
Dermatomyositis is an idiopathic autoimmune connective tissue disease marked by characteristic cutaneous findings and variable skeletal muscle involvement, typically manifesting as proximal muscle weakness [1]. Anti–Melanoma Differentiation–Associated Gene 5 (MDA-5) dermatomyositis (MDA5-DM) is a rare systemic autoimmune disease that was initially described in Japanese patients, typically presenting with clinically amyopathic dermatomyositis (CADM) and rapidly progressive interstitial lung disease (ILD) [2]. MDA5-DM is characterized by typical dermatomyositis-related cutaneous manifestations, polyarthralgia and ILD; however, clinical features of myositis are usually absent in these patients [3]. MDA-5 was first identified in 2002 and is currently recognized as a key protein involved in the regulation of the antiviral immune response [4]. A 40-year-old woman with a known diagnosis of dermatomyositis presented to the emergency department with progressive dyspnea, cough, and fever. On systemic examination, her blood pressure was 132/74 mmHg, pulse rate was 96 beats per minute, respiratory rate was 22 breaths per minute and body temperature was 38.6°C. The patient exhibited symmetrical, erythematous, and scaly plaques on the extensor surfaces of the elbows. These lesions were consistent with Gottron’s sign, which is characteristic of dermatomyositis (see figure 1a). Erythematous, scaly lesions were also observed on the dorsal hands and finger joints. These findings are typical of Gottron’s papules and indicate the cutaneous involvement of dermatomyositis (see figure 1b).

The patient exhibited symmetrical, erythematous, and scaly plaques on the extensor surfaces of the elbows. These lesions were consistent with Gottron’s sign, which is characteristic of dermatomyositis.

Erythematous, scaly lesions were also observed on the dorsal hands and finger joints. These findings are typical of Gottron’s papules and demonstrate the cutaneous involvement of dermatomyositis.
Autoantibody testing revealed negative antinuclear antibodies, while the extractable nuclear antigen profile showed anti-histone antibody positivity (2+; reference range 0–4+) and a positive anti–MDA-5 antibody. The patient had been receiving mycophenolate mofetil (2×1000 mg/day) and methylprednisolone (4 mg/day) for dermatomyositis. Due to a decline in oxygen saturation to 75% on room air, she was admitted to the intensive care unit (ICU). On admission, laboratory evaluation demonstrated elevated inflammatory markers (C-reactive protein (CRP) 32 mg/L; erythrocyte sedimentation rate (ESR) 24 mm/h, normal total leukocyte count (6.7×103/µL) with marked lymphopenia (0.4×103/µL), neutrophil count of 5.84×103/µL, elevated lactate dehydrogenase (594 IU/L) and mildly increased creatine kinase levels (390 U/L). Severe lymphopenia was considered a poor prognostic indicator strongly associated with rapidly progressive interstitial lung disease (RP-ILD) in anti-MDA5–positive dermatomyositis. Given the presence of fever and elevated acute-phase reactants, infectious triggers were prioritized in the differential diagnosis, and blood and urine cultures along with a respiratory polymerase chain reaction (PCR) panel were obtained. Abdominal computed tomography (CT) revealed no infectious focus. Chest CT demonstrated extensive bilateral involvement, predominantly in the basal and peripheral lung regions, characterized by reticular opacities, traction bronchiectasis, and cystic changes consistent with honeycombing. Compared with a CT scan performed 10 days earlier at an external center, marked radiological progression was evident (see figure 2a and 2b), consistent with the aggressive course of anti-MDA5–associated RP-ILD. Empirical antimicrobial therapy with levofloxacin (750 mg/day) and ceftriaxone (2×1000 mg/day) was initiated. However, given the strong suspicion of immune-mediated lung injury, mycophenolate mofetil was discontinued and intravenous immunoglobulin (IVIG) was commenced at a dose of 0.4 g/kg/day for five consecutive days. Despite treatment, inflammatory markers continued to rise (CRP 170 mg/L; ESR 94 mm/h), prompting escalation to broad-spectrum antibiotics with piperacillin–tazobactam (4×4.5 g/day). The patient’s respiratory status rapidly deteriorated, with increasing tachypnea and oxygen requirements, necessitating endotracheal intubation on the third day of ICU admission and IVIG therapy. The respiratory PCR panel was negative for common viral and bacterial pathogens. However, serum cytomegalovirus (CMV) PCR was positive at 357 IU/mL (negative <200 IU/mL; low-level positivity 200–1000 IU/mL).
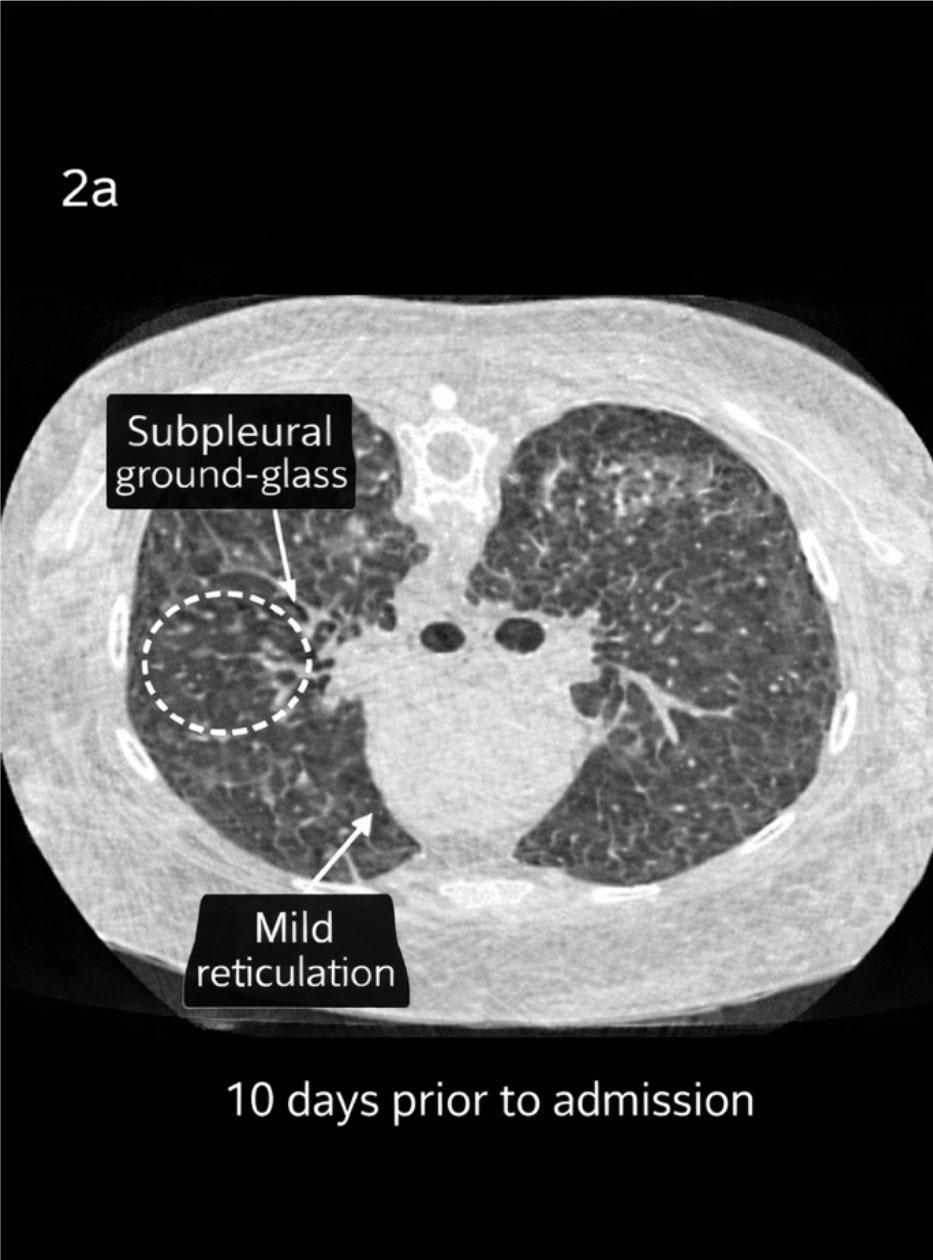
Diffuse but relatively mild involvement is observed in both lungs. Predominantly subpleural and peripheral ground-glass opacities are present, with focal fine reticular changes. Prominent honeycombing or advanced fibrotic changes are limited in this section. Overall, this appearance is consistent with early to intermediate-stage interstitial lung disease.
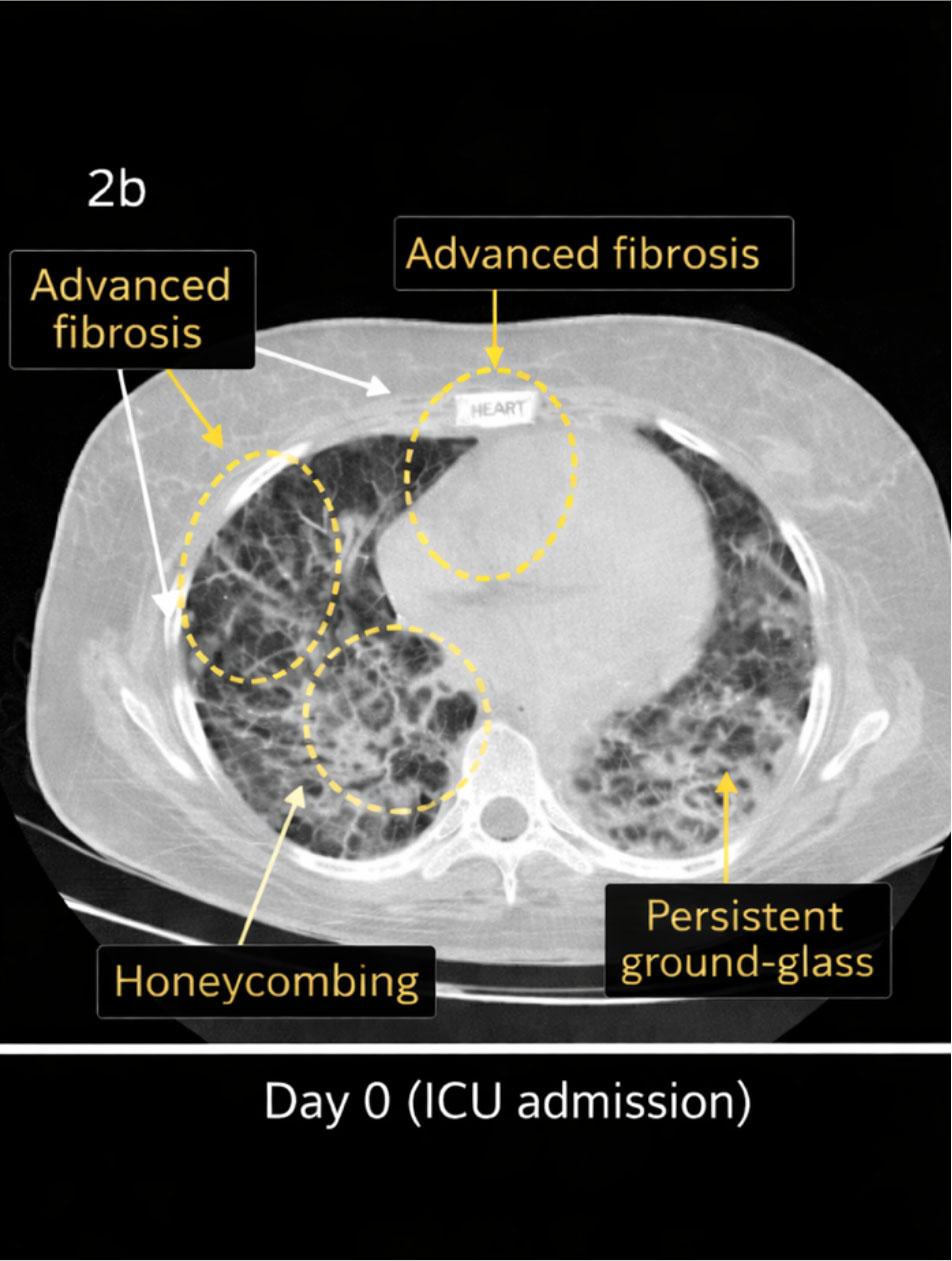
Marked progression is evident, particularly in the basal and subpleural regions. Diffuse reticular opacities, traction bronchiectasis, and cystic changes consistent with honeycombing have developed in certain areas. Ground-glass opacities persist but are accompanied by predominant fibrotic changes. Collectively, these findings reflect advanced fibrotic transformation developing over a short time interval.
Bronchoalveolar lavage could not be performed due to severe hypoxemia (PaO2 < 60 mmHg and SpO2 < 90%) and hemodynamic instability, characterized by hypotension (blood pressure < 90/60 mmHg) and marked tachycardia (heart rate > 160 beats/min). In the absence of definitive evidence demonstrating a direct pathogenic role, the low-level positive CMV viremia detected in this case was interpreted as an associated finding likely related to profound immunosuppression and systemic inflammation rather than the primary cause of pulmonary involvement. Accordingly, CMV reactivation may be considered a potential confounding factor that could have influenced the clinical course, rather than a confirmed mechanistic contributor. During follow-up, the patient developed hemodynamic instability with hypotension and tachycardia, followed by acute kidney injury with an estimated glomerular filtration rate below 15 mL/min. Despite maximal supportive care and immunomodulatory treatment, she succumbed on the fifth day of ICU hospitalization due to refractory respiratory failure secondary to anti-MDA5–associated RP-ILD, with concomitant CMV reactivation and multiorgan failure. The patient’s clinical course is summarized in Table 1. Given the rapid progression of respiratory failure and the high mortality associated with anti-MDA5–related rapidly progressive interstitial lung disease (RP-ILD) reported in the literature, early escalation of immunomodulatory therapy was prioritized. At ICU admission, mycophenolate mofetil was discontinued due to its potential to increase infection risk and its relatively delayed onset of action in controlling acute fulminant inflammatory lung injury.
Timeline of clinical course
| Time point | Clinical events / Findings | Investigations | Treatment | Outcome |
|---|---|---|---|---|
| Day 0 (ICU admission) | Progressive dyspnea, fever, hypoxemia (SpO2 75% RA) | Labs: CRP 32 mg/L, ESR 24 mm/h, severe lymphopenia (0.4×103/µL); Chest CT: rapidly progressive bilateral fibrotic ILD | Oxygen therapy; empirical levofloxacin + ceftriaxone; MMF discontinued; IVIG (0.4 g/kg/day) initiated | Respiratory distress persisted |
| Day 1 | Persistent fever and worsening inflammation | Rising inflammatory markers | Continued IVIG + antibiotics | Clinical deterioration |
| Day 2 | Increasing tachypnea and oxygen requirement | CRP 170 mg/L, ESR 94 mm/h; respiratory PCR negative; CMV PCR: low-level viremia (357 IU/mL) | Antibiotics escalated to piperacillin–tazobactam | Progressive hypoxemia |
| Day 3 | Acute respiratory failure | Severe hypoxemia; BAL deferred due to PaO2 < 60 mmHg, SpO2 < 90%, hypotension and tachycardia | Endotracheal intubation and mechanical ventilation | Temporary stabilization |
| Day 4–5 | Hemodynamic instability and multiorgan dysfunction | Hypotension, tachycardia, acute kidney injury (eGFR < 15 mL/min) | Maximal supportive care and immunomodulatory therapy | Death due to refractory respiratory failure secondary to anti-MDA5–associated RP-ILD |
Intravenous immunoglobulin (IVIG) was selected as the first-line immunomodulatory therapy because of its rapid immunoregulatory effects, relatively favorable safety profile in critically ill patients, and lower risk of infection compared with cytotoxic immunosuppressive agents. Other therapeutic escalation options, including high-dose pulse corticosteroids, calcineurin inhibitors (tacrolimus or cyclosporine), cyclophosphamide, rituximab, and Janus kinase inhibitors, were also considered in accordance with recommended approaches for anti-MDA5–associated RP-ILD. However, these treatments were not administered because the patient’s marked lymphopenia, persistent fever, and the possibility of active infection were considered to confer a substantially increased risk of serious opportunistic infections.
Therefore, a more balanced immunomodulatory strategy was adopted rather than aggressive immunosuppression. Overall, treatment decisions were guided by a risk–benefit assessment aimed at rapidly controlling immune-mediated lung injury while minimizing infectious complications in this critically ill and immunocompromised patient. This case highlights the intrinsically fulminant and frequently fatal nature of anti-MDA5–associated RP-ILD. The rapidly progressive fibrotic lung involvement reflects the aggressive biological behavior of the disease, while concomitant lymphopenia and CMV reactivation are better interpreted as associated findings that may act as synergistic amplifiers of immune-mediated lung injury rather than primary etiologic or mechanistic drivers. Anti-MDA5 positivity should therefore be regarded as a high-risk biomarker conferring substantial mortality, underscoring the critical need for early risk stratification, prompt initiation of immunomodulatory therapy and vigilant monitoring for opportunistic viral reactivation in this vulnerable patient population.