
Chronic Myeloid Leukemia (CML) is a type of hematologic malignancy characterized by the uncontrolled expansion of myelopoietic cells due to the presence of the Breakpoint Cluster Region-Abelson oncogene Locus (BCR-ABL) (Valentina R. et al., 2021). CML is defined by a reciprocal translocation between chromosomes 9 and 22, which results in the formation of the Philadelphia chromosome (Ph). This translocation leads to the creation of the BCR-ABL fusion gene, a hallmark molecular marker of this disease [1].
The clinical progression of CML is categorized into three phases: chronic phase, accelerated phase, and blast phase [2]. Epidemiologically, CML accounts for approximately 20% of all leukemia cases in adults, with an annual incidence of 1.5 cases per 100,000 people. The incidence of CML is higher in men than women, with a male-to-female ratio ranging from 1.2 to 1.7. Although the incidence of CML generally increases with age, the majority of CML patients in Indonesia tend to be younger [3].
In the last two decades, significant advancements have been made in the treatment of CML, primarily with the introduction of Tyrosine Kinase Inhibitors (TKIs) that specifically target the BCR-ABL1 protein. These therapies have proven to be both effective and safe, leading to substantial improvements in prognosis. The use of TKI has increased patient survival from 20% to 80–90%, with therapy targeting the BCR-ABL pathway to stop cell proliferation. TKIs are classified into three generations: first-generation (imatinib), second-generation (nilotinib, dasatinib, and bosutinib), and third-generation (ponatinib) [4].
Despite the remarkable efficacy of TKIs in treating CML, prolonged use can lead to side effects, including cardiovascular toxicity. Cardiovascular complications associated with TKI therapy include congestive heart failure, ischemic heart disease, hypertension, and endothelial dysfunction [2,5]. Hypertension is one of the most commonly reported side effects in patients receiving TKI therapy. In a study involving 531 CML patients treated with various TKIs, hypertension occurred in 33% of patients, with 15% experiencing new-onset hypertension and 18% having worsened hypertension [6].
The increase in blood pressure among CML patients treated with TKIs is believed to be caused by the inhibition of the Vascular Endothelial Growth Factor (VEGF) pathway. This inhibition reduces the bioavailability of Nitric Oxide (NO) and increases the production of endothelin-1, leading to increased vascular resistance and decreased vascular density. Additionally, TKIs have pro-atherogenic and anti-angiogenic effects on endothelial cells, contributing to the increased risk of hypertension [7,8,9]. Uncontrolled hypertension can exacerbate morbidity and mortality in these patients, as well as increase the risk of thromboembolic events and other cardiovascular complications.
Given this context, the aim of this study is to evaluate changes in blood pressure in CML patients receiving TKI therapy, with a focus on comparing the effects of first-generation (imatinib) and second-generation (nilotinib) TKIs, and to assess the long-term cardiovascular impact of these treatments.
This retrospective cohort analysis was conducted at Wahidin Sudirohusodo Hospital and its associated institutions. Data were obtained from the electronic medical records of adult patients diagnosed with CML who commenced therapy with a tyrosine kinase inhibitor TKI, namely imatinib or nilotinib, between January 2025 and January 2026. The baseline was defined as the date of TKI initiation. Blood pressure readings were subsequently recorded at 3, 6, 9, and 12 months after the commencement of medication. The analysis included only those patients for whom complete 12-month follow-up data were available.
The study included adult patients (≥18 years) diagnosed with CML in the chronic phase, who were undergoing treatment with either imatinib or nilotinib for at least 12 months. Exclusion criteria were as follows: patients with pre-existing hypertension, significant cardiovascular conditions (such as congestive heart failure or ischemic heart disease), or advanced chronic kidney disease (eGFR <30 mL/min).
Patient data were extracted from the hospital's medical records system. Information gathered included:
Demographics: Age and gender
CML Treatment History: Type of TKI used (imatinib or nilotinib), treatment duration
Comorbidities: Presence of diabetes, dyslipidemia, hypertension, ischemic heart disease, congestive heart failure, chronic kidney disease, and obesity
Blood Pressure Measurements: Recorded systolic and diastolic blood pressure values before TKI therapy and at 3, 6, 9, and 12 months of follow-up.
Blood pressure measurements were retrospectively collected from the electronic medical records of patients treated at the Hematology–Medical Oncology outpatient clinic. Trained healthcare personnel used a validated automated oscillometric sphygmomanometer (Omron HEM-7130, Omron Healthcare Co., Ltd., Kyoto, Japan) following American Heart Association guidelines. Patients were instructed to refrain from smoking, consuming caffeine, and engaging in physical activity for at least 30 minutes prior to measurement. They were also asked to empty their bladder and rest quietly in a seated position for at least 5 minutes. Measurements were taken with the patient seated, back supported, feet flat on the floor and uncrossed, and the arm at heart level. A properly sized cuff was applied to the bare upper arm. Blood pressure was measured twice, with a 1–2 minute interval between readings, and the final value was the average of at least two measurements obtained during the same visit. Antihypertensive therapy was recommended and initiated at the first occurrence of blood pressure exceeding the ACC/AHA 2025 hypertension threshold (SBP ≥130 mmHg or DBP ≥80 mmHg) [10]. Patients receiving corticosteroids or NSAIDs were excluded from the study. Data on TKI dose and adherence were inconsistently recorded and therefore not included in the analysis.
This study aimed to measure changes in systolic and diastolic blood pressure from the beginning of the study to twelve months after starting TKI treatment. Secondary goals included:
The pattern of blood pressure changes during the twelve-month follow-up.
The emergence of new hypertension, as defined by the 2025 ACC/AHA guidelines, is defined by a systolic blood pressure (SBP) of 130 mmHg or higher, and/or a diastolic blood pressure (DBP) of 80 mmHg or higher [10]. The proportion of patients who started antihypertensive treatment during the follow-up period, including when they began treatment, is presented.
Statistical analysis was performed using SPSS version 25.0 (IBM, USA) and R version 4.3.2 for mixed-effects modelling. Continuous variables were assessed for normality using the Shapiro-Wilk test and summarized as median [range] as appropriate.
Changes in systolic and diastolic blood pressure over the 12-month follow-up (baseline, 3, 6, 9, and 12 months) were analyzed using a linear mixed-effects model, which included fixed effects for time, treatment group (Imatinib vs Nilotinib), and the time × group interaction, and random intercepts for individual patients to account for repeated measurements. The model was adjusted for baseline BP and prespecified covariates: age, sex, smoking status, diabetes mellitus, and dyslipidemia.
Between-group comparisons at 12 months were derived from the mixed-effects model, providing adjusted mean differences with 95% confidence intervals (CI). For categorical outcomes, such as the incidence of hypertension (≥130/80 mmHg, ACC/AHA 2025), risk ratios (RR) with 95% CI were calculated. Statistical significance was set at p < 0.05.
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Biomedical Research Ethics Committee at the Faculty of Medicine, Hasanuddin University (Approval number: 1223/UN4.6.4.5.31/PP36/2025). Informed consent was obtained from all participants prior to inclusion in the study. Patient data were anonymized for analysis to ensure confidentiality and privacy.
A total of 148 patients diagnosed with CML participated in the study. The gender distribution was nearly equal, with 77 male patients (52%) and 71 female patients (48%). Most patients were under 50 years of age, comprising 101 patients (68.2%), while 47 patients (31.8%) were 50 years or older. The majority of patients were non-smokers, accounting for 130 patients (87.8%), while 18 patients (12.2%) reported smoking. Regarding comorbidities, diabetes mellitus was present in 7 patients (4.7%), and dyslipidemia in 5 patients (3.4%). The two TKI therapies, imatinib and nilotinib, were administered to an equal number of patients, with 74 patients (50%) in each group (see Table 1).
Study characteristics
| Variable | Category | N = 148 | % |
|---|---|---|---|
| Gender | Male | 77 | 52 |
| Female | 71 | 48 | |
| Age | <50 years | 101 | 68.2 |
| ≥50 years | 47 | 31.8 | |
| Smoking Status | Yes | 18 | 12.2 |
| No | 130 | 87.8 | |
| Diabetes Mellitus | Yes | 7 | 4.7 |
| No | 141 | 95.3 | |
| Dyslipidemia | Yes | 5 | 3.4 |
| No | 143 | 96.6 | |
| TKI Type | Imatinib | 74 | 50 |
| Nilotinib | 74 | 50 |
Analysis of blood pressure changes before and after TKI therapy showed significant increases in both systolic and diastolic blood pressure for patients in both the imatinib and nilotinib groups throughout the 12-month follow-up period. In the imatinib group, the mean systolic blood pressure (SBP) gradually increased from a baseline of 112 mmHg (90–131) to 125 mmHg (100–134) at the 12-month follow-up, while diastolic blood pressure (DBP) rose from 72 mmHg (79–90) to 81 mmHg (70–97). Similarly, in the nilotinib group, systolic blood pressure increased from 111 mmHg (100–126) at baseline to 130 mmHg (110–146) at the 12-month follow-up, and diastolic blood pressure increased from 70 mmHg (60–83) to 83 mmHg (70–100). These increases were statistically significant for both systolic and diastolic blood pressure in both treatment groups (p < 0.001) (Figures 1 and 2).
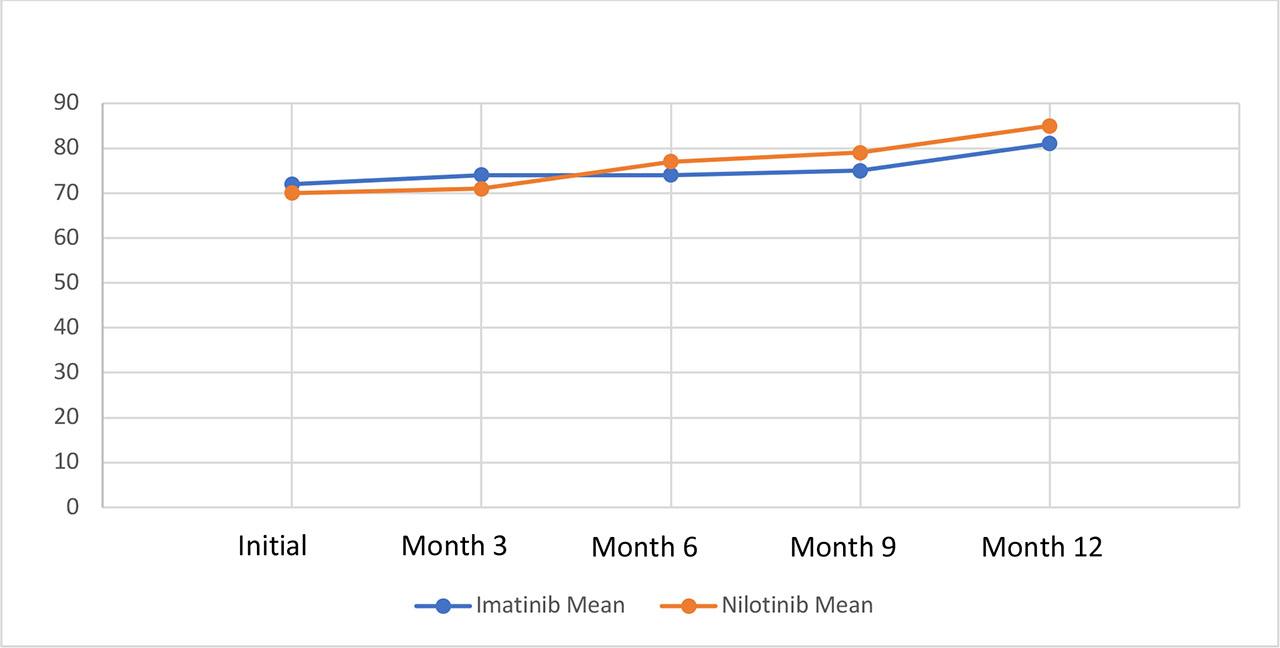
Comparison of systolic blood pressure changes in patients treated with imatinib and nilotinib.
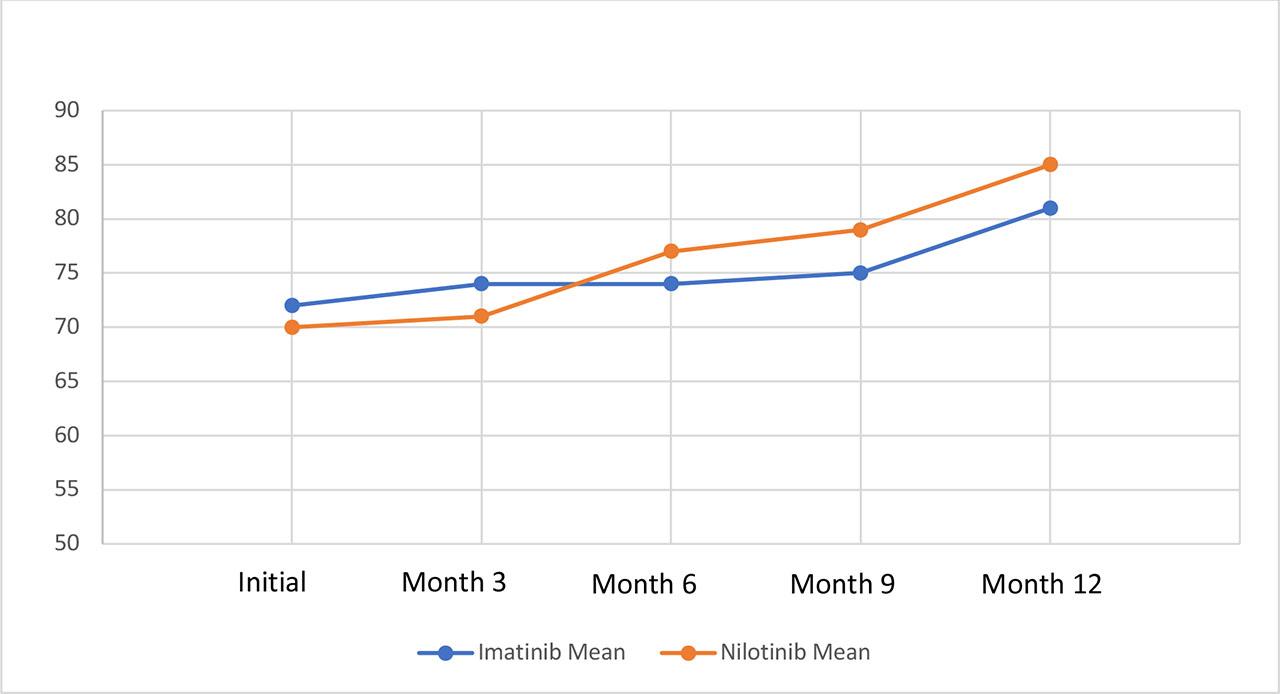
Comparison of diastolic blood pressure changes in patients treated with imatinib and nilotinib.
At baseline, median systolic and diastolic blood pressures were similar between the Imatinib and Nilotinib groups (Table 2). After 12 months, patients receiving Nilotinib had higher blood pressure than those on Imatinib. Median SBP/DBP increased to 130/83 mmHg in the Nilotinib group and 125/81 mmHg in the Imatinib group. Using a linear mixed-effects model adjusted for age, sex, baseline BP, smoking, diabetes, and dyslipidemia, the adjusted mean SBP at 12 months was 132 mmHg (95% CI: 130–134) for Nilotinib and 125 mmHg (95% CI: 123–127) for Imatinib, with a between-group difference of 7 mmHg (95% CI: 4–10; p < 0.001). For DBP, the adjusted mean was 85 mmHg (95% CI: 83–87) for Nilotinib and 81 mmHg (95% CI: 79–83) for Imatinib, with a between-group difference of 4 mmHg (95% CI: 2–6; p = 0.006) (Tables 2 and 3).
Changes in blood pressure before and after TKI therapy
| TKI Type | BP Parameter | Baseline (median [range], mmHg) | 12 Months (median [range], mmHg) | 12-Month Adjusted Mean ± 95% CI (mmHg) | Patients ≥130/80 mmHg at 12 mo n (%)1 | p-value (adjusted)2 |
|---|---|---|---|---|---|---|
| Imatinib | SBP | 112 (90–131) | 125 (100–134) | 125 (123–127) | 28 (37.8%) | <0.001 |
| DBP | 72 (60–90) | 81 (70–97) | 81 (79–83) | 31 (41.9%) | <0.001 | |
| Nilotinib | SBP | 111 (100–126) | 130 (110–146) | 132 (130–134) | 41 (55.4%) | <0.001 |
| DBP | 70 (60–83) | 83 (70–100) | 85 (83–87) | 45 (60.8%) | 0.006 |
Notes:
Patients ≥130/80 mmHg at 12 mo: Number (%) of patients meeting the 2025 ACC/AHA hypertension threshold at the 12-month follow-up.
p-value (adjusted): Derived from the linear mixed-effects model adjusting for age, sex, baseline BP, smoking, diabetes, and dyslipidemia.
Baseline and 12-month BP values are presented as median [minimum–maximum].
12-Month Adjusted Mean ± 95% CI represents the estimated mean from the mixed-effects model, accounting for covariates.
Difference in blood pressure after 12 months of TKI therapy based on drug type
| Blood Pressure | Imatinib Adjusted Mean ± 95% CI | Nilotinib Adjusted Mean ± 95% CI | Between-Group Adjusted Difference ± 95% CI | p-value (adjusted) |
|---|---|---|---|---|
| SBP (mmHg) | 125 (123–127) | 132 (130–134) | 7 (4–10) | <0.001 |
| DBP (mmHg) | 81 (79–83) | 85 (83–87) | 4 (2–6) | 0.006 |
Note: Adjusted for age, sex, baseline BP, smoking, diabetes, and dyslipidemia using a linear mixed-effects model.
Furthermore, a greater proportion of patients receiving Nilotinib met the 2025 ACC/AHA hypertension criteria (SBP ≥130 mmHg or DBP ≥80 mmHg) at 12 months compared with Imatinib: SBP 55.4% vs 37.8% (absolute risk difference: 17.6%) and DBP 60.8% vs 41.9% (absolute risk difference: 18.9%) (Table 2). These findings indicate that Nilotinib therapy is associated with higher blood pressure levels and an increased proportion of patients meeting hypertension criteria relative to Imatinib.
Figure 3 illustrates the difference in adjusted mean systolic blood pressure between the nilotinib and imatinib groups after 12 months of therapy. The nilotinib group showed a higher adjusted mean systolic blood pressure than the imatinib group.
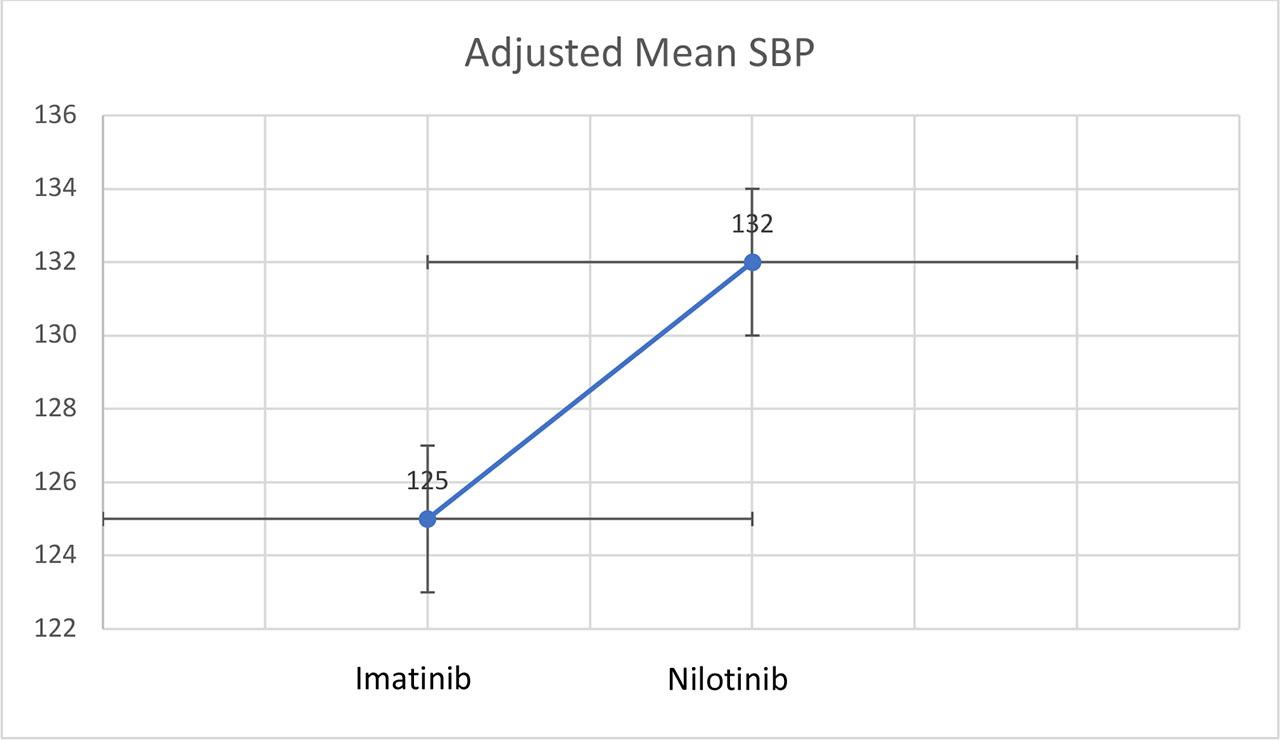
Comparison of blood pressure after 12 months of TKI treatment.
This study involved 148 patients diagnosed with CML who received TKI therapy for at least 12 months. The distribution of gender was relatively balanced, with 77 male patients (52%) and 71 female patients (48%). This finding aligns with the general epidemiology of CML, where the male-to-female ratio typically ranges between 1.3:1 and 1.5:1 [11]. In a large real-world cohort study, it was reported that 56% of CML patients were male. These figures are consistent with global epidemiological data, reflecting the relatively equal gender distribution in our study population [12].
The majority of patients in this cohort were under 50 years of age (68.2%), with only 31.8% being 50 years or older. This age distribution contrasts with global CML epidemiological data, where the highest incidence is typically observed in the fifth to seventh decade of life [13]. However, the inclusion criteria for this study excluded patients with pre-existing hypertension before initiating TKI therapy, a factor that may have contributed to the younger age distribution in our cohort. Hypertension, which often increases with age, could have led to the exclusion of older patients, resulting in a lower proportion of elderly participants in our study. This is further supported by findings who reported that the highest incidence of CML occurs in patients aged 70–74 years, a group which also has a high prevalence of cardiovascular comorbidities such as hypertension and diabetes mellitus [14].
In terms of lifestyle characteristics, only 12.2% of the patients in this study had a history of smoking, whereas 87.8% were non-smokers. This is lower than some real-world reports that found smoking prevalence in CML patients to be between 20% and 30%, particularly among older age groups [6].
Regarding comorbidities, the prevalence in this cohort was low. Diabetes mellitus was present in 4.7% of patients, and dyslipidemia in 3.4%. These figures are substantially lower than those reported in larger real-world studies, where diabetes is found in 10-15% and dyslipidemia in 20-25% of CML patients [12]. The lower prevalence of metabolic comorbidities in our study is likely attributed to the younger age group, as older patients tend to have higher rates of conditions like diabetes and dyslipidemia. The study by Jain et al. in 2018 also noted that CML patients who experienced cardiovascular events during TKI therapy typically had a higher burden of metabolic comorbidities such as diabetes and dyslipidemia [6].
The distribution of TKI therapy was evenly balanced, with 50% of patients receiving imatinib and 50% receiving nilotinib. This balanced distribution was methodologically advantageous, as it allowed for a comparison of blood pressure changes between the two TKI types without bias due to therapy distribution. In real-world clinical practice, older patients and those with more comorbidities tend to be prescribed imatinib, while younger patients with fewer comorbidities are more likely to receive second-generation TKIs like nilotinib [7].
Our investigation reveals that TKI treatment correlates with notable elevations in both systolic and diastolic blood pressure across a 12-month period, with Nilotinib exhibiting a more pronounced impact compared to Imatinib. Employing a linear mixed-effects model, which was adjusted for age, sex, baseline BP, smoking status, diabetes, and dyslipidemia, the adjusted mean SBP at the 12-month mark was 132 mmHg for Nilotinib, contrasted with 125 mmHg for Imatinib; DBP values were 85 mmHg and 81 mmHg, respectively (Table 3). These observations suggest that Nilotinib therapy presents a greater propensity for increased blood pressure, aligning with prior studies that have documented more significant cardiovascular effects associated with second-generation TKIs.
Furthermore, a greater proportion of patients within the Nilotinib cohort met the 2025 ACC/AHA hypertension guidelines (≥130/80 mmHg), thereby highlighting the critical need for prompt intervention and consistent blood pressure assessment throughout TKI treatment. These observations imply that healthcare providers should adopt a more vigilant approach to managing cardiovascular risk factors in individuals receiving Nilotinib, regardless of their prior hypertension history.
These findings are consistent with those who observed a similar increase in both systolic and diastolic blood pressure after TKI therapy compared to pre-treatment levels. Their study also highlighted hypertension as the most common cardiovascular side effect, with an incidence of 33% among patients receiving TKIs, consisting of 15% new-onset hypertension and 18% worsening of pre-existing hypertension [6].
The results align with other studies reporting that second-generation TKIs, like nilotinib, are associated with a higher risk of hypertension and cardiovascular issues compared to imatinib. This difference is attributed to the antiangiogenic and pro-atherogenic effects of nilotinib on vascular endothelial cells, resulting from the inhibition of the VEGF pathway, reduced nitric oxide bioavailability, and activation of the renin-angiotensin system [8]. A study by Agarwal et al. in 2018, further explained that inhibition of the VEGF pathway by TKIs leads to vasoconstriction, which contributes to systemic hypertension [15].
After 12 months of TKI therapy, patients receiving Nilotinib exhibited a significantly greater increase in blood pressure compared with those receiving Imatinib. Based on the linear mixed-effects model adjusted for age, sex, baseline BP, smoking, diabetes, and dyslipidemia, the adjusted mean SBP was 132 mmHg in the Nilotinib group versus 125 mmHg in the Imatinib group, and the adjusted mean DBP was 85 mmHg versus 81 mmHg, respectively (Table 3). These results indicate that Nilotinib therapy is associated with a stronger hypertensive effect than Imatinib, even after controlling for key covariates.
The results are consistent with findings who demonstrated that nilotinib is associated with a higher risk of cardiovascular diseases, including hypertension, compared to imatinib and dasatinib. Their study found that this effect was related to increased levels of total cholesterol and LDL, as well as endothelial dysfunction due to inhibition of the PI3K/AKT-eNOS pathway [16].
Long-term studies such as ENEST1st and ENESTnd have also reported a higher incidence of hypertension in patients treated with nilotinib compared to those receiving imatinib, with rates of 10.4% for nilotinib versus 8.3% for imatinib [17]. This supports the observation that second-generation TKIs may have a more pronounced hypertensive effect.
In the present study, although significant increases in blood pressure were observed, not all patients exceeded the 2025 ACC/AHA hypertension threshold (≥130/80 mmHg) at 12 months. This discrepancy may reflect several factors, including the relatively short follow-up period and the younger patient population with fewer baseline cardiovascular comorbidities. In clinical practice, early interventions such as lifestyle modification or initiation of antihypertensive therapy may help attenuate the progression of TKI-associated blood pressure increases, potentially reducing the proportion of patients who develop overt hypertension.
This study has several limitations. First, as a retrospective observational study, data were abstracted from routine clinical care across multiple providers and sites, which may introduce information bias. Although blood pressure measurements were generally standardized, not all aspects of the protocol could be verified, including rest period, abstinence from caffeine or smoking, bladder emptying, patient positioning, cuff size, and number of readings, introducing potential measurement error and inter-operator variability.
Second, treatment allocation may have been influenced by clinicians’ assessment of baseline cardiovascular risk, resulting in confounding by indication. The linear mixed-effects model adjusted for age, sex, baseline BP, smoking status, diabetes, and dyslipidemia, but residual confounding from unmeasured variables cannot be excluded.
Third, exact dates when patients first exceeded the ACC/AHA 2025 hypertension threshold were not consistently recorded, preventing time-to-event analyses such as Kaplan-Meier curves or Cox proportional hazards modelling. As a result, we cannot determine whether Nilotinib-treated patients developed hypertension earlier than those receiving Imatinib, although the higher proportion meeting hypertension criteria at 12 months suggests a clinically meaningful difference. Fourth, this was a single-center study with predominantly younger patients and few comorbidities, partly due to exclusion of pre-existing hypertension, which may limit generalizability to older, higher-risk CML populations. Further studies in broader cohorts are warranted to validate these findings.
Fifth, BMI data were not collected for this study. Consequently, BMI could not be incorporated into adjusted analyses, and its potential impact on blood pressure variability could not be assessed.Finally, the 12-month follow-up may be insufficient to capture long-term cardiovascular effects of TKI therapy. Despite these limitations, the study provides valuable insight into the longitudinal blood pressure changes associated with Imatinib and Nilotinib in a real-world cohort.
This study highlights significant increases in blood pressure in CML patients undergoing treatment with either imatinib or nilotinib over 12 months, with nilotinib showing a stronger association with elevated blood pressure. The findings underline the cardiovascular risks tied to long-term TKI therapy, particularly with second-generation TKIs like nilotinib, which may induce endothelial dysfunction and vascular resistance. While the blood pressure changes observed were significant, not all patients met the clinical criteria for hypertension, suggesting that early detection and intervention may help prevent more severe cardiovascular issues. Given the retrospective nature and relatively short follow-up of this study, further research with longer follow-up periods is needed to fully understand the long-term effects of TKI therapy on cardiovascular health, providing better insights for patient management strategies.