The heart failure (HF) epidemic is a relentlessly evolving global health burden [1]. It is recognized as one of the leading causes of mortality worldwide, with constant progress in diagnosis and management, yet with remaining challenges and unmet needs [2]. At the crossroads of multiple comorbidities, kidney disease is a prognostic factor of utmost importance in HF, doubling the risk of all-cause mortality. In this setting, specific cardiac biomarkers play an essential role in evaluating patients' prognosis. Of these, cardiac troponin (cTn) is both a marker of severity and prognosis in HF, as well as a predictor of HF or death in chronic kidney disease [3].
Especially with the use of high-sensitivity assays, troponin levels are elevated in many patients with renal failure, even in the absence of overt myocardial damage, and in most patients with heart failure with reduced ejection fraction (HFrEF). Although the mechanisms underlying this finding remain controversial, a key takeaway is the demonstrated predictive value of troponin for outcomes in these patients [4,5].
Elevated cTnT in patients with renal dysfunction may be caused by uremic cardiotoxins and reduced renal clearance, although the link does not seem to be solely due to these factors. Serum troponin T is increased more frequently than troponin I in patients with renal failure [6].
It is still unknown how much of the elevated concentration of cTn in patients with renal illness is due to impaired renal clearance [7]. Additional mechanisms have been considered, including oxidative injury [8], supply/demand mismatch [9], increased inflammation [10], and dialysis-related physiologic changes such as hemodynamic shifts and anemia [11]
In patients with HFrEF, even in those with mild to moderate CKD, elevated levels of hs-TnT were strongly associated with incident HF [12].
In patientss with advanced CKD and preserved LVEF, troponin levels are associated with diastolic dysfunction and an increased risk of mortality [13,14].
A meta-analysis [15] showed that hs-TnT levels independently predict long-term all-cause and cardiovascular mortality, as well as cardiovascular hospitalization. The outcome was unaffected by HF etiology or renal function.
Some studies found an association between long-term all-cause mortality and higher troponin levels in chronic disease (CKD). However, this association lost significance once adjusted for the severity of CKD, leaving uncertainty regarding the role of renal filtration in modulating cardiac troponin levels in CKD [16,17].
Interestingly, it is still unclear why significantly most patients have an increased cTnT versus cTnI in ESRD [16].
Applying general population biomarker thresholds to CKD patients compromises diagnostic accuracy, as many asymptomatic individuals with advanced CKD exhibit positive results, thus obscuring the prognosis of cardiovascular events.
Optimizing troponin cut-off values for prognostication in heart failure (HF) is challenging; a meta-analysis of 10 studies identified 18 ng/L hs-cTnT as ideal, but this value varied by sex and increased with worsening renal function, impacting predictive accuracy, particularly at later stages of CKD [3,15].
A retrospective cohort analysis [18] showed that using the GFR-specific cutoffs, hs-cTnT was strongly associated with cardiovascular events. They determined the optimal cut-off value for hs-cTnT at 22.7 ng/L for an eGFR of 30–44 mL/mi, a value of 26.8 ng/L for an eGFR of 20–29 mL/min, and a value of 35.5 ng/L for an eGFR below 20 mL/min. Moreover, these GFR-specific cutoffs showed superior prognostic value compared with standard cutoffs, supporting the concept of GFR-specific cutoffs for cardiovascular risk stratification in patients with advanced CKD.
The methodology for this systematic review was in concordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 statement guidelines [19].
We searched the PubMed (MEDLINE) database from the year 2011 until September 1, 2024, using the main keywords “heart failure”, “troponin”, “prognosis”. A second search was conducted on October 21, 2024, using the same strategy, and the results were considered final. The strategy is detailed in Supplementary Material – Table 1.
Two authors independently reviewed the titles and abstracts of the articles. Each author independently selected articles for inclusion in the analysis. In case of disagreement, a third author determined whether the articles should be included.
We included all study designs that evaluated the prognostic value of troponin in heart failure, provided they also conducted a multivariable analysis that considered renal function.
Evaluation of renal function was considered any type of assessment: eGFR (either qualitative or quantitative assessment), creatinine, urea, cystatin C, BUN levels, diagnosis of CKD, and stratification of CKD.
We did not impose any restrictions on sample size, study duration, or the interventions given to patients.
Only English-written articles were included in the analysis.
Reviews, meta-analyses, systematic reviews, case reports, and animal studies were excluded.
Studies on cohorts including HF among other diagnoses, without separate analysis of the HF subgroups were also excluded.
Studies that reported only composite outcomes were excluded to ensure clarity in assessing individual effects and to avoid potential biases introduced by heterogeneous components.
Our initial search retrieved 1324 publications, of which 992 were considered for inclusion. 65 publications were analysed in the full-text selection. After applying the inclusion and exclusion criteria 29 full-text records were selected for this review, with a total of 36134 patients evaluated. The selection process is detailed in Figure 1.
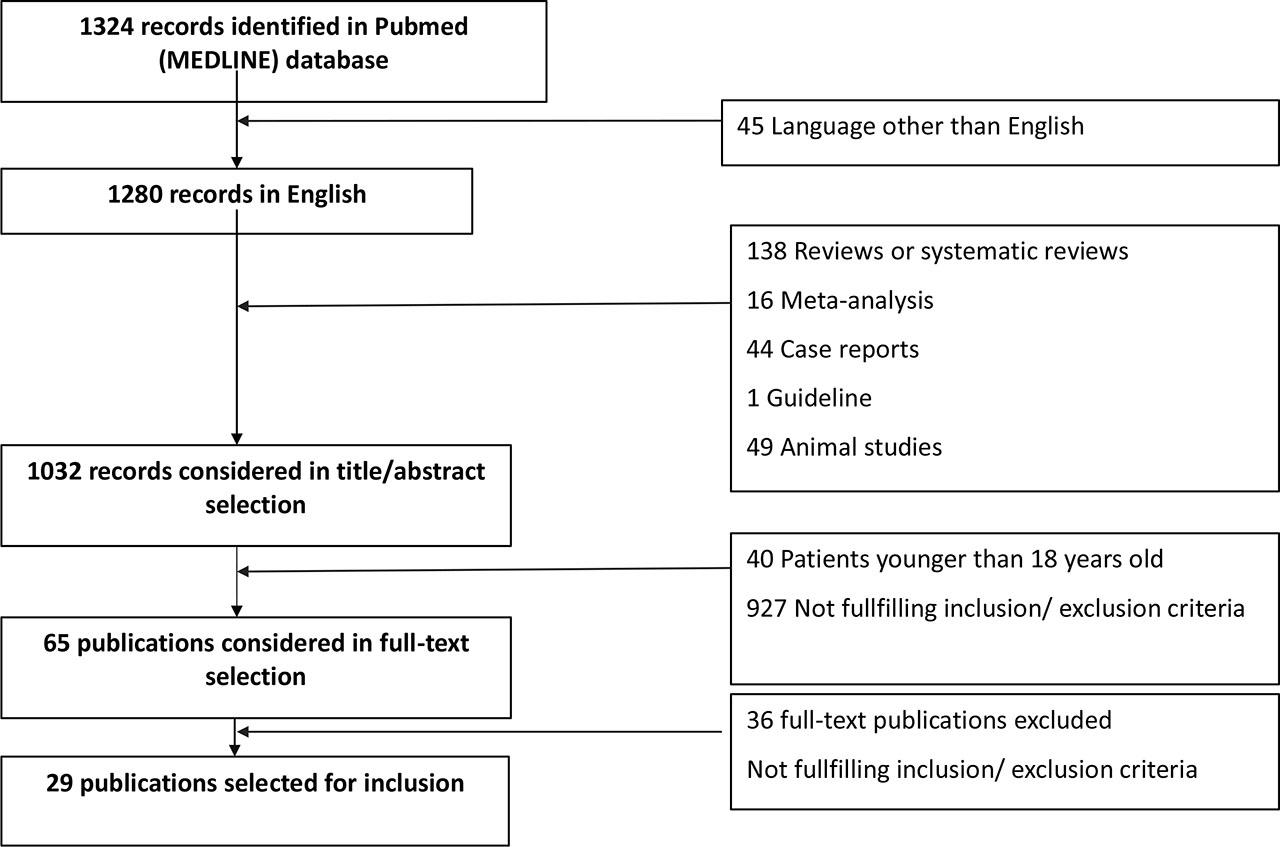
Flowchart for the process of article selection.
General characteristics of the included studies
| Author, year | Study Type | Population (N) | Baseline Pathology | Duration of Follow-up | Type of troponin | Main Outcome(s) |
|---|---|---|---|---|---|---|
| Yilmaz Oztekin, 2023 [48] | Retrospective cohort study | 249 |
| 30 months | hs-cTnT | All-cause mortality |
| Bosselmann, 2013 [49] | Prospective cohort study | 424 |
| 4.5 years (IQR: 2–7.7) | hs-cTnT | All-cause mortality |
| Aulin, 2022 [26] | Substudy of a RCT (ARISTOTLE) | 4568 |
| 1.9 years (median) | hs-cTnT |
|
| Berge, 2022 [27] | Retrospective analysis of a prospective cohort study (ACE 2 study) | 143 |
| 823 days (median) | hs-cTnT | All-cause mortality |
| Berge, 2021 [31] | Retrospective analysis of a prospective cohort study (ACE 2 study) | 143 |
| 464(median) | Hs-TnT | All-cause mortality |
| Aimo, 2019 [28] | Retrospective analysis of data from 3 cohorts | 1449 |
| 11 months (median) | hs-cTnT |
|
| Ledwoch, 2021 [30] | Retrospective cohort study | 971 |
| 30 days | hs-cTnT | All-cause mortality |
| Ledwoch, 2022 [29] | Retrospective registry | 847 |
| 30 days | hs-cTnT | All-cause mortality |
| Jungbauer, 2014 [32] | Prospective cohort study | 149 |
| 757 days (mean) (IQR 711-809) | hs-cTnT |
|
| Guisado-Espartero, 2014 [33] | Prospective cohort study RICA registry | 406 |
| 1 year | cTnT |
|
| Zymliński, 2017 [22] | Prospective cohort study | 130 |
| 1 year | hs-cTnI | Cardiovascular mortality |
| O'Connor, 2011 [51] | Substudy of an RCT (PROTECT study) | 288 | AHF with renal insufficiency | 60 days (primary) and 7 days (secondary) | cTnT |
|
| Barlera, 2013 [34] | Prospective RCT (GISSI-HF) | 6975 |
| 3.9 years | hs-cTnT | All-cause mortality |
| Masson, 2012 [35] | Substudy of two RCTs (Val-HeFT & GISSI-HF) | 5284 |
| Val-HeFT: 24 months (median); GISSI-HF: 47 months (median) | hs-cTnT |
|
| Lupon, 2013 [36] | Prospective cohort study | 876 |
| 41.4 months | hs-cTnT | All-cause mortality |
| Ather, 2013 [37] | Retrospective cohort study | 196 |
| 5 years | cTnI | All-cause mortality |
| Lok, 2013 [38] | Substudy of an RCT DEAL-HF | 209 | CHF | Median 8.7 years (8.7 ± 1 year) | hs-cTnT | All-cause mortality |
| Egstrup, 2012 [39] | Prospective cohort study | 416 |
| Median 4.4 years (IQR: 1.9-7.5) | hs-cTnT | All-cause mortality Composite outcome of all-cause mortality and cardiovascular hospitalization |
| Zhang, 2015 [40] | Retrospective analysis of a prospective cohort study | 1189 |
| 1 year | cTnT, cTnI | All-cause mortality |
| Kawahara, 2011 [20] | Prospective cohort study | 95 |
| 4.25 years | hs-cTnI | Cardiovascular mortality |
| Fabbri, 2015 [41] | Retrospective analysis of SAFE-SIMEU database | 1234 |
| 1 year | All-cause mortality | |
| Lee, 2022 [42] | Retrospective analysis of a prospective registry (KorAHF) | 4396 |
| 784 days (IQR 446–1116) | hs-cTnI | All-cause mortality |
| Bayes-Genis, 2013 [43] | Prospective cohort study | 879 |
| 3.46 years (mean) | hs-cTnT | All-cause mortality |
| Felker, 2012 [44] | Biomarker substudy within an RCT ASCEND-HF | 808 |
| 180 days | cTnI |
|
| Mcdowell, 2023 [45] | Biomarker substudy within an RCT (PARADIGM-HF trial) | 1559 |
| 30.7 months (mean) | hs-cTnT |
|
| Demissei, 2021 [23] | Post-hoc analysis of an RCT (RELAX-AHF) | 1161 |
| 180 days | hs-cTnT | Cardiovascular mortality |
| Tentzeris, 2011 [46] | Prospective cohort study | 172 |
| 1301 days | hs-cTNT | All-cause mortality or HF hospitalization |
| Bjurman, 2012 [47] | Prospective cohort study | 131 |
| 3 years | cTnT | All-cause mortality |
| Horiuchi, 2021 [50] | Retrospective analysis of a prospective cohort (AKINESIS study) | 787 | AHF | 1 year | hs-cTnI |
|
AHF, acute heart failure; CHF =,chronic heart failure; CKD, chronic kidney disease; cTnI, cardiac troponin I; cTnT =,cardiac troponin T; HF, heart failure; HFrEF, heart failure with reduced ejection fraction; hs-cTnI, high sensitivity cardiac troponin I; hs-cTnT, high sensitivity cardiac troponin T; IQR, interquartile range; LVEF, left ventricular ejection fraction; RCT, randomized clinical trial, WRF, worsening renal failure
Four articles [20,21,22,23] evaluated cardiovascular mortality as the primary endpoint. Two studies [22,23] focused on patients with acute heart failure, excluding acute coronary syndromes, while the other two [20,21] focused on patients with non-ischemic chronic heart failure. Among them, two studies analysed hs-cTnI, and the other two examined hs-cTnT.
These studies included a total of 6,670 patients. The largest cohort, comprising 5,284 CHF patients with all types of LVEF, was analysed retrospectively using data from two clinical trials, VAL-HeF [24] and GISSI-HF [25] as reported by Masson et al. (2012). The smallest study [21] investigated 95 stable outpatients with nonischemic CHF with dilated cardiomyopathy (DCM) as the underlying etiology in 70 patients.
Data from this studies suggests that high-sensitivity cardiac troponin T (hs-cTnT) and high-sensitivity cardiac troponin I (hs-cTnI) are independent predictors of cardiovascular mortality and cardiac death in patients with acute heart failure (AHF) [23], even after adjusting for various confounding factors including other biomarkers and renal function [22]. Kawahara et al. demonstrates an association between increasing troponin levels and mortality risk, hs-cTnI at baseline (0.03 ng/mL) (P = .0011), change in hs-cTnI after 6 months (hs-cTnI 0 ng/mL) (P = .022) (P = .0008) was significant independent predictor of cardiac death [21]. While the inclusion of other clinical risk factors in the models reduced the overall risk estimates, the association between elevated hs-cTnT and mortality risk remained, with hazard ratios ranging from 1.40 to 2.99 across various trials and outcomes [20].
Details of studies evaluating cardiovascular mortality
| AUTHOR/YEAR | Type of biomarker | Troponin cut off | HR/OR (95%CI) | HR/OR (95%CI) | Parameters included in the adjusted/multivariable analysis |
|---|---|---|---|---|---|
| Unadjusted (univariable) analysis | Adjusted (multivariable) analysis | ||||
| Zymliński 2017 [22] | hs-cTnI | >= URL | 1.44 | - | systolic blood pressure, natural logarithm of N-terminal pro-B type natriuretic peptide, diabetes mellitus and chronic kidney disease. |
| Increase vs stable/decrease | 2.22 | 1.90 (0.84–4.29) | |||
| 1Ln/pgml | 1.97 (1.88–7.87) | 1.67 (1.01–2.76) | |||
| Increase vs decrease | 3.84 (1.88–7.87) | 3.22 (1.52–6.82) | |||
| Kawahara 2011 [21] | hs-cTnI | hs-cTnI at baseline (ng/mL) (≥0.03 = 1, b0.03 = 0) | 15.895 | 10.679 | age, sex, NYHA class, body weight, creatinine |
| 5.7 (1.2–7.9) | |||||
| Demissei 2017 [23] | hs-cTnT | 1.63 (1.46–1.81) | 1.64 (1.44–1.88) | Adjusted for a pre-defined baseline model encompassing clinical variables (geographic region, systolic blood pressure, orthopnoea, angina, hyperthyroidism, mitral regurgitation, and atrial fibrillation/flutter at screening), laboratory parameters (white blood cell count, lymphocyte %, blood urea nitrogen, sodium, potassium, calcium, and total protein), and study treatment. The covariate orthopnoea on the ordinal scale (0,1,2,3) was dichotomized into binary as: orthopnoea: 2/3 vs. 0/1. Rationale: there were 0 subjects who died due to cardiovascular causes for orthopnoea level ‘none | |
| Masson 2012 [5] | hs-cTnT | upper limit of 13.5 ng/L | Mortality for worsening heart failure Val-HeFT 2.32 (1.90–2.82) | 2.26 (1.78–2.86) | age, BMI, LVEF, NYHA class, ischemic etiology of HF, systolic and diastolic blood pressures, prescription of diuretics, beta-blockers or spironolactone, serum creatinine, log baseline hs-cTnT. |
| age, BMI, LVEF, NYHA class, ischemic etiology of HF, systolic and diastolic blood pressures, heart rate, diabetes mellitus, atrial fibrillation, COPD, prescription of diuretics or betablockers, serum bilirubin, serum creatinine, log baseline hs-cTnT. | |||||
| Mortality for worsening heart failure GISSI-HF 2.99 (2.30–3.89) | 2.9 (2.08–4.03) | ||||
BMI, body mass index; COPD, Chronic Obstructive Pulmonary Disease; HF,heart failure; LVEF, left ventricle ejection fraction; NYHA,New York Heart Association; hs-cTnT, High-sensitivity cardiac troponin T;
Twenty five studies reported the predictive utility of troponin for all-cause mortality in heart failure, adjusted by the renal function [26,27,36,37,38,39,40,41,42,43,44,45,28,46,47,48,49,50,29,30,31,32,33,34,35]. The total number of patients was 25203, with five studies [27,30,34,43,49] focusing on cohorts partially or fully included in previous analyses [29,31,35,36,39].
The majority of studies reported the prognostic performance of hs-cTnT [27,28,43,45,46,49,50,29,30,31,32,35,36,38,39]. Three studies reported cTnT [26,33,47], three studies cTnI [37,42,44], one study included patients with either cTnT or cTnI measurements [41], one had a separate analysis for cTnT and cTnI [40].
Thirteen studies involved a prospective analysis [27,31,46,47,49,32,33,34,36,39,40,42,43], and the remaining twelve, a retrospective analysis [26,28,48,50,29,30,35,37,38,41,44,45].
The majority of studies included patients across the entire spectrum of LVEF [26,27,36,41,42,43,47,28,29,30,31,32,33,34,35], nine investigated patients with LEVF <50% [37,39,40,43,44,45,46,48,49], and one did not mention the cohort's LVEF [50].
Details of studies evaluating all-cause mortality
| 3A. ALL-CAUSE MORTALITY IN CHRONIC HEART FAILURE | ||||||
|---|---|---|---|---|---|---|
| Author, year | Type of biomarker | Troponin cut-off | Outcome | HR/OR (95%CI) | HR/OR (95%CI); | Parameters included in the adjusted/multivariable analysis |
| Unadjusted (univariable) analysis | Adjusted (multivariable) analysis | |||||
| Barlera 2012 [34] | hs-cTnT |
| Median 3.9 years | HR 1.50 (1.24 – 1.81) | NT-proBNP, NYHA class, age, COPD, SBP, DM, eGFR, sex, uricemia, LVEF, Hb, BMI, aortic stenosis | |
| Bayes-Genis 2013 [43] | hs-cTnT | Continuous variable, logarithmic form | Median follow-up 3.46 (1.85 – 5.05) years | Total cohort HR 2.71 (2.25 – 3.26), p<0.001 | Total cohort HR 1.58 (1.27 – 1.97), p<0.001 | age, sex, ischemic etiology of HF, LVEF, NYHA class, DM, Hb (g/dL), serum Na (mmol/L), BB treatment, ACEI/ARB treatment, eGFR (in mL/min/1.73 m2), NT-proBNP, cystatin C, sST2 |
| Renal insufficiency HR 2.62 (2.04 – 3.37), p<0.001 | Renal insufficiency subgroup HR 1.65 (1.24 – 2.2), p<0.001 | |||||
| McDowell 2023 [45] | hs-cTnT | Continuous variable, log transformed | median 37 months | HR 1.63 (1.31 – 2.03), p<0.001 | PREDICT-HF score: Age, sex, race, BMI, region, time since HF diagnosis, NYHA class, prior HF hospitalization, treatment with sacubitril-valsartan/beta-blocker, DM, PAD, prior MI, valvular heart disease, bundle branch block, prior PCI, LVEF, SBP, serum K, Cl, BUN, uric acid, albumin, bilirubin, total cholesterol, LDL, triglycerides, AST, Hb, absolute lymphocyte count, absolute neutrophil count, absolute monocyte count, NT-proBNP or BNP | |
| Lupon 2013 [36] | hs-cTnT | Continuous variable quadratic term, logarithmic function of hs-cTnT | Median 41.4 (IQR 22.1 – 60.5) m | HR 11.68 (5.51 – 24.75) | HR 3.9 (1.81 – 8.41) | age, sex, LVEF, eGFR, BMI, NYHA functional class, DM, COPD, AF, ischemic etiology, Hb, serum Na, BB treatment, and ACEI or ARB |
| Masson 2012 [5] | hs-cTnT |
|
|
|
|
|
|
| |||||
| Lok 2013 [38] | hs-cTnT | hs-cTnT > 26.5 ng/ml | Median 8.4 years | HR 1.53 (1.32 – 1.78) |
|
|
| Yilmaz Oztekin 2023 [48] | hs-cTnT | Hs-cTnT ≥ 21.5 ng/L | median follow-up of 30 months | HR 1.012 (1.007–1.017), p<0.001 | HR:1.012, 95% CI:1.003–1.020, p= 0.005 | eGFR, hemoglobin, NT-proBNP, BMI, and left atrial diameter |
| Tentzeris 2011 [46] | hs-cTnT | hs-cTnT > 14 pg/mL | median follow-up 1301 [707 – 1636] days) | HR 4.54; 95% CI, 1.92–10.73, p<0.001 | HR 1.92 (1.11 – 3.33) p=0.02 | age, sex, NYHA class, eGFR <60 mL/min/1.73m2, median NT-proBNP > 1809 pg/mL |
| Jungbauer 2014 [32] | hs-cTnT | hs-cTnT > 14 ng/L | 3-year follow-up | OR 4.80 (1.58 – 14.59) p = 0.0057 | HR 1.2 (1.03 – 1.50) p = 0.025 | Age, eGFR, LVEF, NYHA class > 2 |
| Bosselmann 2013 [49] | hs-cTnT | Quartile groups | median follow-up of 4.5 (interquartile range: 2–7.7) years | HR 3.07 (1.90 – 4.96) P<0.001 | age, sex, LVEF, NYHA class, DM, IHD, eGFR | |
| Egstrup 2012 [39] | hs-cTnT | Quartile groups | Median 4.4 (IQR 1.9 – 7.5) years |
|
| age, gender, LVEF, NYHA class, DM, CAD, Hb, eGFR, interval of inclusion |
| The gender-specific 99th percentile concentration limit as established in a healthy population: men > 18 ng/L women > 8 ng/L |
| age, gender, LVEF, NYHA class, DM, CAD, Hb, eGFR, interval of inclusion, NT-proBNP | ||||
| Aulin 2022 [26] | cTnT | Continuous variable Log-transformed, natural logarithm |
| χ2 = 220 | χ2 = 127 | Step 1: randomized treatment, age, sex, HTN, DM, CAD, history of stroke/TIA, BMI, HR, SR, renal function (CrCl) |
| χ2 = 56 | Step 2: Step 1 + N-terminal B-type natriuretic peptide (NT-proBNP) | |||||
| Zhang 2015 [40] | Separate analysis for cTnT and cTnI | 90th percentile cTnT > 0.105 ng/ml | 1-year all-cause mortality | OR 3.9 (1.96 – 7.76) | age ≥75 years, NYHA class III/IV, AF, eGFR < 30 mL/min/1.73 m2, DM, use of diuretics | |
| 90th percentile cTnI | 1-year all-cause mortality | OR 1.59 (0.65 – 3.88) | age ≥75 years, NNYHA class III/IV, AF, eGFR < 30 mL/min/1.73 m2, diabetes, use of diuretics | |||
| 3B. ALL-CAUSE MORTALITY IN ACUTE HEART FAILURE | ||||||
| Berge 2021 [31] | hs-TnT |
| Long-term all-cause mortality | HR 1.37 (95%CI 1.10 – 1.71) | HR 1.20 (95%CI 0.93 – 1.55) | Age, male sex, BMI, NYHA class IV, COPD, DM, NT-proBNP, CRP, eGFR |
| Berge 2022 [27] | hs-TnT |
| HR 1.37, 95% CI 1.10 – 1.61 | Not statistically significant | NEWS2 score, age, male sex, BMI, smoking, NYHA class IV, HF, AF, COPD, CAD, hypertension, diabetes, NT-proBNP, CRP, eGFR | |
| Ledwoch 2022 [30] | hs-TcnT |
| 30-day all-cause mortality |
| age, sex, NYHA class, DM, HTN, MI, AF, eGFR | |
| Aimo 2019 [28] | hs-cTnT | hs-cTnT ≥ 43 ng/L | In-hospital mortality RR 2.7 (95%CI 1.7 – 4.5) |
| Patient cohort, age, sex, new-onset vs.worsening HF, history of CAD, admission LVEF, NYHA class, SBP, Hr, eGFR, Hb, Na, white blood cell count, history of AF, HTN, DM, COPD | |
|
|
| ||||
| Ledwoch, 2021-2022 [30] | hs-cTnT |
| 30-day all-cause mortality |
| N/A | N/A |
| Horiuchi 2021 [50] | hs-cTnI | Continuos variable log-2 transformed | 1-year all-cause mortality |
| HR 1.12 (1.03 – 1.22), p=0.012 | age, Black race, history COPD, oedema, SBP, Hr, Na, Hb, and BUN, BNP, sNGAL, uNGAL, and Gal3. |
| Guisado Espartero 2014 [33] | cTnT | cTnT > 0.02 ng/mL | 1-year all-cause mortality | 2.52 (1.58 – 4.01) | 1.91 (1.09 – 3.32) | age, female sex, BMI > 25 kg/m2, IHD, previous HF, anemia, LVEF < 45%, NYHA III–IV, eGFR < 60 mL/min/1.73m2, NT-proBNP > 3264 pg/mL |
| Separate analysis of patients with eGFR<60: patients with eGFR < 60 mL/min/1.73 and intermediate-high TnT had more deaths than those with eGFR > 60 mL/min/1.73 | ||||||
| Bjurman 2013 [47] | cTnT | cTnT>10ng/L | All-cause long-term mortality at 3 years | HR 2.94 (1.06 – 8.15), p=0.038 | HR 147 (11.2 – 1929.8), p<0.001 | Age, ALP, urea, creatinine, orosomucoid, NT-proBNP, TnT, CK-MB, CysC |
| Ather 2013 [37] | cTnI with 3 measurements during 3 different admissions |
|
|
|
| age, gender, race, ischemic etiology of HF, EF, NYHA class, number of vessels having more than 50% stenosis on angiography, baseline admission TnI, baseline peak TnI, CV admission, HF admission and total number of admissions during the run-in period; history of smoking, HTN, PAD, AF, DM, COPD, CKD, LVF, CAD |
| Felker 2012 [44] | cTnI | Continuous variable, log transformed in using log base 2 | Death at 30 days |
| Doubling of cTnI: OR 1.11 (0.89 – 1.38), p=0.37 | Age, log(BUN), serum sodium, hypotension (baseline), dyspnoea at rest |
| Death at 180 days | Doubling of cTnI: HR 1.25 (1.13 – 1.38), p<0.001 | Doubling of cTnI: HR 1.11 (0.99 – 1.25), p=0.086 | Age, log(BUN), serum sodium, hypotension (baseline), dyspnoea at rest (baseline). | |||
| Lee 2022 [42] | cTnI | cTnI≥0.05 ng/mL (elevated); <0.05 ng/mL (normal) | Overall all-cause mortality |
|
| Age, sex, previous history of admission due to HF, HTN, DM, CKD, COPD, CVA, prior history of CAD, MI, malignancy, initial SBP, initial LVEF, initial Na, initial Cr, AF at admission, medication at discharge, including ACEI/ARB, BB, or AA |
| cTnI≥0.05 ng/mL | 90-day all-cause mortality |
|
| |||
| cTnI≥0.05 ng/mL | Post-90-day all-cause mortality |
|
| |||
| Fabbri 2015 [41] | cTnT or cTnI |
| 1-year all-cause mortality | HR 1.21 (1.05 – 1.39) | age, sex, new-onset dysrhythmias, cardiac valvular diseases, CAD, presence PM or ICD, history of AHF, CKD, COPD, DM, CVD, cognitive defects, poor nutritional status, compliance with pharmacology prescriptions (ACEI, ARB, BB, loop diuretics, MRA, anticoagulants, antithrombotic agents), plasma Na<135 mEq/L, NT-proBNP > 5000ng/L, eGFR < 30 mL/min/1.73m2 | |
AA, aldosterone antagonist; ACEI, angiotensin-converting enzyme inhibitor; AHF, acute heart failure; AF, atrial fibrillation; ARB, /angiotensin II receptor blocker; AST, aspartate transferase; BB, beta blocker; BMI, body mass index; BUN, blood urea nitrogen; CAD, coronary artery disease; CHF, chronic heart failure; CKD, chronic kidney disease; CI, confidence interval; Cl, chloride; COPD, chronic obstructive pulmonary disease; CrCl, creatinine clearance; CV, cardiovascular; CVD, cardiovascular disease; CVA, cerebrovascular accident; CysC, cystatin C; cTnI, cardiac troponin I; cTnT, cardiac troponin T; DBP, diastolic blood pressure; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; EF, ejection fraction; Gal3, galectin 3; Hb, hemoglobin; HF, heart failure; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; HR, hazard ratio; Hr, heart rate; hs-CRP, high sensitivity C reactive protein; hs-cTnI, high sensitivity cardiac troponin I; hs-cTnT, high sensitivity cardiac troponin T; HTN, arterial hypertension; IHD, ischemic heart disease; IHF, ischemic heart failure; IQR, interquartile range; K, potassium; LDL, low density lipoprotein; Log, logarithmic transformation; LVH, left ventricular hypertrophy; MI, myocardial infarction; MRA, mineralocorticoid receptor antagonist; N/A, non applicable; Na, sodium; NYHA, New York Heart Association; OR, odds ratio; PAD, peripheral arterial disease; PCI, percutaneous coronary intervention; Q, quartile; SBP, systolic blood pressure; sNGAL, serum Neutrophil gelatinase-associated lipocalin; sST2, soluble ST 2; SR, sinus rhythm; TIA, transient ischemic attack; uNGAL, urine Neutrophil gelatinase-associated lipocalin; ↓, decrease; ↑, increase;
Thirteen studies enrolled 14682 patients with CHF [26,32,46,48,49,34,37,36,38,39,40,43,45], the majority reporting hs-cTnT [32,34,49,35,36,38,39,43,45,46,48], one using cTnT [26] and one including a separate analysis for cTnT and cTnI [40]. Troponin was expressed as absolute values, percentual variations, logarithmic transformation, dichotomic variable using different cut-offs (Table 3A).
hs-cTnT evaluated as a continuous variable after logarithmic transformation was associated with all-cause mortality independent of renal function assessed by eGFR [34,36,43] or BUN [45] in four studies undertaken on three cohorts of patients with reduced LVEF [45], reduced and mildly reduced EF [36,43] or all types of LVEF [34]. Moreover, in a subgroup analysis of patients with eGFR<60 mL/min/1.73m2, after multiparametric adjustment, hs-cTnT remained an independent predictor of all-cause mortality [43] (Table 3A).
Three distinct cut-off values of hs-cTnT, respectively hs-cTnT > 14 ng/L [32,46], hs-cTnT > 21.5 ng/L [48] and hs-cTnT > 26.5 ng/L [38] were proven to be independently associated with all-cause mortality after adjusting for eGFR as a continuous parameter [32,38,48] or as a dichotomic variable using the eGFR <60 mL/min/1.73m2 cut-off [46]. One study used gender-specific cut-off values, respectively > 18 ng/L for men and > 8 ng/L for women in the multivariable analysis for all-cause long-term mortality and confirmed the predictive power independent of renal function estimated by the eGFR [39] (Table 3A).
Two analyses of the same cohort demonstrated the incremental prognostic value of higher hs-cTnT quartiles for long-term all-cause mortality, independent of eGFR, LVEF, NYHA class and other comorbidities [39,49] (Table 3A).
The rise of hs-cTnT levels > 15% from baseline during follow-up was also associated with all-cause mortality, independent of creatinine levels [35] in a large cohort of patients from two clinical trials, Val-HeFT [24] and GISSI-HF [25] (Table 3A).
cTnT evaluated as a log-transformed continuous variable was also independently associated with all-cause mortality in a sub study of the ARISTOTLE trial, after adjustment for creatinine levels [26]. cTnT and cTnI values in the 90th percentile, analysed separately, were predictive of 1-year all-cause mortality in HF patients with reduced LVEF and ICD implantation in primary prevention, after adjusting for eGFR < 30 ml/min/1.73m2 among other parameters [40] (Table 3A).
Twelve studies included 10521 AHF patients [27,28,47,50,29,30,31,33,37,41,42,44], analyzing the entire range of troponin: hs-cTnT [27,28,29,30,31], hs-cTnI [50], cTnT [33,47], cTnI [37,42,44], either cTnT or cTnI [41]. All-cause mortality was documented in-hospital [28], at 30-days [29,30,44], over the first months post-discharge [28,42,44] or after long-term follow-up [27,28,31,33,37,41,42,47,50]. The majority of studies included patients with all types of LVEF [27,28,29,30,31,33,41,42,47] and two included patients with reduced LVEF [37,44] (Table 3B).
hs-cTnT evaluated as a continuous variable was associated with 30-day all-cause mortality after adjustment for eGFR among other parameters, irrespective of the type of LVEF [30]. For inhospital mortality discordant results were reported [28]. In multivariable analysis including eGFR, log2-transfomed hs-cTnT was independently correlated with in-hospital all-cause mortality, while the dichotomic value of hs-cTnT > 43 ng/L was not [28]. The quantitative value of hs-TnT was also evaluated for predicting long-term all-cause mortality with conflictive results from the same cohort after multiparametric adjustment, the negative results arising after including the NEWS2 score in the regression analysis [27,31]. Three different cut-off values of hs-cTnT were independently associated with all-cause long-term mortality in AHF, respectively hs-cTnT > 43 ng/L adjusted for eGFR [28], hs-cTnT > 40 ng/L in patients with eGFR ≥ 45 ml/min and hs-cTnT > 55 ng/L in patients with eGFR < 45 ml/min [29] (Table 3B).
hs-cTnI assessed as a continuous variable log2-transformed was also independently correlated with 1-year all-cause mortality after multivariable adjustment including BUN as a marker of renal function [50] (Table 3B).
The prognostic value of cTnT was evaluated as a dichotomic variable using two cut-off values. cTnT > 20 ng/L was correlated with 1-year all-cause mortality independent of eGFR < 60 ml/min/1.73m2 [33]. cTnT > 10 ng/L was predictive of 3-year all-cause mortality after adjustment for creatinine levels [47] (Table 3B).
Discordant results were obtained for cTnI across three different cohorts. cTnI as a continuous variable was not associated with all-cause death at 30 or 180 days in patients with reduced LVEF [44]. In patients with reduced LVEF with multiple admissions for AHF and three cTnI measurements during different hospitalizations, those with the minimum TnI > 40 ng/L had a higher risk of all-cause long-term mortality, after adjusting for chronic kidney disease among other multiple clinical and biological parameters [37]. When evaluating patients stratified by the HF etiology, cTnI > 50 ng/L was an independent predictor of all-cause 90-day mortality in both patients with ischemic and non-ischemic HF, while the same cut-off was only correlated with post-90-day mortality in non-ischemic HF, and not in ischemic patients [42] (Table 3B).
Using the cut-off values of cTnT ≥ 50 ug/L and cTnI ≥ 0.5 ng/L, Fabbri et al. confirmed that a positive troponin, regardless of the type, was independently associated with 1-year all-cause mortality in AHF patients, after multiple adjustments for clinical, laboratory and treatment parameters, including not only CKD, but also eGFR < 30 ml/min/1.73m2 [41] (Table 3B).
Heart failure hospitalizations have been a frequent outcome followed by the articles included in this review, either alone (4 studies) or as part of a composite outcome (10 studies).
Noteworthy, some studies [51], [33] found that a baseline troponin T was associated with a higher risk for heart failure hospitalization, compared with patients with negative troponin T at baseline. however, the association did not reach statistical significance (HR 1.61; P=0.07, respectively p=0.37). Still, for the letter study, comparing the subgroups according to renal function did not reveal differences in heart failure readmission.
A model including hs-cTnT along with other biomarkers identifies eRFG as an independent predictor for mortality but not for CV hospitalizations (HR 0.97; 95%CI 0.87–1.09; p=0.59) [52]. Additionally, hs-cTnT cut-off values that predict endpoints increased with declining renal function. When troponin was analyzed independently, a correlation was observed between its predictive value for rehospitalization as renal function declines. However, this correlation was only evident down to an eGFR of 30 ml/min/1.73m2, below which it was no longer present (Table 4).
Other studies, however, found a potential prognostic value for predicting an increased risk of heart failure hospitalization in pts with increased troponin at baseline. In a substudy of the ARISTOTLE trial [26] there were strong indications of non-linear associations between log biomarker levels and the log rate of hospitalization for HF (unadjusted χ [2] =5.54; p-0.062; adjusted χ [2]=6.29; p=0.0454). The model was adjusted into two steps; the first step included renal function. Higher levels of troponin were independently associated with a higher probability of hospitalization for HF, regardless of HF status at baseline.
Details of studies evaluating heart failure hospitalizations
| Author, year | Type of biomarker | Troponin cut-off | HR/OR (95%CI) | HR/OR (95%CI) | Parameters included in the adjusted/multivariable analysis |
|---|---|---|---|---|---|
| Unadjusted (univariable) analysis | Adjusted (multivariable) analysis | ||||
| O'Connor, 2011 [51] | cTnT | 0.01 ng/mL | 1.64; p=0.08 | ||
| 0.03 ng/mL | 1.61; p =0.07 | ||||
| Espartero, 2014 [33] | cTnT | 0.02 ng/mL | 1.25 (0.83-1.89); p=0.29 | 1.13 (0.72-1.77); p=0.59 | Age, Sex, BMI, Ischemic heart disease, Previous HF, Anemia, LVEF, NYHA III-IV, eGFR b 60 mL/min/1.73 m2, Troponin T, NT-proBNP |
| Aulin, 2022 [26] | hs-cTnT | Continuous variable (Log-transformed using natural logarithm) | χ2 =5.54; p=0.062 | χ2=6.29; p=0.0454 |
|
| Aimo, 2019 [28] | hs-cTnT | limit of detection 5 ng/L, upper reference value 14 ng/L | HR 0.97; 95%CI 0.87-1.09; p=0.59 |
| |
| hs-cTnT | 1.41 (1.35-1.47); p <0.001 | ||||
| eGFR ≥90 | 1.37 (1.06-1.76) p=0.014 | ||||
| mL/min/1.73 m2 | |||||
| eGFR 60-89 | |||||
| mL/min/1.73 m2 | 1.40 (1.31-1.50); <0.001 | ||||
| eGFR 30-59 | |||||
| mL/min/1.73 m2 | 1.45 (1.36-1.54); p<0.001 | ||||
| eGFR <30 mL/min/1.73 m2 | 1.17 (0.96-1.42); p =0.121 | ||||
BMI, body mass index; CrCl, creatinine clearance; eGFR estimated Glomerular Filtration; HR, hazard ratio; HF, heart failure; hs-CRP, High-sensitivity C-reactive protein;LVEF, left ventricle ejection fraction;NYHA,New York Heart Association; NT-proBNP, N-terminal pro b-type Natriuretic Peptide; TIA, transient ischemic attack;
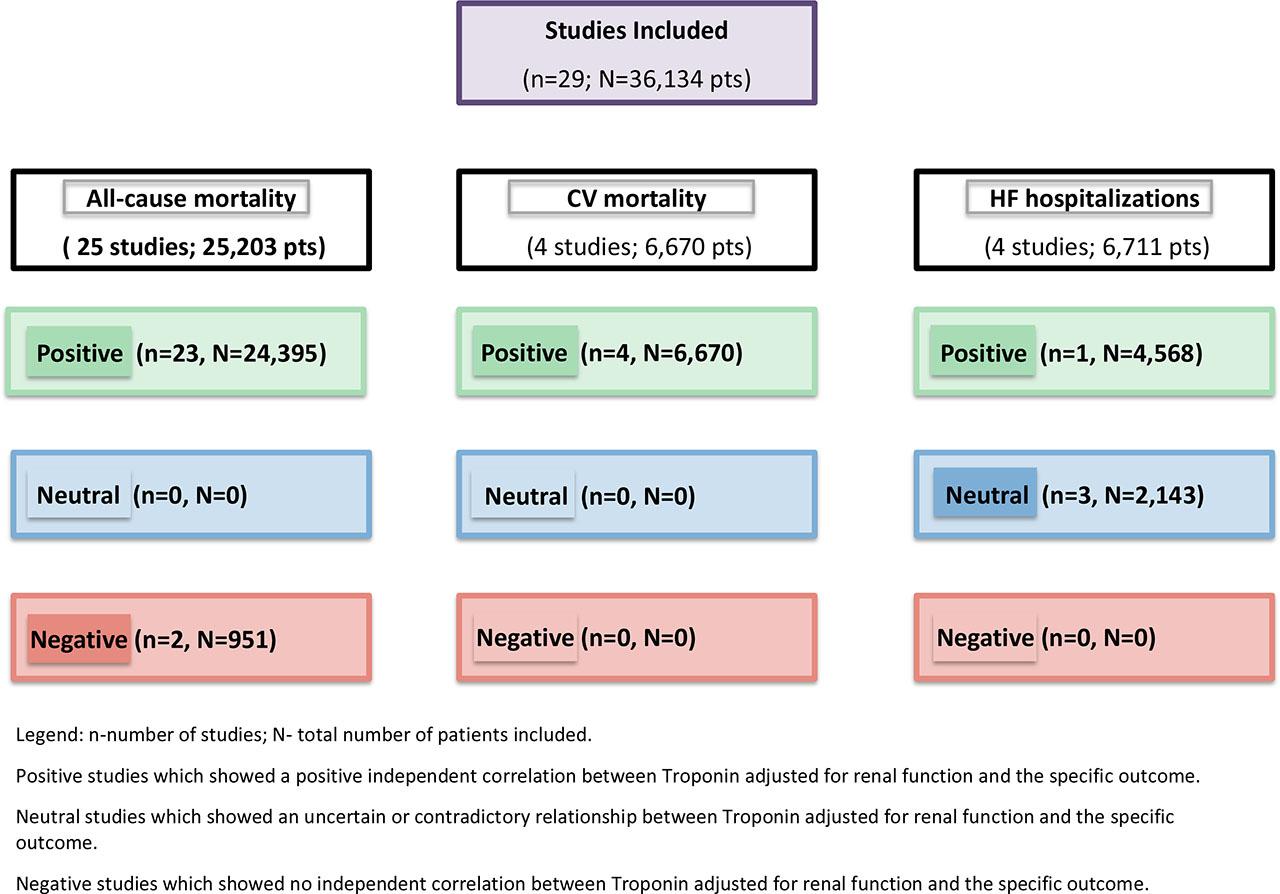
Studies divided according to their results.
Troponin levels serve as strong independent predictors of cardiovascular and all-cause mortality in heart failure patients after adjusting for renal function. Notably, renal dysfunction modifies the prognostic value of troponin, with the highest risk observed in patients displaying both elevated troponin levels and worsening renal function. In chronic heart failure (CHF) patients, elevated high-sensitivity troponin T (hs-cTnT) levels are particularly relevant as independent markers for all-cause mortality, regardless of renal function indices [32,34,53,35,36,38,39,45,48,49,52].
In acute heart failure (AHF), various troponin assays (hs-cTnT, hs-cTnI, conventional cTnT, and cTnI) demonstrate independent predictive capabilities for all-cause mortality across different follow-up periods. However, inconsistent findings emerge regarding their ability to predict in-hospital and long-term mortality when adjusted for scores like the NEWS2, as well as post-90-day mortality in ischemic heart failure [27,31].
Most studies indicate a lack of positive correlation between troponin levels and the risk of heart failure rehospitalization when stratified by renal function. While troponin reliably predicts mortality, its association with heart failure hospitalization remains weaker and inconsistent. This association improves when combined with markers of renal dysfunction, such as neutrophil gelatinase-associated lipocalin (NGAL), yet it may diminish in patients with severe renal impairment (eGFR <30 mL/min/1.73m2) [32].
Overall, the relationship between troponin levels and heart failure hospitalizations stratified by renal function remains complex and variable. Some studies suggest a potential correlation between elevated troponin T levels and increased rehospitalization risk, but these findings often lack statistical significance. Interestingly, troponin may have more pronounced predictive value in patients with declining renal function, as certain models suggest higher troponin levels could predict hospitalizations, although only up to a specific threshold of renal function [26,33,51,52]. Despite these potential associations, the evidence remains inconsistent, and troponin levels adjusted for renal function are not consistently reliable indicators of heart failure readmission risk.
A significant finding of this review is the robust association between elevated hs-cTnT levels and all-cause mortality; Jungbauer et al. noted that patients in the highest quartile had a hazard ratio (HR) of 2.6 for mortality after adjusting for renal function, illustrating the importance of troponin as a prognostic marker in heart failure management [32].
Furthermore, understanding the relationship between cardiac and renal functions is essential, as elevated troponin levels often indicate myocardial injury while also reflecting worsening renal function. For example, Tentzeris et al. demonstrated that higher hs-cTnT levels correlate with renal failure, underscoring the necessity of a comprehensive evaluation of both heart and kidney health [52].
Lastly, adjusting for renal function is crucial, as demonstrated by studies like those of Horiuchi et al. that confirm troponin levels maintain their significance as predictors of adverse outcomes even with renal impairment [50]. This emphasizes the importance of monitoring troponin in heart failure patients, particularly those with renal dysfunction, to provide insights into their overall risk.
Given its strong predictive value for mortality, troponin should be integrated into risk stratification models for patients with concurrent renal dysfunction. Future research should focus on exploring troponin-guided management strategies, refining treatment approaches, and ultimately improving clinical outcomes.
The sample sizes across studies varied significantly, potentially limiting the statistical power and reliability of findings in those with smaller populations. Additionally, the follow-up durations ranged widely, with shorter periods possibly missing long-term prognostic implications and longer studies risking bias from loss to follow-up. Furthermore, the heterogeneity of troponin assays — such as hs-cTnT, hs-cTnI, cTnI, and cTnT — and the use of different cut-off values further complicate comparisons and impact the overall consistency of the results.