surgical practice reveals that axillary staging continues to be performed for many cases of malignant phyllodes tumors (12,16). Data regarding sentinel lymph node biopsy in phyllodes tumors are lacking. In our case ultrasound and MRI examination revealed insignificant lymphadenopathy, most likely of the reactive type, but given the pathohistological findings it was decided to perform axillary dissection.
Previous studies have showed that young age (<35 years) is an adverse prognostic factor for reccurence free survival in patients with malignant phyllodes tumor, while older age (>50 years) was correlated with advanced tumor extension and poor cancer-specific survival (8,15). These findings may help to distinguish the patients at high risk of developing local recurrence and imply that surgery such as wide local excision and mastectomy, should be performed on younger patients, especially with malignant phyllodes tumors.
Still, there is no consensus regarding the recommendations for radiotherapy, hormonal therapy and systemic chemotherapy. Because of the rarity of this tumor there is a lack of sufficient prospective study data, especially for border and malignant tumors (9,16,17). Currently, the use of adjuvant therapy remains controversial, but it has been more frequently utilized. According to a study in the National Cancer Database from the American College of Surgeons’ Commission on Cancer involving 3120 patients in 2008–2009 year, adjuvant radiotherapy was used in 19.5% of cases, more than doubled compared to the rate of 9.5% in 1998–1999 year. Many authors support that in patients. Many authors support that in patients with malignant phyllodes tumor adjuvant radiotherapy may be more effective in younger patient and should be used without consideration of the surgery type. It is associated with an increased time to local recurrence compared to women who had surgery alone (10,16,17). In our case taking into account patients age and pathohistological findings the oncologic consilium recommended the adjuvant radiotherapy.
To date, there has been only one prospective study involving 28 patients, which has showed that chemotherapy has little effect on survival (9). The sample sizes of few retrospective studies were too small to prove the efficacy of chemotherapy (9,18). For this reason, most clinicians avoid chemotherapy as a first-line treatment due to lack of evidence. Our patient did not received chemotherapy.
After operative treatment, this group of patients should be followed up with regular physical and ultrasound examinations (8,9,19). In our case during postoperative follow up for the first 11 months, patient has been feeling well, with good quality of life and no current signs of local recurrence and metastasis.
Malignant phyllodes tumors do not respond to hormonal and chemotherapy, which is standardly used in the treatment of the breast cancer. The malignant type most often metastasizes to the lungs (66%), bones (28%) and brain (9%). The incidence of axillary lymph node involvement in malignant form is low, ranging from 1.1% to 3.8% In the case of hematogenous dissemination, this type of tumor is treated according to the sarcoma treatment protocol. Because, there are not many reports of phyllodes tumors, past case reports and studies have reported that the rate of local recurrence in all three histological types or in the form of distant metastases in the first 2 years is up to 27% and directly depends on the size of the primary operated tumor .Also, 5-year disease-free survival rates of 96% is for benign and 66% for malignant .types., while median survival after metastatic disease is poor, ranging from 4 to 17 months. Compared to benign and borderline, malignant phyllodes types have a higher rate of disease recurrence, decreased overall survival, and distant metastasis. After surgical treatment, this group of patients requires regular monitoring in the form of ultrasound examinations. (8,9) Our patient has been feeling well since the time of surgery with no current signs of metastasis or local recurrence.
Phyllodes breast tumors, especially malignant cases are very rarely referred to by foreign and domestic authors. One of the work is a review of a patient who was treated for a giant exulcerated borderline philodes breast tumor (10,20).
We conclude that phyllodes tumors, especially malignant forms are very rarely thought of in routine daily work and there is a high likelihood of missing these tumors. Important anamnestic data on the rapid growth of the breast palpable mass, regardless of the age of the patient with the initial ultrasound examination is should be the main indication for further diagnostic evaluation. It is necessary to be vigilant in the prompt diagnosis and management of this rare tumors. The early diagnosis is crucial for improving the overall outcome of the disease after treatment, as well as for promoting the good quality of life of the patient. With a precise choice of diagnostic multimodalities this tumor can be successfully treated. Still, there are various types of treatment modalities for phyllodes tumors. The surgical treatment is the gold standard, but should be better tailored in the management of malignant or recurrent tumors. The role of adjuvant radiotherapy and chemotherapy remains uncertain, but encouraging. It is certain, that future prospective studies with more patients are required.