
The association of elevated HbA1c values with functional outcomes has been explored from a single center in Saudi Arabia, according to the TOAST subtypes in this study. Higher admission HbA1c values independently affected the functional recovery of patients in the study cohort after adjusting for stroke subtypes and other recognized variables. However, the incremental predictive value of HbA1c beyond established clinical predictors (like NIHSS, age, and etiologic subtypes) is modest, despite its statistical significance. Further large sample-sized multi-center studies are needed to consider HbA1c as an important standalone biochemical prognostic biomarker in patients with AIS.
Acute ischemic stroke (AIS) is a heterogeneous disease with multiple etiologies that contributes substantially to mortality and long-term residual disability [1]. Determination of underlying etiology according to the TOAST criteria is essential, as risk factor management, acute treatment strategies, and prognostic outcomes vary among the different etiologic subtypes [2]. Notably, stroke affects a relatively younger population among Asian countries, including the Kingdom of Saudi Arabia (KSA), underscoring the need for vigilant management of modifiable risk factors, including diabetes mellitus (DM) which is the cause of chronic hyperglycemia (CH) [3].
Importantly, acute stress hyperglycemia (AH) in patients without known DM can sometimes confound diagnosis, leading to misclassification as new-onset diabetes, and therefore it is important to measure Glycated hemoglobin (HbA1c) levels at the time of arrival, which reflects average glycemic levels over the preceding 2–3 months [4]. HbA1c serves as a reliable biochemical marker for confirming CH [4]. Notably, HbA1c has emerged as a marker for predicting stroke severity, therapeutic response to endovascular treatment (EVT) and 90-days outcome. A recent meta-analysis has suggested that HbA1c may predict stroke prognosis and should therefore be measured at the time of admission to guide early disability-prevention strategies [5].
Recently, a study from KSA has reported an association of HbA1c with stroke severity and mortality [6]. Furthermore, elevated HbA1c levels have also been shown to adversely affect the successful therapeutic response to EVT for large vessel occlusion (LVO) [7,8,9]. Nevertheless, the relationship between glycated hemoglobin levels and outcomes in patients with AIS remains controversial. While some studies have reported an independent relationship between elevated HbA1c and poor functional outcomes after AIS [10,11,12], others have failed to demonstrate such a relationship [13,14]. Jeong et al. [13] found that the impact of HbA1c on both short as well as long-term outcomes after AIS was influenced by patient age and stroke subtype. A recent Saudi Arabian study [15] highlighted a link between HbA1c levels and intracranial atherosclerosis–related AIS, emphasizing the need to optimize the management for CH as the levels were higher. However, the association across different TOAST stroke subtypes was not explored. Alfakeeh et al. [16] similarly reported significantly elevated HbA1c levels among Saudi patients with stroke, indicating suboptimal glycemic control that warrants closer attention and management.
Given the inconsistency in previously reported findings, this study aimed to evaluate the effect of CH, assessed by HbA1c levels at admission, on 3-month functional recovery among patients with AIS of various etiologic subtypes. There is a paucity of data on the effect of CH on outcomes in stroke patients from the region according to TOAST subtypes, which are a major determinant of prognosis; therefore, we attempted to bridge this gap by conducting this study. The KSA has a population in which the patients with AIS are relatively younger and have a higher prevalence of modifiable risk factors [3,15,16]. Publishing this study may significantly influence practitioners’ therapeutic interventions to improve glycemic control in high-risk patients.
This is a retrospective and observational study, which was conducted at the Neurology Department of King Fahd Hospital, affiliated with Imam Abdulrahman Bin Faisal University (IAU). The study was conducted after approval by the IAU Institutional Review Board Ethics Committee (IRB-2024-03-235) obtained in 2024. Data of all patients admitted with the diagnosis of AIS between January 2018 and September 2023 were reviewed retrospectively and included. Adult patients, ≥18 years with a confirmed diagnosis of AIS by clinical evaluation and radiological findings, as recommended by the World Health Organization criteria [17], were enrolled. Each diagnosis was verified by both a neuro-radiologist and a stroke neurologist. Patients diagnosed with non-ischemic conditions, including transient ischemic attack, intracerebral hemorrhage, brain abscess, tumor, or dural sinus thrombosis, were excluded.
Data were reviewed and retrieved from the digital medical record system of the hospital. The collected variables included patient demographics such as age and sex, along with clinical characteristics including the presence of vascular risk factors, comprising hypertension (HTN), diabetes mellitus (DM), ischemic heart disease (IHD), atrial fibrillation (AF), dyslipidemia (DLP), smoking status, prior stroke history, and the National Institutes of Health Stroke Scale (NIHSS) score at the time of arrival after symptoms onset. Biochemistry laboratory parameters, including fasting blood sugar (FBS) and glycated hemoglobin (HbA1c) values were collected. Radiological findings, including brain computed tomography (CT) and magnetic resonance imaging (MRI), were reviewed for each patient. Infarctions were categorized according to the vascular territory and cerebral area affected as the total anterior circulation infarction (TACI), partial anterior circulation infarction (PACI), posterior circulation infarction (POCI), and lacunar infarction (LI). TOAST criteria were applied to classify and determine stroke subtypes as large artery atherosclerotic disease (LAA), small vessel occlusive disease (SVO), cardioembolic (CE), other determined (OD), or undetermined (UD) etiologies [2].
Functional recovery was evaluated by assessing the modified Rankin Scale (mRS) at 90 days and was categorized as good functional outcome (FOC) for mRS 0–2 or poor FOC for mRS 3–6 [18]. As this was a retrospective analysis utilizing de-identified electronic data, verbal informed consent requirement was waived according to the policy.
All data analyses were performed using IBM SPSS Statistics, version 27 (IBM Corp., Armonk, NY, USA). Continuous variables and quantitative data were expressed as either mean ± standard deviation (SD) or median with interquartile range (IQR), where appropriate. Categorical variables were summarized as frequencies and percentages.
The Pearson chi-square test or Fisher’s exact test were applied to do comparisons between different categorical variables were evaluated using while independent t-tests were applied for continuous variables. For quantitative non-normally distributed data, the independent-Samples Mann-Whitney U Test was used, and for quantitative normally distributed data, the independent sample t-test was applied. A p-value < 0.05 was set as statistically significant.
The strength of statistical association between different demographic, clinical, and radiological variables and functional recovery was examined applying the chi-square test and risk was expressed by calculating the odds ratios (ORs) and 95% confidence interval (95% CI). To control for potential confounders, multivariate logistic regression (MLR) models were constructed calculating adjusted ORs and 95% confidence intervals (CIs) to establish the significant association between HbA1c and outcomes, adjusting for variables, found significant during univariate analysis. HbA1c was studied as a continuous variable. Binary logistic regression was performed to create models predicting prognosis including all variables found significantly associated with poor recovery with and without HbA1c. ROC were later performed to find the strength of both models. The receiver operating characteristic (ROC) curve analysis was also performed to find the strength of association between HbA1c and FOC in the whole study cohort and for each TOAST subtype.
In total, 518 patients were included in the final data analysis. Men comprised more than half of the cohort, with a male-to-female ratio of 2.1:1. The mean ± standard deviation (SD) age was 56.4 ± 14.4 years, with a median (interquartile range [IQR]) of 56 (46–66) years. In all AIS patients, the mean ± SD HbA1c level was 7.94 ± 2.51, with a median (IQR) of 7.10 (5.9–9.9). The median (IQR) for NIHSS score at admission was 6 (3–10).
The most frequent AIS subtype was LAA, determined in 34.4% of the total patients, followed by SVO in 29.7%. Patients with CE and LAA strokes were relatively older than those with other etiologic subtypes. Baseline demographic, clinical, and radiological characteristics stratified by TOAST classification are summarized in Table 1. Age, sex distribution, NIHSS scores, and vascular risk factor prevalence significantly differed among the various stroke subtypes. The greatest male predominance was observed in the LAA subtype (p = 0.017).
Characteristics of patients, including demographic and clinical characteristics according to different TOAST subtypes
| Variables | All patients | Large artery atherosclerosis type | Cardioembolic type | Small vessel occlusive type | Other determined | Undetermined | p value |
|---|---|---|---|---|---|---|---|
| Men | 383(74) | 144(80.9) | 55(64) | 118(76.1) | 18(66.7) | 48(66.7) | 0.017 |
| Age | |||||||
| means±SD | 56.4±14.4 | 59.6±12.7 | 59±16.6 | 54.2±12.7 | 41.5±13.0 | 55.7±15.5 | <0.001 |
| median (IQR) | 56(46–66) | 58(50–69) | 60(45.7–74.2) | 52.5(44–62) | 40(34–48.7) | 58(42–67) | |
| Diabetes mellitus | 347(67) | 143(80.3) | 51(59.3) | 102(65.8) | 6(22.2) | 45(62.5) | <0.001 |
| Hypertension | 344(66.4) | 139(78.1) | 49(57) | 102(65.8) | 13(48.1) | 41(56.9) | <0.001 |
| IHD | 108(20.8) | 31(17.4) | 42(48.8) | 22(14.2) | 3(11.1) | 10(13.9) | <0.001 |
| Dyslipidemia | 254(49) | 97(54.5) | 41(47.7) | 74(47.7) | 9(33.3) | 33(45.8) | 0.26 |
| Previous stroke/TIA | 92(17.8) | 46(25.8) | 12(14) | 18(11.6) | 6(22.2) | 10(13.9) | 0.008 |
| Smoking | 135(26.1) | 52(29.2) | 20(23.3) | 42(27.1) | 7(25.9) | 14(19.4) | 0.55 |
| Arrived within therapeutic window | 235(45.4) | 61(34.3) | 55(64) | 71(45.8) | 13(48.1) | 35(48.6) | <0.001 |
| NIHSS | |||||||
| means±SD | 7.7±5.9 | 8.8±6.2 | 10.3±6.8 | 4.8±3.1 | 8.1±5.3 | 8.5±6.2 | <0.001 |
| median (IQR) | 6(3–10) | 7(4–13) | 9(4–16) | 4(3–7) | 7(3–12) | 7(3.2–12) | |
| Hyperacute treatment | 158(30.5) | 49(27.5) | 35(40.7) | 35(22.6) | 13(48.1) | 26(36.1) | 0.004 |
| Territorial anterior circulation infarct | 46(8.9) | 25(14) | 12(14) | 0 | 5(18.5) | 4(5.6) | <0.001 |
| Partial anterior circulation infarct | 202(39) | 90(50.6) | 58(67.4) | – | 12(44.4) | 40(55.6) | <0.001 |
| Posterior circulation infarct | 97(18.7) | 51(28.7) | 14(16.3) | – | 8(29.6) | 22(30.6) | <0.001 |
| Lacunar infarct | 168(32.4) | 9(5.1) | – | 155(100) | 4(5.6) | <0.001 | |
| HbA1c | |||||||
| means±SD | 7.9±2.5 | 8.69±2.6 | 7.23±2.3 | 7.86±2.3 | 6.30±1.6 | 7.70±2.5 | <0.001 |
| median (IQR) | 7.1(5.9–9.7) | 8.15(6.5–10.9) | 6.4(5.6–8.3) | 7.1(5.9–9.9) | 5.8(5.4–6) | 6.9(5.7–9.4) | |
| Poor functional recovery | 181(35) | 85(47.8) | 41(47.7) | 24(15.5) | 6(22.2) | 25(34.7) | <0.001 |
| Good functional recovery | 337(65) | 93(52.2) | 45(52.3) | 131(84.5) | 21(77.8) | 47(65.3) | <0.001 |
Note: Data are represented as number (%).
Patients with LAA subtype exhibited the highest mean HbA1c values (8.69 ± 2.6) among all groups, followed by the SVO subtype. Overall, 35% of the cohort had poor FOC at 3 months. The association of demographic and clinical variables with FOC is presented in Table 2. Patients with poor FOC had significantly higher age than those with favorable outcomes (p < 0.001). The presence of DM, HTN, IHD, previous stroke, and AF, and large territorial infarctions were each associated with poor outcomes. Higher admission NIHSS scores were also predictive of poor FOC compared to lower scores.
Distribution of demographic and other clinical variables including HbA1c levels between patients with good and poor functional recovery
| Variable (n) | Good functional recovery | Poor functional recovery | *Odds Ratio | 95% confidence interval | P value |
|---|---|---|---|---|---|
| Age (mean±SD) | 54.5±14.07 | 60±14.49 | – | <0.001 | |
| Male (383) | 254 (75.3) | 129 (71.3) | 0.87 | 0.67–1.13 | 0.34 |
| Hypertension (344) | 212 (62.9) | 132 (72.9) | 1.36 | 1.03–1.78 | 0.02 |
| Diabetes mellitus (347) | 213 (63.2) | 134 (74) | 1.40 | 1.06–1.85 | 0.012 |
| Ischemic heart disease disease (108) | 61 (18.1) | 47 (26) | 1.33 | 1.03–1.72 | 0.03 |
| Dyslipidemia (254) | 160 (47.5) | 94 (51.9) | 1.12 | 0.88–1.42 | 0.33 |
| Prior H/O stroke (92) | 46 (13.6) | 46 (25.5) | 1.57 | 1.23–2.02 | 0.001 |
| Atrial fibrillation (45) | 20 (5.9) | 25 (13.8) | 1.83 | 1.36–2.47 | 0.001 |
| NIHSS on presentation (Mean±SD) | 5.31±4.00 | 12.57±6.0 | – | <0.001 | |
| TOAST subtypes | |||||
| Large artery atherosclerosis (178) | 93 (27.6) | 85 (46.9) | 1.69 | 1.34–2.12 | <0.001 |
| Cardio-embolic (86) | 45 (13.4) | 41 (22.7) | 1.47 | 1.13–1.90 | 0.007 |
| Small vessel occlusion (155) | 131 (38.8) | 24 (13.3) | 0.35 | 0.24–0.52 | <0.001 |
| Other determined (27) | 21 (6.2) | 06 (3.3) | 0.62 | 0.30–1.27 | 0.15 |
| Undetermined (72) | 47 (13.9) | 25 (13.8) | 0.99 | 0.70–1.39 | 0.96 |
| Territorial anterior circulation infarct (46) | 5 (1.5) | 41 (22.7) | 3.00 | 2.53–3.56 | <0.001 |
| Partial anterior circulation infarct (202) | 121 (35.9) | 81 (44.8) | 1.26 | 1.00–1.60 | 0.04 |
| Lacunar infarct (168) | 142 (42.1) | 27 (14.9) | 0.36 | 0.25–0.52 | <0.001 |
| Posterior circulation infarct (97) | 66 (19.6) | 31 (17.1) | 0.89 | 0.65–1.23 | 0.49 |
| Hyper acute treatment (158) | 103 (30.6) | 55 (30.4) | 0.98 | 0.76–1.26 | 0.88 |
| HbA1c (Mean±SD) | 7.57±2.25 | 8.61±2.83 | <0.001 |
Note: *OR are adjusted for poor functional outcome.
Among the TOAST etiologic subtypes, both LAA and CE were significantly associated with higher odds of poor FOC compared with SVO. Specifically, LAA was associated with OR = 1.69 (95% CI, 1.34–2.12; p < 0.001) and CE with OR = 1.47 (95% CI, 1.13–1.90; p = 0.007), whereas SVO showed a significantly lower likelihood of poor FOC with OR = 0.35 (95% CI, 0.24–0.52; p < 0.001). SVO was the only subtype that was associated with higher likelihood of good functional recovery with OR = 1.48 (95% CI, 1.33–1.66; p < 0.001). OD and UD subtypes didn’t demonstrate any significant association with outcomes.
HbA1c demonstrated a significant association with FOC in the whole study cohort (p = < 0.001), with higher values correlating with poor FOC, as shown in Figure 1a. When stratified by TOAST subtype, higher HbA1c values remained significantly associated with poor FOC in the LAA (p = 0.027), CE (p = 0.046), and SVO (p = 0.021) subtypes as illustrated in Figure 1b, 1c, and 1d respectively. Whereas UD and OD subtypes didn’t demonstrate any significant association between admission HbA1c levels and FOC, (p = 0.37) and (p = 0.79), respectively. Importantly, HbA1c remained statistically significant after full adjustment for all variables found significant during initial analysis including age, NIHSS, LAA, CE subtype, and comorbidities such as DM, HTN, IHD, prior stroke, and AF (p < 0.001; OR = 1.27; 95% CI, 1.12–1.45).
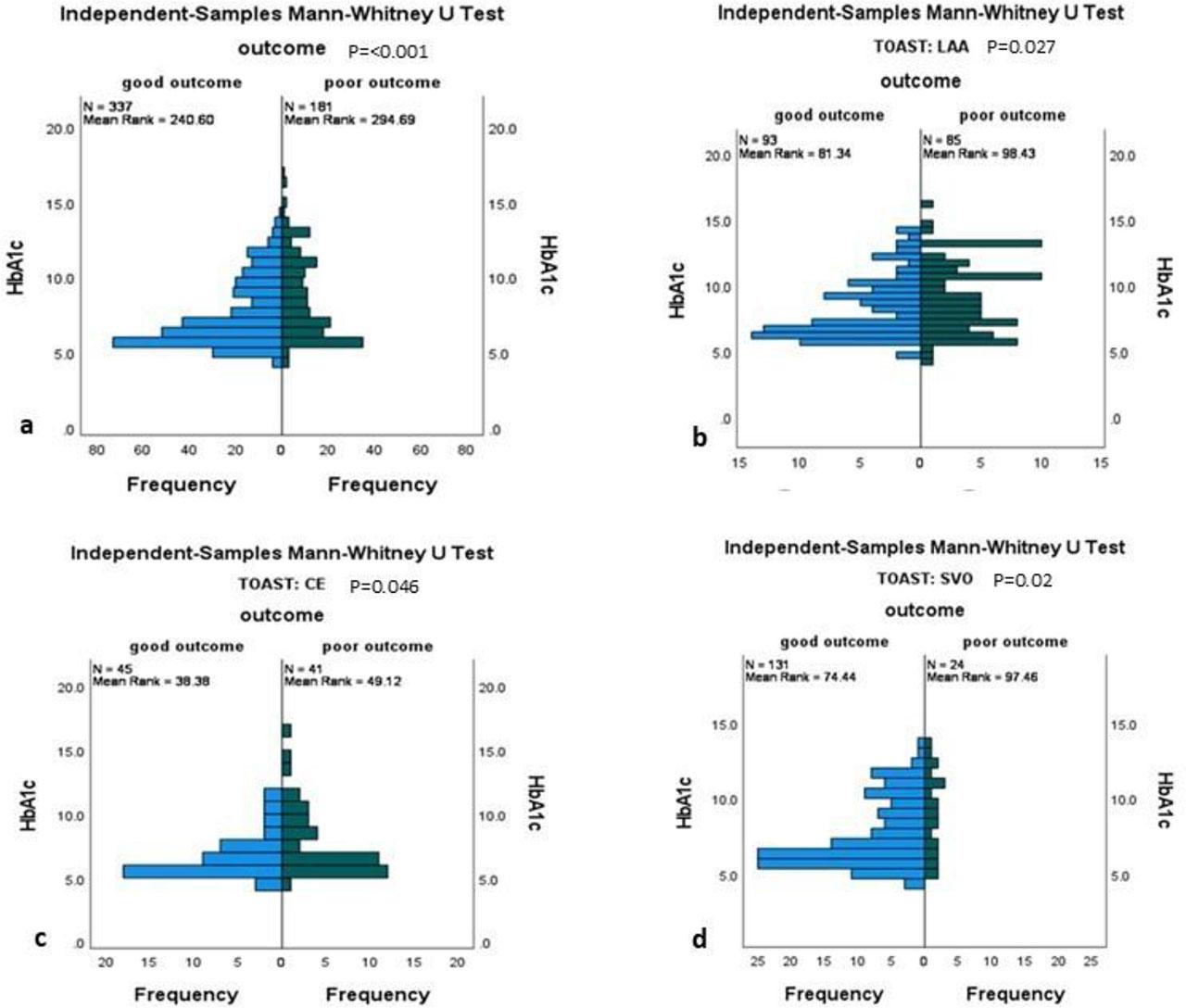
HbA1c distribution according to the outcomes among, a; all patients with Acute ischemic stroke, b; with large artery atherosclerosis (LAA) stroke subtype, c; cardioembolic (CE) stroke subtype, d; small vessel occlusive (SVO) stroke subtype.
Adjustment for variables found to be significantly associated with poor functional recovery for each etiologic subtype was also performed. In LAA subtype, prior stroke was the only risk factor that was associated with poor FOC. All patients with TACI had poor FOC in LAA subtype (p < 0.001; OR = 2.25; 95% CI, 2.09–3.10). When adjusted for TACI in LAA subtype, HbA1c exhibited a statically significant association (p = 0.04; OR = 1.14; 95% CI, 1.00–1.30). In CE subtype, age (p < 0.001) and AF (p = 0.02; OR = 1.68; 95% CI, 1.08–2.61) were the only risk factors, associated with poor FOC. In SVO subtype, female sex, HTN and IHD were associated with poor FOC, and these were adjusted during MLR. The relationship between HbA1c and poor FOC across multivariate models is summarized in Table 3.
Multiple models of Logistic regression analysis for association of HbA1c with poor functional recovery in all patients with acute ischemic stroke
| Variables | Odds ratio | 95% confidence interval | P value |
|---|---|---|---|
| Model 1, adjusted for NIHSS | |||
| HbA1c | 1.29 | 1.17–1.41 | <0.001 |
| NIHSS | 1.32 | 1.25–1.39 | <0.001 |
| Model 2, adjusted for CE subtype | |||
| HbA1c | 1.20 | 1.11–1.29 | <0.001 |
| CE subtype (yes versus no) | 2.30 | 1.41–3.75 | 0.001 |
| Model 3, adjusted for LAA subtype | |||
| HbA1c | 1.14 | 1.06–1.23 | <0.001 |
| LAA subtype (yes versus no) | 2.02 | 1.37–2.98 | <0.001 |
| Model 4, adjusted for SVO subtype | |||
| HbA1c | 1.18 | 1.09–1.27 | <0.001 |
| SVO subtype (yes versus no) | 0.23 | 0.14–0.38 | <0.001 |
| Model 5, adjusted for subtypes associated with poor recovery (LAA and CE) | |||
| HbA1c | 1.16 | 1.08–1.26 | <0.001 |
| LAA | 2.91 | 1.90–4.47 | <0.001 |
| CE | 3.66 | 2.15–6.22 | <0.001 |
| Model 6, Model adjusted for risk factors | |||
| HbA1c | 1.25 | 1.13–1.39 | <0.001 |
| Age | 1.02 | 1.00–1.03 | 0.01 |
| DM | 0.59 | 0.32–1.08 | 0.09 |
| HTN | 1.29 | 0.81–2.04 | 0.27 |
| IHD | 1.48 | 0.91–2.41 | 0.11 |
| AF | 2.52 | 1.26–5.06 | 0.009 |
| Prior stroke | 1.32 | 0.76–2.29 | 0.31 |
The ROC curve analysis in our study cohort identified an optimal HbA1c cut-off value of 6.8% by Youden’s index for predicting poor outcome, yielding a sensitivity of 65.7% and a specificity of 50.1%, with an area under the curve (AUC) = 0.604 (p < 0.001), indicating modest predictive performance. In univariate analysis, HbA1c ≥ 6.8% was significantly associated with poor FOC (p = 0.04; OR = 2.4; 95% CI, 1.10–5.7). This association remained significant after multivariate adjustment for TOAST etiologic subtype (p = 0.01; OR = 1.66; 95% CI, 1.11–2.44), and after full adjustment, confirming independent predictive value. HbA1c < 6.8% had lower likelihood of poor FOC (p = 0.016; OR = 0.62; 95% CI, 0.42–0.91), after adjusting for LAA and CE subtypes, the etiologies significantly associated with poor FOC. HbA1c < 6.8% was associated with better FOC, reinforcing the clinical relevance of this cut-off. When performed for each etiologic subtype, the SVO subtype showed the most significant association of HbA1c with outcome among all subtypes as shown in Figure 2. Models predicting poor FOC; including all variables demonstrating significant association during univariate analysis without and with HbA1c, are shown in Figure 3. Baseline NIHSS were consistently included in these fully adjusted models, given its well-established role as a key predictor of stroke functional recovery. Both models, without and with HbA1c, exhibited a strong association with an AUC of 0.869 and 0.878, respectively. However, adding HbA1c increased the strength of association slightly, limiting its significance in an independent capacity.
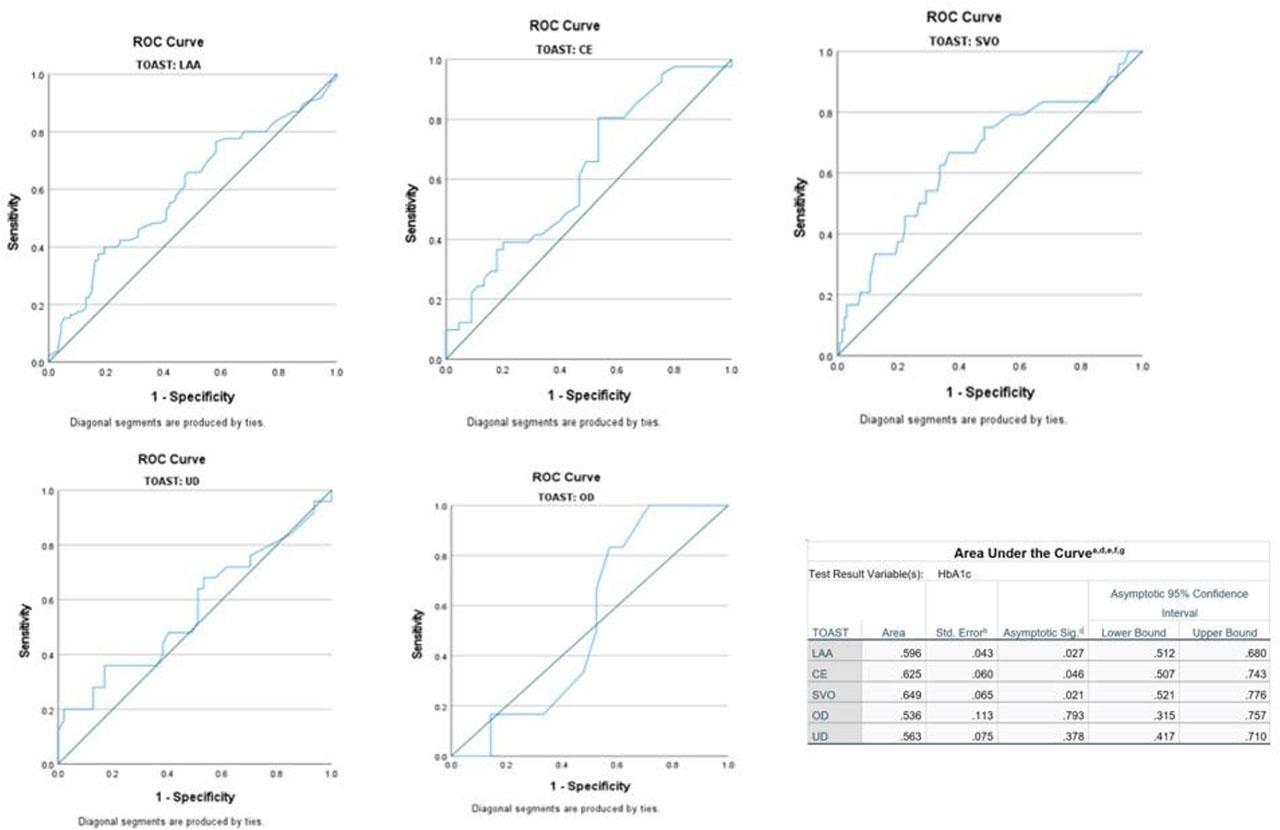
ROC analysis demonstrating an association of HbA1c with functional recovery in different TOAST subtypes.
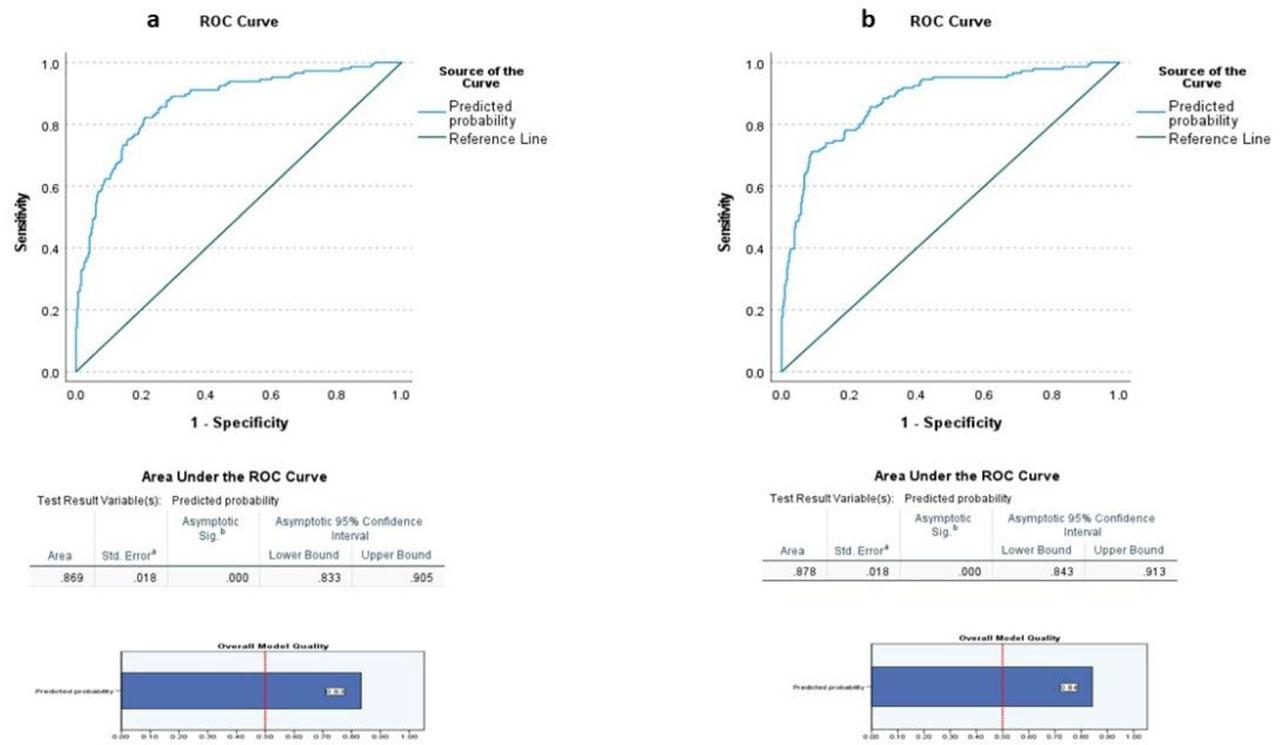
Models (including all variables demonstrating significant association during univariate analysis; age, NIHSS, DM, HTN, IHD, previous stroke, AF, LAA, and CE subtypes) predicting poor functional recovery in patients with acute ischemic stroke, model 1 – without incorporating HbA1c, model 2 – with HbA1c.
This study evaluated the association between CH reflected by elevated HbA1c levels and 90-day FOC in patients with AIS, irrespective of age or previously known diabetes status. Stroke subtypes were determined according to the TOAST system to examine whether the prognostic effect of HbA1c varied across different etiologic mechanisms or not. Consistent with previous reported literature, we found that older age, higher admission NIHSS, and vascular risk factors, particularly DM, HTN, IHD, prior stroke, and AF, were associated with poor outcomes. These findings align with established predictors of stroke severity and recovery reported in prior systematic reviews and cohort studies over the past few decades [19,20,21].
Underlying stroke etiology plays a pivotal role in predicting FOC. In our cohort, LAA was the most common underlying etiology, followed by SVO. In our study cohort, LAA and CE subtypes demonstrated a significantly greater likelihood of poor recovery, whereas SVO was associated with more favorable outcomes. This pattern has been observed previously, with lacunar infarctions generally having smaller infarct volumes and better neurological functional recovery than atherosclerotic and cardioembolic strokes [22]. In addition to CE, patients with LAA exhibited the highest mean HbA1c levels and were associated with poor functional recovery. This indicates that patients with a high atherosclerotic vascular risk are not optimally managed for glycemic control. Inadequate management of factors that could substantially worsen outcomes is worrisome and requires the strict implementation of measures to improve outcomes.
Elevated HbA1c levels at admission were significantly associated with poor FOC in the overall AIS population, and this relationship persisted after adjusting for demographic, clinical, and stroke severity variables. When stratified by the TOAST subtype, HbA1c levels remained independently predictive of poor FOC in the SVO, LAA, and CE subtypes. Using ROC analysis, we identified an HbA1c cut-off of 6.8% that optimally discriminated between good and poor FOC. Patients with HbA1c levels ≥ 6.8% had significantly higher odds of residual functional disability at 90 days, even after adjusting for stroke subtype and other confounders. Similar associations between CH and poor post-stroke recovery have been reported in prior studies [10,11, 23,24,25,26]. A recent study from SA also observed a significant increase in stroke severity for HbA1c levels exceeding 6.5%, and HbA1c levels < 6.5% were associated with not only less severe strokes but also lower mortality [6]. Cao et al. also reported a lower risk of poor 3-month FOC in diabetic patients with AIS, with HbA1c values closer to 6.1%; however, the association was nonlinear [14]. Some studies have suggested that the prognostic effect of HbA1c may vary with age or differ between diabetic and non-diabetic groups, highlighting population-specific influences and supporting the need for context-sensitive clinical interpretations.
In our study, the discriminatory ability of the model of HbA1c alone for poor FOC (AUC = 0.604) indicated modest predictive performance, which limited the clinical applicability of HbA1c as a standalone prognostic marker. Although this effect was statistically significant, it may become more evident with a larger sample size or greater study power. SVO was the subtype in our cohort that demonstrated the strongest association between HbA1c and FOC among the TOAST subtypes in the ROC curve analysis. SVO was also the only subtype in a study by Jeong et al., in which elevated HbA1c demonstrated a significant association with poor functional recovery among young adults [13]. In our study, the effect on CE subtype was not independent of age. The varied responses among different TOAST subtypes can be explained by differences in age groups, prevalence of risk factors, and extent of infarction.
Several biological mechanisms may explain the effects of CH on stroke outcomes. Elevated HbA1c is associated with endothelial dysfunction, impaired collateral circulation, increased oxidative stress, pro-thrombotic activity, and impaired neuronal survival responses [27,28,29]. These mechanisms may contribute to increased infarct growth, worsened reperfusion dynamics, and reduced neural recovery potential in patients with high HbA1c levels. The European American Stroke Guidelines suggest maintaining HbA1c levels below 7% in patients with AIS while addressing age and other patient-related factors [30]. Recently, the authors performed a secondary analysis of the RESCUE BT trial and found that an HbA1c > 6.5% was significantly associated with worse FOC in patients with LVO who underwent EVT [9]. They established a significant association between glycated hemoglobin (HbA1c), which was assessed as a continuous variable, and patient outcomes. Our study demonstrated a similar relationship between HbA1c and outcomes; however, the study population was different, as we studied all patients with AIS and not only those with LVO who underwent EVT. However, based on our findings, we suggest conducting such studies in this region to provide evidence for the effect of CH on therapeutic and functional outcomes in patients undergoing EVT for LVO. This will enhance knowledge and help management by providing scientific data.
We identified HbA1c > 6.8% to be significantly associated with poor functional recovery in the studied population and emphasized that physicians should follow the recommendations in the guidelines for HbA1c values in patients with AIS [30]. Furthermore, there is a need to further investigate the targets to be achieved for each of the major TOAST subtypes – SVO, LAA, and CE – by conducting further multicenter studies with large sample sizes. When discussing disorders with a high chance of significant disability, preventive strategies are the cornerstone for reducing the disease burden, and every single step carries a high value. Higher HbA1c levels (both as continuous and categorical increments) have been associated with an increased risk of first-ever AIS in both non-diabetic and diabetic populations [1]; therefore, screening and regular monitoring of HbA1c levels should be practiced by physicians to prevent AIS. Importantly, stroke cases per 100,000 people in the KSA increased by 11.4% between 1990 and 2021, and if proactive preventive strategies are not implemented, it may rise further [31, 32]. Self-awareness of treatment, monitoring tests indicating adequate glycemic control, and a healthy lifestyle are pivotal in preventing disease-related complications among high-risk patients. A multicenter Saudi Arabian study has shown a positive effect of educating patients about glycated hemoglobin, including the level and target goal on glycemic control [33], and such strategies, if practiced by every physician, can make a difference in health management.
Our study has some limitations. First, this was a single-center study, which may have affected the generalizability of our observations. Second, we evaluated the effect of HbA1c as a marker of chronic glycemic exposure independent of the diagnostic labeling of diabetes mellitus. Third, data regarding pre-admission glycemic control and medication adherence were not consistently available in the medical records and therefore could not be incorporated into the analysis. Fourth, we acknowledge that the HbA1c ≥ 6.8% threshold in our study is data-driven, that need further external validation and cannot be considered as a definitive clinical cut-off. Finally, the observational design precluded conclusions regarding causality.
Despite these limitations, we presented data on HbA1c levels assessed as a continuous and categorical variables and stroke FOC according to TOAST subtypes, which show evidence that CH is a statistically significant modifiable predictor of poor functional recovery in AIS. Our findings align with a large multicenter Japanese study by Kamouchi et al., which reported unfavorable outcomes in AIS patients with HbA1c > 6.8% [10]. The identified HbA1c value of <6.8% in our study cohort was less than 7%, which is the value mentioned in the guidelines to be achieved [30] and shows the pertinent clinical relevance of the data. Furthermore, it is in accordance with published studies from different regions of the world, and therefore has epidemiological relevance [6, 9, 14, 10, 13]. However, as the incremental predictive value of HbA1c beyond established clinical predictors (like NIHSS, age, and etiologic subtypes) in our study is modest, we recommend considering HbA1c more as a risk modifier rather than a standalone prognostic tool. Overall, the results of our study suggest that HbA1c, which reflects the underlying metabolic risk and chronic glycemic burden, has a limited utility as a standalone prognostic biomarker, and therefore should not be considered as an individual prognostic factor for FOC in patients with AIS. Rather, it has an important role in refining risk stratification when used in conjunction with established clinical predictors such as stroke severity, TOAST subtype, and vascular risk factors. Moreover, the determination of the definite optimal cut-off value for HbA1c threshold needs further verification, as it varies in many published research studies, including ours. The important consideration is that, though it is not uniform, it is less than 7.0 in most of the studies, strengthening and emphasizing the crucial importance of following the recommendations by guidelines [30].
Higher HbA1c levels at admission were associated with a poor 3-month FOC in patients with AIS. An HbA1c threshold of ≥6.8% was identified as a predictor of unfavorable functional recovery. Our findings indicate that CH has a role in risk stratification predicting stroke prognosis in patients with major TOAST subtypes when used with other well-established predictors, and highlight the need for optimized long-term glycemic control and closer post-stroke monitoring in high-risk individuals.