The association between autoimmune rheumatic diseases and cardiovascular diseases, which increased morbimortality, has been widely acknowledged [1,2]. Cardiovascular involvement might have manifested as asymptomatic and mild, but, in certain cases, it could have progressed to a serious and potentially life-threatening condition [3]. European League Against Rheumatism (EULAR) proposed recommendations for management of cardiovascular disease (CVD) risk in patients with rheumatic diseases [Rheumatoid Arthritis (RA), AS, or PsA] since 2016, including an initial CVD risk assessment followed by a 5-year CVD risk assessment [4]. A meta-analysis study showed that SpA was associated with significantly increased risks of CVD including myocardial infarction (MI) and stroke compared to general population [5]. Patients with axSpA also had higher mortality rates, as a result of being frequently comorbid with CVD, which was the most common cause of death after malignant diseases [6].
Developed in 1995 by Tei et al., Myocardial performance index (MPI) or “Tei Index” was a ratio that could be easily assessed using Doppler echocardiography, generated from systolic and diastolic time intervals [7]. The isovolumetric contraction times (ICT) and isovolumetric relaxation times (IRT) were summed together and divided by the total ejection time (ET) yield this ratio. It has been well validated and acknowledged for its ability to efficiently evaluate the myocardium’s overall global function [8]. Compared to commonly used methods such as Ejection Fraction (EF), MPI was a simpler, more powerful and more reliable tool, considerably easier to obtained due to its independence from the delineation of the endocardial border [8,9,10,11]. This index was previously used for the assessment of left ventricular performance in patients with cardiac amyloidosis, coronary artery disease, dilated cardiomyopathy, and congestive heart failure [7,12,13,14,15].
Previous guidelines from American Society of Echocardiography and European Association of Cardiovascular Imaging for the echocardiographic evaluation of left ventricular function recommended a comprehensive, multiparametric approach [16,17]. This included two-dimensional (2D) and, preferably, three-dimensional (3D) assessments of left ventricular ejection fraction (LVEF), global longitudinal strain (GLS), tissue Doppler imaging (TDI), transmitral flow velocities, left atrial (LA) volume, and tricuspid regurgitation (TR) velocity for diastolic function assessment. MPI was not emphasized in these guidelines, not due to its novelty, but likely because its clinical utility had been largely been eclipsed by more accurate and reproducible measures. In resource-limited settings across Southeast Asia, including Indonesia, advanced echocardiography modalities such as 3D imaging, strain imaging, maybe even tissue Doppler were not widely available. This highlighted the need for a readily accessible parameter, which served as the rational for this review. Utilizing MPI assessment through echocardiography could have enhanced the accessibility, affordability, and availability of cardiac function evaluation for SpA patients. Several studies indicated that MPI might have had a potential role in assessing cardiac function in autoimmune rheumatic disease populations, including SpA patients [18,19,20,21]. MPI provided a good picture when used to differentiate the presence of early cardiovascular disorders in study patients compared to controls. Recent meta-analyses by Romand X. et al., demonstrated that ax-SpA had slight impairment of LVEF and more frequently exhibited LV diastolic dysfunction [22]. Similarly, Bolaji O et al., found a markedly reduced LVEF in AS patients compared to controls [23]. However, no comprehensive systematic review or meta-analysis had yet evaluated the role of MPI specifically in SpA to date. Thus, this study was conducted to assess the utility of MPI in evaluating cardiac function in SpA patients.
The methodology for this systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 statement guideline. The study protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO) under registration number: CRD42024622439.
This study aimed to assess the utility of MPI in assessing LV function in SpA patients.
This systematic review included all observational studies, either cross-sectional, case-control, or cohort studies, from 1995 (Tei index first introduced) up to the 2023 year of publication and written in English. In contrast, studies falling within the scope of in vitro or in silico research; interventional studies, including randomized controlled trials (RCTs), non-RCTs, quasi-experimental studies, or multi-arm trials; as well as those categorized as reviews, case reports, case series, conference abstracts, book chapters, or commentaries/editorials were excluded.
The participants in the preliminary studies were adult patients aged 18 years and older who had been diagnosed with SpA according to the Assessment of SpondyloArthritis International Society (ASAS) criteria, New York criteria, or European Spondyloarthropathy Study Group (ESSG) criteria. All participants underwent echocardiography and were compared with healthy adults to assess MPI. Participants having had a past occurrence of MI or stroke, severe valvular disease, atrial fibrillation, hypertrophic cardiomyopathy, congenital heart conditions, or a history of cardiac procedures, as well as those who were pregnant or breastfeeding were excluded. (Supplementary File 1)
The primary outcome of interest was MPI in SpA. Meanwhile, the secondary outcomes included systolic function, diastolic function, correlation of MPI with disease duration, disease activity, systemic inflammation, and cardiovascular risk factor were assessed qualitatively.
A comprehensive search using MEDLINE, ProQuest, Google Scholar, Scopus and Cochrane Library electronic databases was conducted to gather relevant studies. Three separate authors independently executed this search using our predetermined keywords for Rheumatic Autoimmune Disease and Myocardial Performance Index, with the year of study limited to [1995 (MPI first introduced) – 2023] (Supplementary File 2). The rationale behind using the Rheumatic Autoimmune Disease keywords was the possibility or more than one autoimmune or autoinflammatory disease were discussed in the study. All studies examining the SpA and MPI were included. This article specifically focused on LV MPI in SpA patients as LV MPI was more commonly assessed and LV cardiac dysfunction was more frequently reported than right ventricular (RV) dysfucntion in SpA patients. Consequently, studies that only assessed RV MPI were excluded.
All retrieved studies were exported into Mendeley reference manager software, and then checked for duplication, followed by titles and abstracts screening using Rayyan software. Three authors independently conducted the assessments and studies were excluded when the title and/or abstracts were not appropriate for this review. The selected papers underwent full-text assessment using the aforementioned eligibility criteria. Reasons for exclusion were documented within the program, and the reference lists of included studies were manually screened for additional eligible studies. The study selected for the review was determined by majority agreement.
The following data of included studies were extracted independently: the name of primary author, country of origin, study design, sample sizes, age and gender of participants, disease duration, disease activity, echocardiography method, and the outcome of interest. The three independent authors extracted data from all eligible studies. The same authors independently assessed the included studies with following parameters: incomplete outcome data and selective outcome reporting.
MPI, systolic function and diastolic function in SpA patients and control, were quantified and reported as mean differences.
Two independent reviewers evaluated each study using the Newcastle-Ottawa Scale (NOS) adapted for cross-sectional, case-control, and cohort studies. The NOS tool comprised three domains: selection process, comparability, and outcome. Based on the degree of bias, each study’s overall quality was categorized into three levels according to the total NOS score: very high risk of bias (0 to 3 points), high risk of bias (4 to 6) and low risk of bias (7 to 9), with higher score indicating better methodological quality. Discrepancies in assessments were resolved by discussion among the whole review team until consensus was achieved.
The confidence in cumulative evidence was assessed using the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) approach. The GRADE system assessed the quality of evidence for each individual outcome by evaluating factors including the risk of bias within-study (methodological quality), directness of evidence, heterogeneity, precision of effect estimates and risk of publication bias. The overall certainty of evidence was classified into high, moderate, low, or very low quality [24].
All continuous outcomes were presented as mean differences (MDs) and 95% Confidence Intervals (CIs) between each group. We used the Review manager (RevMan; Cochrane Collaboration) version 5.4 to synthesize the pooled data, the heterogeneity, and the power of each study. All synthesized data were presented as forest plots. Some studies reported primary outcomes using different evaluation or calculation methods, therefore the meta-analyses were conducted with a random effects model. However, if the I2 value was 0%, the fixed effect model was conducted.
The effect of each trial was plotted by the inverse of its SE in a funnel plot test, which was utilized to investigate any potential publication bias. Heterogeneity across trials was assessed using the I2 statistic. Less than 25% of an I2 value was regarded as subtle, 25% to 50% as low, 51% to 75% as moderate, and more than 75% as high heterogeneity. Sensitivity analyses were conducted to investigate potential source of the observed heterogeneity. P-values below 0.05 were regarded as significant.
The study selection process and results were presented in a flowchart as shown in Figure 1. Initially, 2239 relevant studies were identified through the search strategy. After removing duplicates, 1694 studies were obtained, with 17 studies being extracted following title and abstract screening. Based on the selection criteria, 16 studies were considered for full-text screening. Five studies did not meet the criteria, among which three did not assess LV MPI index, one study assessed right ventricular MPI index, and one wrong population study. Finally, 11 studies were included in the systematic review, with seven that met eligibility criteria for data extraction being used in meta-analysis.
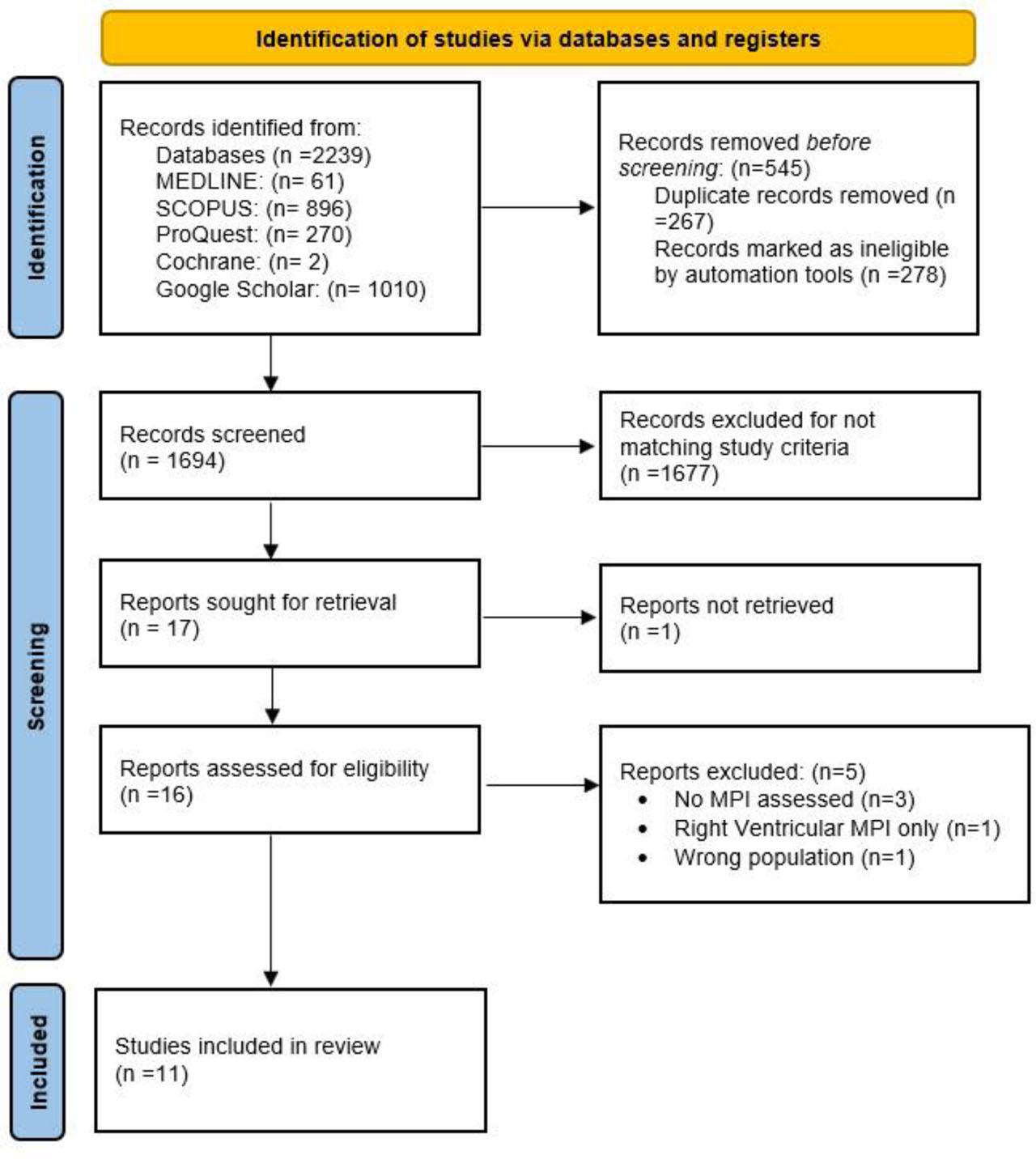
PRISMA 2020 Flow Diagram of Included Studies.
The inclusion criteria were met by a total of 11 studies with one study focusing on uSpA and ten studies focusing on AS. The case group included 544 participants (342 males, 202 females) and the control group comprised 453 participants. The characteristics of the included studies were reported in Table 1.
The included studies comprised two cross-sectional and nine case-control studies. Of the 11 studies included, seven were conducted in Turkey, two in Egypt, one in Greece, and one in Brazil [10,20,21,25,26,27,28,29,30,31,32]. This review encompassed a range of SpA conditions, with one study focusing on uSpA and ten studies on AS with mean ages ranged from 33.79±8.84 to 44.69±9.03 years.
The echocardiography techniques in all studies were performed using transthoracic echocardiography, with six studies using conventional echocardiography, four studies using TDI, and one study by Okan et al., utilized both methods to assess the LV systolic and diastolic function as well as MPI [30]. The systolic indices such as LVEF were reported to be significantly lower in AS compared to healthy control only by two studies. In contrast, the diastolic indices such as E/A ratio [mitral inflow early diastolic wave (E)/late diastolic wave (A)] or Em/Am ratio [early diastolic myocardial peak velocity (Em)/late diastolic myocardial peak velocity (Am)] were reported to be significantly different by four included studies. The remaining of included studies demonstrated no significant difference of diastolic and systolic indices.
The disease duration in each study varied, with the shortest duration being at least one year and the longest duration reported as 30.6±9.5 years; data from two studies were not available. The most frequently used scoring to describe the disease activity of AS was BASDAI with values ranging from 1.24±1.13 to 5.01±7.71. Only two out of eleven included studies assessed the MPI with disease activity and duration. Rosa RE et al., found altered MPI was not associated with disease activity (as measured with BASDAI) (p=1.00) but was associated with disease duration. Patients with more than 20 years of disease had higher rates of concentric ventricular remodeling (p=0.02) and altered MPI (p=0.014) than those with less than 20 years disease duration [11]. Moyssakis I et al. demonstrated significant correlation of LV MPI and disease duration (r=0.549, p<0.001) and BASDAI score (r=0.405, p=0.004), but not with BASFI or BASMI score [26].
Kocabas et al. were the only researches to investigate the relationship between MPI and traditional cardiovascular risk factors such as body mass index (BMI), systolic blood pressure (SBP), and diastolic blood pressure (DBP) in patients with AS [25]. Their findings showed no significant association between these factors and MPI. In contrast, MPI demonstrated a significant correlation with systemic inflammation, particularly erythrocyte sedimentation rate (ESR) and red cell distribution width (RDW), suggesting a stronger link between inflammation and cardiac function in this patient group. Further details were shown in Table 1.
Study Characteristics
| No | Author, Publication Year | Country | Type of study | Echocardiography technique | Participant | Disease Duration (years) | Disease Activity | Outcome of Interest | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Age (years) | ||||||||||
| Case | Control | Case | Control | ||||||||
| uSpA | |||||||||||
| 1 | Albayrak et al., 2013 [27] | Turkey | Cross-sectional study | TTE |
|
| 43.4 ±9.1 | 41.1± 8.9 | N/A | N/A | Conventional Echocardiography
|
| AS | |||||||||||
| 2 | Kucuk et al., 2018 [28] | Turkey | Case-control study | TTE |
|
| 41.0 ± 9.2 | 37.5 ± 10.7 | 8.53 |
| Conventional Echocardiography
|
| 3 | Özmen C et al., 2020 [29] | Turkey | Cross-sectional study | TTE |
|
| 44.0 (36.0–52.0) | 45.0 (29.5–56.5) | At least 1-year | N/A | Conventional Echocardiography
|
| 4 | Nageeb G et al., 2013 [32] | Egypt | Case-control study | TTE |
|
| 43.9±10.2 | N/A | 30.6±9.5 |
| Tissue Doppler Imaging
|
| 5 | Kocabas H et al., 2018 [25] | Turkey | Case-control study | TTE |
|
| 44.69±9.03 | 43.13±8.59 | 19.14±7.51 |
| Conventional Echocardiography
|
| 6 | Rosa RE et al., 2015 [10] | Brazil | Case-control study | TTE |
|
| 38.95 | 35.85 | 16.45 (3–32) |
| Conventional Echocardiography
|
| 7 | Seddik et al., 2023 [21] | Egypt | Case-control study | TTE |
| 45 |
| 36.33±6.43 |
|
| Conventional Echocardiography
|
| 8 | Moyssakis et al., 2009 [26] | Greece | Case-control study | TTE |
|
| 41.78 ± 10.02 | 39.92 ± 9.11 | 14.77 ± 10.07 |
| Conventional Echocardiography
|
| 9 | Okan T et al., 2008 [30] | Turkey | Case-control study | TTE |
|
| 38±11 | 36±9 | N/A |
| Conventional Echocardiography
|
| 10 | Acar G et al., 2009 [20] | Turkey | case-control study | TTE |
|
| 37.82±10.22 | 35.74±9.98 | 69.48±63.85 (months) |
| Conventional Echocardiography
|
| 11 | Kiris A et al., 2012 [31] | Turkey | case-control study | TTE |
|
| 36.4±10 | 39.1±8.2 | 7.6±4.4 |
| Tissue Doppler Imaging
|
AS: Ankylosing Spondylitis, uSpA: undifferentiated Spondyloarthritis, TTE: transthoracic echocardiography, EF= ejection fraction, MPI= myocardial performance, E = peak early diastolic myocardial velocity, A=peak late diastolic myocardial velocity, Em = tissue doppler mitral annular E wave velocity, Am = tissue doppler mitral annular A wave velocity, BASDAI: Bath Ankylosing Spondylitis Disease Activity Index, BASFI: Bath Ankylosing Spondylitis Functional Index, BASMI: Bath Ankylosing Spondylitis Metrology Index, MASES: Maastrich Ankylosing Spondylitis Enthesitis Score, ASQoL: Ankylosing Spondylitis Quality of Life Questionnaire, NS: non significant
Among the eleven studies evaluated using NOS, nine were case-control studies (Table 2.A) and two were cross-sectional studies (Table 2.B). Eight of nine case-control studies were considered as having good quality with one case-control study by Kocabas et al., was considered to be of fair quality [25]. All cross-sectional studies were categorized as having good quality.
Results of Quality Assessment using Newcastle-Ottawa Scale (NOS) adopted for case-control studies.
| No | First Author, Year of Publication, Country | Selection | Comparability | Outcome | Overall Risk of Bias | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S4 | O1 | O2 | O3 | ||||
| 1 | Kucuk et al., 2018, Turkey [28] | * | * | 0 | * | ** | * | * | * | Good quality |
| 2 | Nageeb G et al., 2013, Egypt [32] | * | * | 0 | * | * | * | * | 0 | Good quality |
| 3 | Kocabas H et al, 2018, Turkey [25] | * | 0 | 0 | * | * | * | * | * | Fair quality |
| 4 | Rosa RE et al, 2015, Brazil [10] | * | * | * | * | ** | 0 | * | * | Good quality |
| 5 | Seddik et al., 2023, Egypt [21] | * | * | 0 | * | * | * | * | 0 | Good quality |
| 6 | Moyssakis et al., 2009, Greece [26] | * | * | 0 | * | ** | * | * | 0 | Good quality |
| 7 | Okan T et al., 2008, Turkey [30] | * | * | 0 | * | ** | * | * | 0 | Good quality |
| 8 | Acar G et al., 2009, Turkey [20] | * | * | 0 | * | ** | * | * | * | Good quality |
| 9 | Kiris A et al., 2012 [31] | * | * | * | * | ** | * | * | 0 | Good quality |
Results of Quality Assessment using Newcastle-Ottawa Scale (NOS) adopted for cross-sectional studies.
| No | First Author, Year of Publication, Country | Selection | Comparability | Outcome | Overall Risk of Bias | ||||
|---|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S4 | O1 | O2 | ||||
| 1 | Albayrak et al., 2013, Turkey [27] | 0 | * | ** | ** | ** | ** | * | Good study |
| 2 | Ozmen et al., 2020, Turkey [29] | 0 | 0 | * | ** | ** | ** | * | Good study |
Overall studies were considered to be good quality by NOS for cross sectional and case-control tools, implying that plausible bias was unlikely to significantly influence the results. Only one study (Kocabas et al., 2018) was designated as fair quality study, as shown in Table 2.A. [25]. The heterogeneity was high for Conventional MPI (cMPI), with I2 test results of 87%, while for Tissue Doppler MPI (tdMPI), we found no substantial heterogeneity, with I2 test results of 0%. Together with a different wide range of 95% CI from individual studies, the statistical heterogeneity may have reflected some inconsistencies. Furthermore, effect estimates came from a small number of studies (only five for cMPI and three for tdMPI), thus inferred serious imprecision. However, no serious indirectness or publication bias was observed that could affect the overall results. Due to the paucity of included studies, publication bias was assessed qualitatively, and no unpublished studies were found in the literature search, suggesting that publication bias is unlikely to be a concern in this analysis. Hence, we rated the quality of evidence as moderate, as displayed in Table 3.
GRADE evidence profile.
| Outcome | Number of participants (studies) | Quality Assessment | Summary findings | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Newcastle Ottawa Scale (NOS) | Inconsistency | Indirectness | Imprecision | Publication bias | Overall quality of evidence | MD total | 95% CI (lower, upper) | ||
| Conventional MPI | 230 case 244 control (5 studies) | Not Serious | Seriousa | Not Serious | Seriousb | Not Seriousc | Moderate | 0.05 | (0.01, 0.08) |
| Tissue Doppler MPI | 171 case 93 control (3 studies) | Not Serious | Not Serious | Not Serious | Seriousb | Not Seriousc | Moderate | 0.08 | (0.06, 0.10) |
MPI: Myocardial Performance Index; MD: Mean Difference; CI: Confidence Interval.
The overall heterogeneity was high, with I2 test results of 87% for Conventional MPI. Furthermore, individual studies have a different wide range of CI, and thus reflected its statistical heterogeneity.
Effect estimates come from a small number of studies (only five for Conventional MPI and three for Tissue Doppler MPI).
Publication bias was assessed qualitatively, and no unpublished studies were found in the literature search, thus not affecting the publication bias.
The seven included studies in the quantitative synthesis yielded various results in between group comparisons. Table 4.A summarizes the differences in MPI assessed by conventional echocardiography between SpA and healthy control groups. Most studies consistently reported significantly higher mean of cMPI values in patients with AS compared to healthy control, with the exception of the study by Kucuk et al., 2018, which did not demonstrate a significant difference [28]. Meanwhile, Table 4.B presented findings based on tissue Doppler echocardiography. All included studies showed that AS patients had significantly elevated tdMPI values relative to controls. For patients with uSpA, however, no statistically significant differences in MPI were observed with either echocardiographic method.
Results of Conventional Myocardial Performance Index (cMPI) in Spondyloarthritis (SpA) compared to healthy control.
| No | Author, Year | Conventional Myocardial Performance Index (cMPI) | ||||||
|---|---|---|---|---|---|---|---|---|
| SpA | Control | p-value | ||||||
| Mean | SD | Participants | Mean | SD | Participants | |||
| Undifferentiated Spondyloarthritis (uSpA) | ||||||||
| 1 | Albayrak 2013 [27] | 0.49 | 0.05 | 40 | 0.49 | 0.08 | 40 | 1.0 |
| Ankylosing Spondylitis (AS) | ||||||||
| 1 | Okan 2008 [30] | 0.49 | 0.06 | 49 | 0.41 | 0.04 | 33 | 0.0001 |
| 2 | Moyssakis 2009 [26] | 0.392 | 0.031 | 57 | 0.37 | 0.034 | 78 | 0.0002 |
| 3 | Kocabas 2018 [25] | 0.71 | 0.15 | 35 | 0.57 | 0.18 | 38 | 0.0006 |
| 4 | Kucuk 2018 [28] | 0.54 | 0.1 | 30 | 0.53 | 0.1 | 30 | 0.70 |
| 5 | Ozmen 2020 [29] | 0.41 | 0.11 | 59 | 0.38 | 0.08 | 65 | 0.083 |
Results of Tissue Doppler Myocardial Performance Index (tdMPI) in Spondyloarthritis (SpA) compared to healthy control.
| No | Author, Year | Tissue Doppler Myocardial Performance Index (tdMPI) | ||||||
|---|---|---|---|---|---|---|---|---|
| SpA | Control | p-value | ||||||
| Mean | SD | Participants | Mean | SD | Participants | |||
| Undifferentiated Spondyloarthritis (uSpA) | ||||||||
| 1 | Albayrak 2013 [27] | 0.45 | 0.1 | 40 | 0.44 | 0.07 | 40 | 0.1078 |
| Ankylosing Spondylitis (AS) | ||||||||
| 1 | Okan 2008 [30] | 0.47 | 0.07 | 49 | 0.39 | 0.04 | 33 | 0.0001 |
| 2 | Kiris 2012 [31] | 0.4 | 0.13 | 77 | 0.33 | 0.1 | 40 | 0.0036 |
| 3 | Nageeb 2013 [32] | 0.45 | 0.09 | 45 | 0.36 | 0.07 | 20 | 0.0002 |
The quantitative synthesis results of AS patients for between group comparisons of MPI using conventional echocardiography were shown in Figure 2.A, whereas the results for between group comparisons of MPI using tissue Doppler echocardiography were displayed in Figure 2.B. Based on the results, significant differences of MPI using conventional and tissue Doppler echocardiography in were found in between group comparisons (MD= 0.05, 95% CI: 0.01–0.08, p-value=0.006 and MD=0.08, 95%CI: 0.06–0.10, p value<0.00001, respectively). However, the between group comparisons of MPI outcomes demonstrated high heterogeneity (I2 = 87%) when assessed with conventional echocardiography, while assessments using tissue Doppler echocardiography showed low heterogeneity (I2 = 0%).
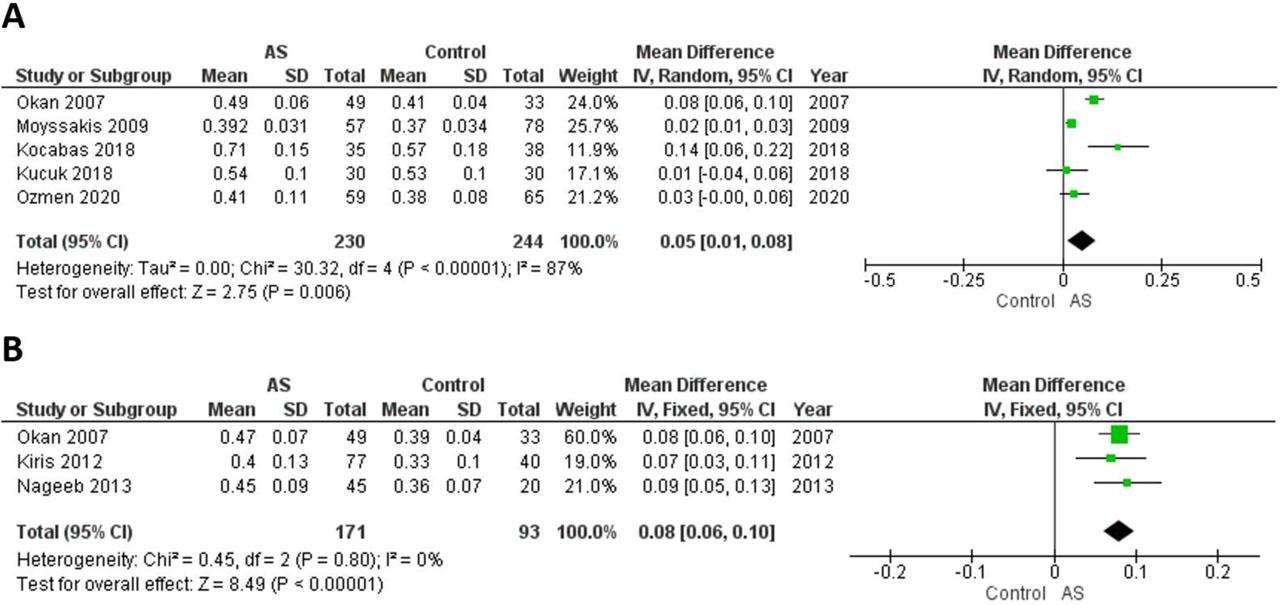
Meta-Analysis Results [Forest Plot] for Myocardial Performance Index in Ankylosing Spondylitis (AS) compared to healthy control; A: Conventional Myocardial Performance Index (cMPI) B: Tissue Doppler Myocardial Performance Index (tdMPI).
This meta-analysis demonstrated a significant increase of cMPI in the AS group compared to healthy controls. Our quantitative analysis results also indicate a notable distinction of tdMPI in AS groups compared to healthy control. All studies showed trends toward elevated tdMPI values in AS groups. The altered cMPI and tdMPI observed in this meta-analysis might have potential for prognostic value in SpA patients as higher MPI value indicates poorer cardiac function, while a lower MPI value indicates better cardiac function. A systematic review by Bennet S et al., have shown that MPI might be an important prognostic marker in acute myocardial infarction (AMI) as significant association with episodes of heart failure, reinfarction, death and left ventricular thrombus formation were found in 14 out of 16 studies [8]. In heart failure patients, MPI value >0.47 indicated heart failure with 86% sensitivity and 82% specificity, and levels of MPI value >0.77 increased 1-, 3-, and 5-year mortality [33].
Some inflammatory pathways could contribute to the development of ventricular dysfunction in AS, with chronic inflammation histopathologically impacting myocardial tissue, valve adventitia, and intimal fibrous proliferation [25]. The process led to Left Ventricular Diastolic Dysfunction (LVDD) and followed by Left Ventricular Systolic dysfunction (LVSD) later. Okan et al., demonstrated a four-fold increased risk for LVDD in AS patients compared to healthy controls, with the most significant risk factor being increased TNF-α [32]. The progression of LVDD served as an independent indicator for the likelihood of heart failure and mortality [34,35].
Later, Doppler echocardiography in AS patients showed impaired diastolic and global LV functions, whereas in early patients they were generally asymptomatic [25,29,30,32]. This asymptomatic phase has been a challenge for previous researchers to find a method of measurement or diagnosis. Several recent studies have attempted to find factors that might be related to this cardiovascular disorder, such as red cell distribution, pre-systolic waves, and CRP [25,29,30]. These studies compared their variables to the appearance of heart function using echocardiography and an index, namely MPI.
LVEF has been the most common and focused echocardiography parameter to assess myocardial function. However, LVEF only describes systolic function. Therefore, assessment of global LV function has been suggested as an alternative to LVEF [36]. Although LVEF and MPI is a simple and non-invasive tool, but MPI has the advantage of easy-to-estimate, reproducible parameters, and considerably evaluate globally from systolic and diastolic function, whereas with its independence to the delineation of the endocardial border [8,9,10,36]. The cumulative effect of both systolic and diastolic dysfunction in AS likely underlies the observed elevation in MPI values, reflecting subclinical cardiac involvment.
Conventional echocardiography has been widely utilized for assessing ventricular functions. However, when it comes to evaluating LV diastolic function, this method relied heavily on loading conditions, particularly mitral inflow patterns, which were significantly influenced by preload and could undergo significant changes with the progression of diastolic dysfunction [37]. In contrast, TDI assessment of diastolic function was less influenced by loading conditions, allowing for easy acquisition of myocardial and annular velocities. TDI also offered a rapid way to differentiate between normal and pseudonormal patterns, as well as to distinguish between constrictive and restrictive physiologies [30].
In systolic function indices, two studies by Ozmen et al. and Rosa et al. showed significant difference of LVEF in AS patients compared to healthy subjects [10,29]. These results aligned with meta-analyses results conducted by Romand et al., which reported a statistically negligible decrease in LVEF in ax–SpA, and with Almasi S et al., which found a significant LVEF reduction (p=0.020) in AS patients compared to controls [22,38]. A study by MidtbØ H et al., reported the mean of LVEF was normal both in AS patients and controls (p=0.05) [39].
In diastolic function indices, four studies demonstrated significant differences E/A or Em/Am in AS patients compared to healthy control, relevant with Romand et al., findings, reported altered E/A ratio of ax-SpA and estimated 16.4% of LVDD and increased in axial spondyloarthritis (ax-SpA) [22]. These might have been due to diffuse myocardial infiltration and fibrosis leading to diastolic dysfunction in the early phase, followed by systolic dysfunction in the later phase. Heslinga et al., showed that diastolic dysfunction occured in a range of 9–45% among individuals with AS, even without overt cardiovascular disease and the EF is within normal range. This LVDD may eventually lead to heart failure with preserved ejection fraction (HFpEF) [40].
Albayrak et al., found no significant difference in either cMPI and tdMPI between patients with uSpA and healthy control. Different results obtained by the uSpA group in MPI could have been caused by disease progression [27]. A recent review study by Xia et al., indicated that AS developed in 22% (95%CI 11.0%–33.0%) of uSpA over 5 years, 29.1% (95%CI 25.7%–32.5%) over 8 years, and 39.9% (95%CI 19.0%–60.8%) over 10 years [41,42]. In uSpA patients, there was no significant difference of LVEF and control patients. However, the deterioration of certain diastolic parameters such as Em and Am could indicate early cardiac involvement, while the left ventricular systolic function remained preserved [27].
The cMPI demonstrated a high degree of heterogeneity, with I2 results of 87%, while the tdMPI demonstrated no substantial heterogeneity, with I2 results of 0%. The variability of cMPI could have stemmed from clinical, methodological, or statistical perspectives. From a clinical perspective, the differences in participants or outcomes could have led to high heterogeneity. The number of participants ranged from 30 to 59 subjects, with some studies having unequivocal male-to-female ratios. The larger the sample, the higher the likelihood of effect sizes to occur. Furthermore, the disease duration in each study was varied, with the shortest duration of at least one year and the longest duration being 19.14±7.51 years. This variability could have influenced the progression of cardiac damage, leading to more pronounced alterations in MPI values.
From a methodological perspective, the differences in population matching may have contributed to high heterogeneity. While the mean ages of the case and control groups exhibited minimal disparity, the age ranges demonstrated considerable heterogeneity, with 38±11 to 44.69±9.03 years in the case group and 36±9 to 43.58 ± 20.47 years in the control group [21,25,26]. Furthermore, ethnicity also played a crucial role in determining the diversity of SpA incidence and risk factors, considering the study population originated from different geographical regions, including Asia (Turkey) and Europe (Greece) [26]. Prior research revealed that the low prevalence of SpA coincided with a low prevalence of HLA-B27, which is predominantly found in Asia compared to other continents [43].
As the number of our included studies was fewer than 10, funnel plot assessment could have led to misinterpretation and unreliable results. Therefore, we conducted a qualitative evaluation using GRADE assessment as shown in table 3. Potential publication bias usually arose from the tendency of authors or publishers to release papers with only significant results. In this review, each study showed various significance in their reported outcomes of MPI values, as described in Table 4.A and 4.B, highlighting the fact that the studies included in our meta-analysis reported both significant and insignificant results.
To the best of our knowledge, this was the first comprehensive systematic review and meta-analysis focused on evaluating MPI in adult SpA patients. A notable strength of our study was the ability of MPI values to evaluate cardiac dysfunction in SpA using both conventional echocardiography and TDI, making the MPI evaluation widely and easily accessible. However, our study had some limitations. Although MPI was not widely utilized and was generally outperformed by other modalities for evaluating LV function, it might still have held clinical value in resource-limited settings. In such contexts, MPI could have served as a useful tool for detecting subclinical myocardial dysfunction in specific populations, such as AS patients. The number of studies was relatively small because MPI was not a routine assessment of cardiac function. This study only included observational studies, thus could not evaluate causative relations between SpA and impaired cardiac function. We also did not explore specific subsets of SpA other than AS due to paucity of studies for these specific subsets of SpA. Additionally, the findings might have been subject to geographical bias, as the majority of the included studies originated from Turkey, potentially limiting the generalizability of the findings.
Future studies might focus on clinical consequences of MPI towards cardiac dysfunction in SpA patients, and acceptable abnormal cut off for predictive and prognostic value. If its utility was proven, the MPI simplicity and durability could have made it a mainstay in clinical practice. Furthermore, comparing the effectiveness of TDI and conventional echocardiography in determining MPI accuracy might have helped determine which modality was better at identifying cardiac dysfunction in SpA.
Our study concluded that there were significant differences in MPI values between AS patients and healthy controls. Tissue doppler imaging and conventional echocardiography both revealed a positive trend toward increased MPI values in AS patients. Given these findings, a routine MPI assessment for early detection and management of cardiac dysfunction in AS patients might have been warranted. Further studies were needed to confirm these findings.