
FIGURE 1.
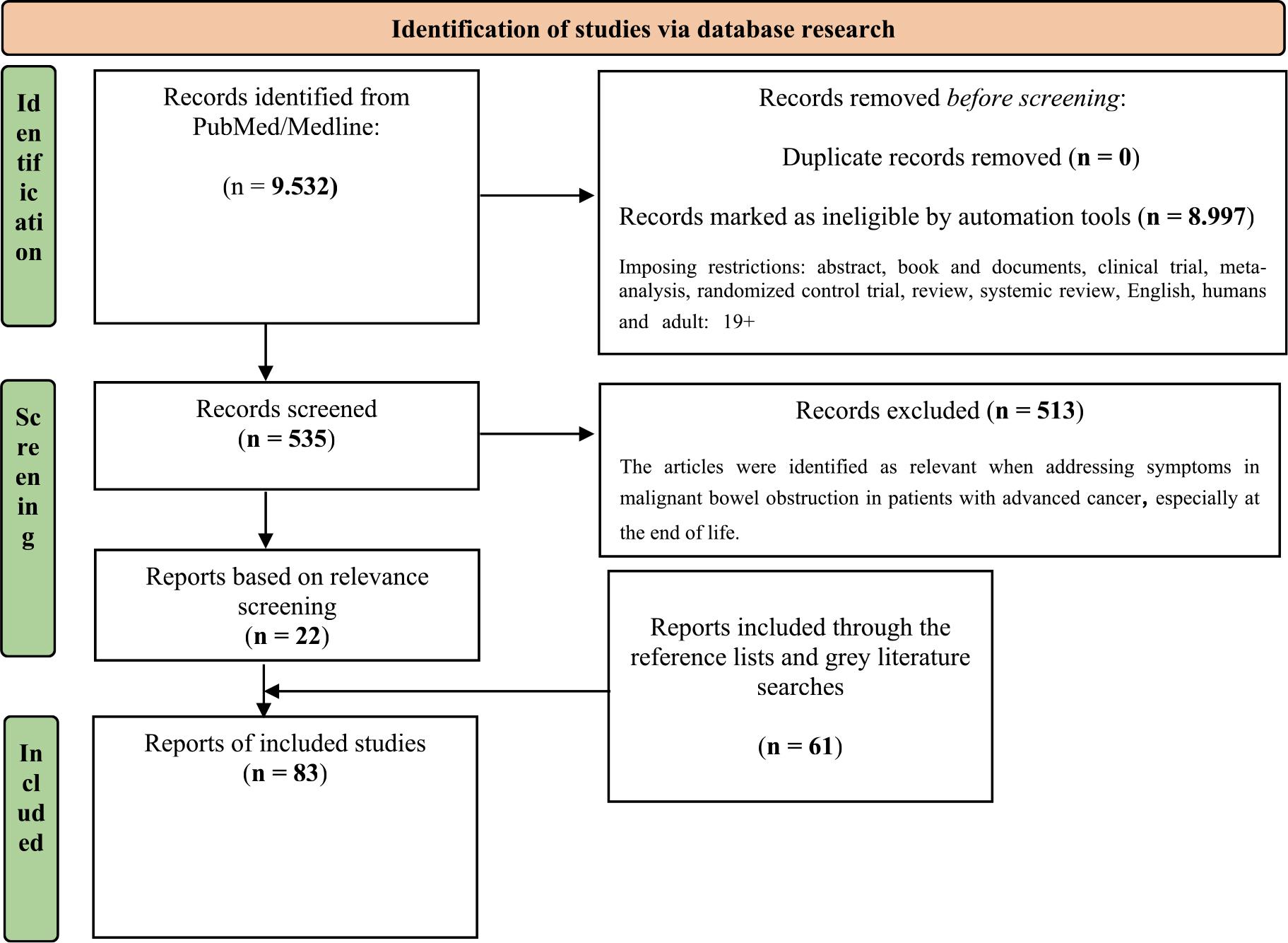
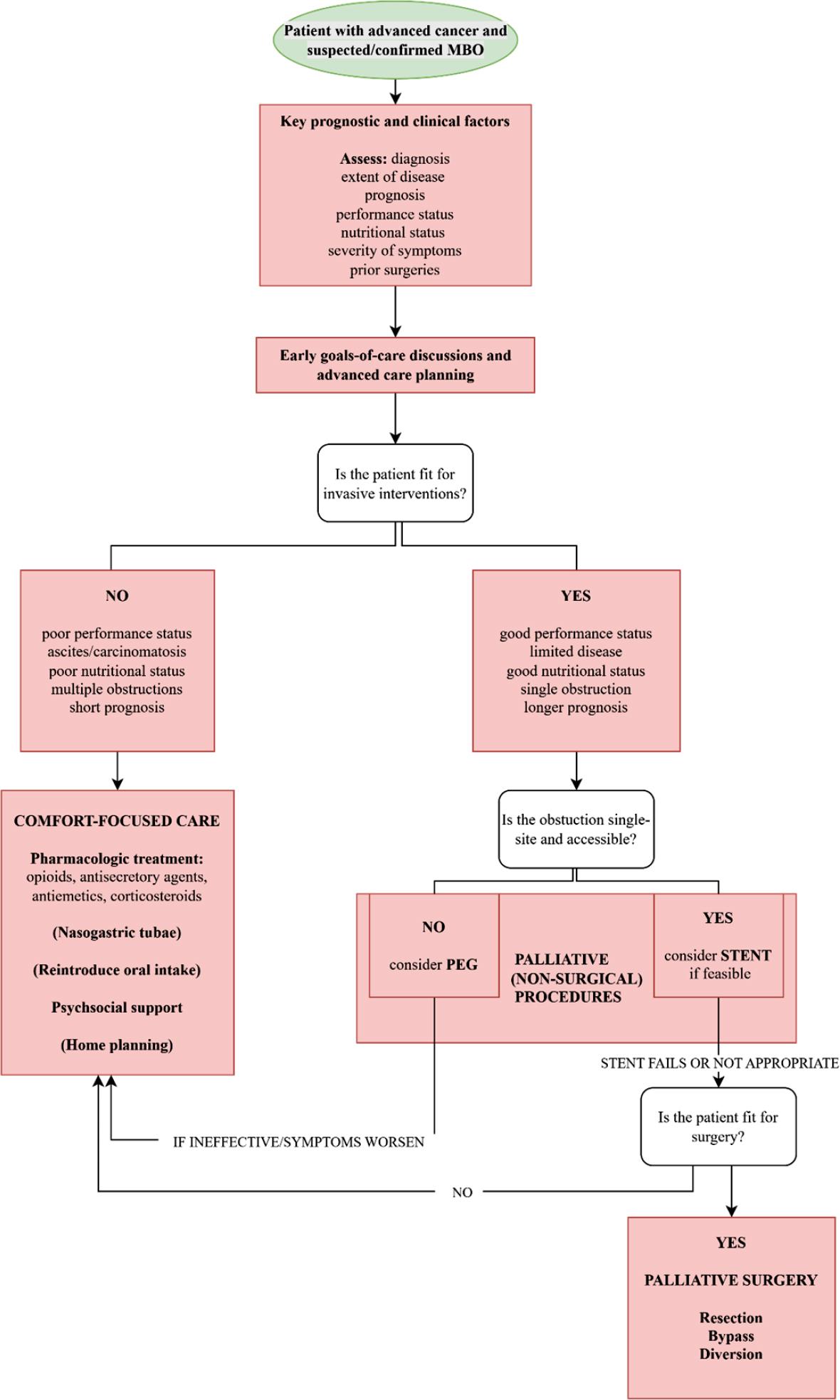
FIGURE 2.
Summary of suggestions for malignant bowel obstruction management, with associated level and grade of evidence10
| Nutrition | Level of evidence1 | Grade2 |
|---|---|---|
| At the initial diagnosis of MBO, patients should be placed nil per os. Once the obstruction has fully or partially resolved, a gradual, symptom-guided reintroduction of oral intake is recommended. This typically progresses from clear fluids to free or full fluids, followed by texture-modified low-fiber diets, and, if tolerated, a return to a normal-textured low-fiber diet. | IV | B |
| Nutrition interventions for patients with advanced cancer should be pursued only when the anticipated benefits for quality of life or survival clearly outweigh the associated risks. These decisions should be guided by a multidisciplinary team and include explicit discussions with patients and their caregivers about expected outcomes. | IV | B |
| Parenteral hydration has not been shown to prevent or alleviate symptoms such as thirst or dry mouth, nor does it prolong survival. When administered in excess, it may contribute to fluid overload and the development of peripheral or pulmonary edema. | III | B |
| Routine initiation of parenteral hydration is not recommended during the last days of life. | III | B |
| Home parenteral nutrition may provide benefit and help preserve quality of life in a carefully selected subset of patients with MBO. | IV | D |
| For home parenteral nutrition delivery central venous access is preferred. | III | B |
| At the end-of-life at home, parenteral nutrition should be discontinued (or not initiated) as it raises the risk of complications and may prolong suffering. | V | D |
Summary of recommendations for malignant bowel obstruction management, with associated level and grade of evidence_10 Level of evidence (Table 3), Grade (Table 4)
| Palliative (non-surgical) procedures | Level of evidence1 | Grade2 |
|---|---|---|
| Self-expanding metallic stents represent the preferred option for managing single-level large bowel obstruction, provided the procedure is technically achievable and there is no evidence of colonic perforation. | II | B |
Summary of the pharmacological treatment frequently used in malignant bowel obstruction
| Substance class | Drug | Remark |
|---|---|---|
| Analgesic | morphine | For pain – titrate or according to previous dosage |
| Corticosteroids | dexamethasone* | Peri-tumourous oedema reduction and anti-emetic effect |
| Somatostatine analagues | octreotide* | Reduction of gastrintestinal secrections |
| Anti-cholinergic | buthylscopolamine* | Reduction of gastrintestinal secrections |
| Prokinetic agent | metoclopramide | Drug of choice for incomplete obstruction; due to increased gastrointestinal motility, pain and vomiting may worsen; CAVE – for complete obstruction |
| Anti-psychotic | haloperidol* | Drug of choice for complete obstruction |
| levomepromazine* | ||
| olanzapine* | CAVE – elderly, patients with demetia | |
| Setrone | granisetron* | Increases constipation |
| H2 blocker | ranitidine* | |
| Proton pump inhibitor | omeprazole* |
Level of evidence_10 Level I and II are reccomendations, III-V suggestions
| Level | Criteria |
|---|---|
| I | Meta-analysis of multiple, well-designed, controlled studies; randomized trials with high power. |
| II | At least one-well designed experimental study; randomized trials with low power. |
| III | Well-designed, quasi-experimental studies (nonrandomized, controlled single-group, pretest-posttest comparison, cohort, time, or matched case-control series). |
| IV | Well-designed, non-experimental studies (comparative and correlational descriptive and case studies). |
| V | Case reports and clinical examples. |
Summary of suggestions for palliative surgery for malignant bowel obstruction management, with associated level and grade of evidence_10 Level of evidence (Table 3), Grade (Table 4)
| Palliative surgery | Level of evidence1 | Grade1 |
|---|---|---|
| For patients with multi-level obstruction, palliative surgical intervention may be appropriate in carefully selected cases. | IV | B |
| Patients with advanced cancer who undergo palliative surgery for MBO face a substantial risk of postoperative complications; therefore, less invasive surgical approaches should be considered whenever feasible. | IV | B |
Grade10
| Grade | Evidence needed |
|---|---|
| A | Type I or consistent findings from multiple studies of type II, III, or IV. |
| B | Types II, III, or IV and consistent findings. |
| C | Types II, III, or IV and inconsistent findings. |
| D | Little/no systematic empirical evidence. |
Summary of suggestions and recommendations for malignant bowel obstruction management, with associated level and grade of evidence10
| Intervention | Level of evidence1 | Grade2 |
|---|---|---|
| Anti-emetics | ||
| Anticholinergics (e.g., hyoscine butylbromide) are generally less effective than octreotide for reducing vomiting in MBO. | III | D |
| Haloperidol demonstrates anti-emetic efficacy, particularly in complete MBO. | IV | B |
| Dopamine antagonist prokinetic drugs (metoclopramide) may be beneficial in partial MBO but is generally contraindicated in complete MBO due to the risk of perforation. | III | B |
| Histamine H1 antagonists, (e.g., dimenhydrinate, cyclizine) show utility in nausea and vomiting reduction in complete MBO. | IV | D |
| Phenothiazines (e.g., chlorpromazine) may be usful anti-emetics in MBO. | IV | D |
| Granisetron, serotonin (5HT3) antagonist may decrease nausea and vomiting in MBO. | III | D |
| Somatostatin analog (octreotide, lanreotide) may decrease vomiting in MBO. | I | A |
| Thienobenzodiazepene antipsychotic (e.g., olanzapine) may provide benefit in reducing nausea and vomiting in MBO. | I | A |
| Analgesics | ||
| Although there is no evidence of support, opioids are commonly used to treat pain associated with MBO. | V | D |
| Anticholinergics (hyoscine butylbromide) may be effective in abdominal pain reduction in MBO. | III | D |
| Corticosteroids | ||
| Steroids may reduce acute symptoms of MBO and be used for short-term benefits. | III | B |
| Bowel decompression | ||
| Nasogastric tube may be temporary used for decompression in acute MBO. | V | D |
| Endoscopic or percutaneous gastrostomy tube may help in gastric decompression in MBO. | IV | B |
| Percutaneous transesophageal gastro-tubing may be help in gastric decompression in MBO. | IV | C |