FIGURE 1.
FIGURE 2.
FIGURE 3.
FIGURE 4.
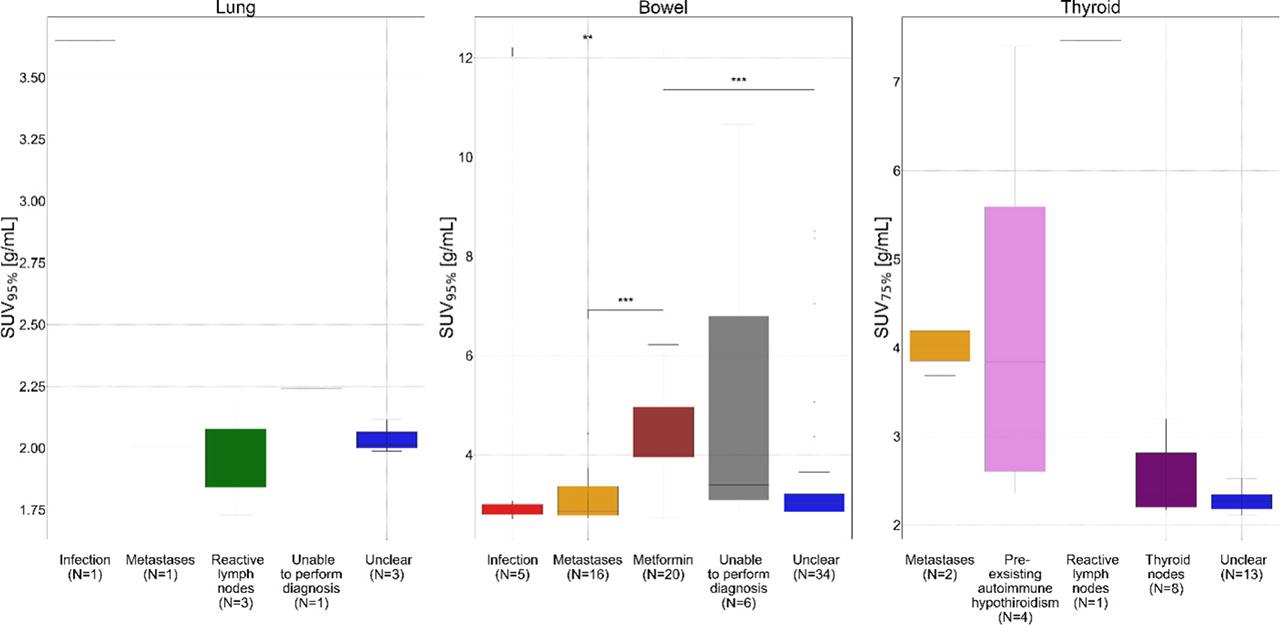
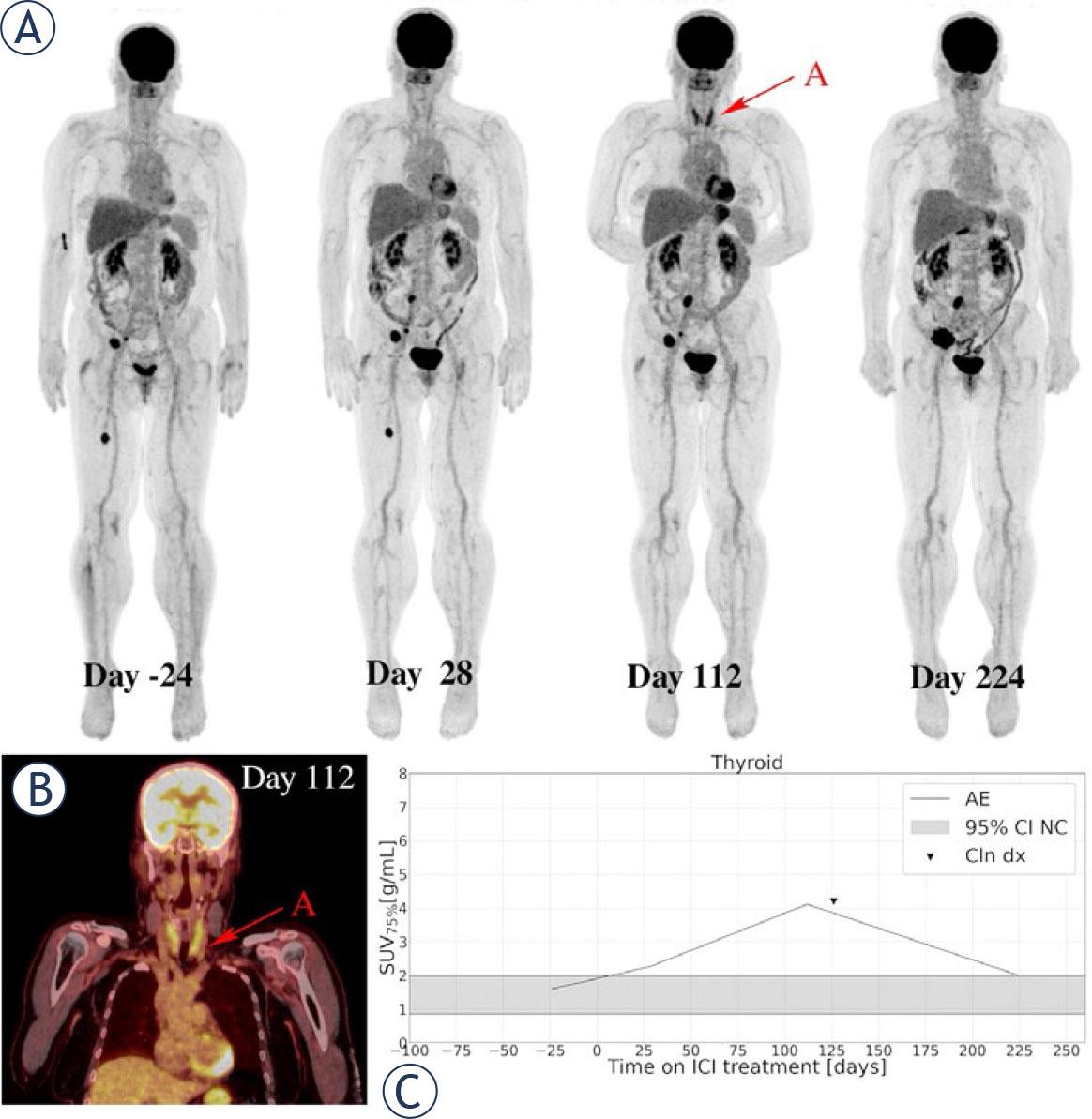
FIGURE 5.
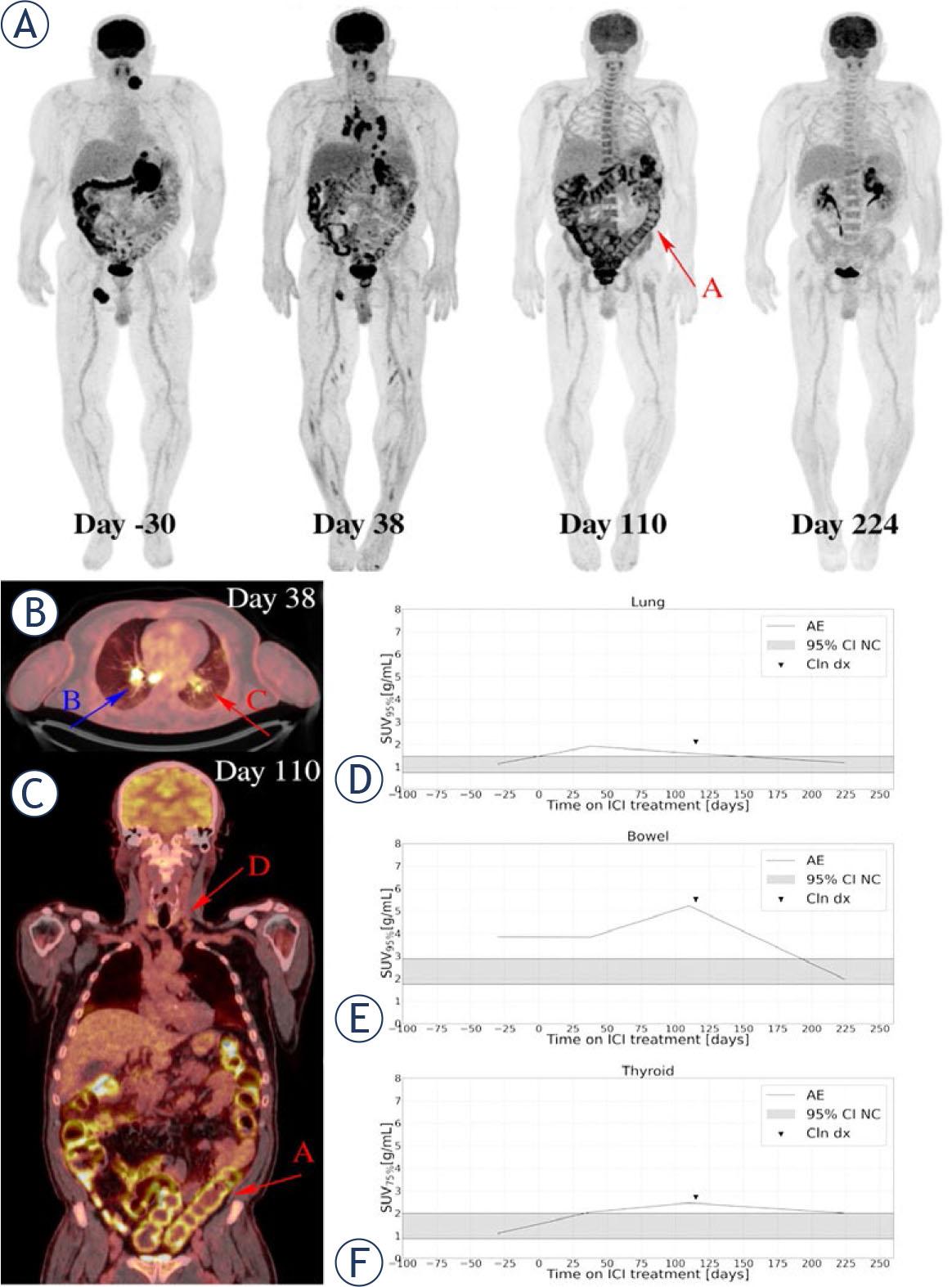
FIGURE 6.
Clinical diagnosis of immune-related adverse events
| irAE | Any Grade No (%) | Grade 3–5 No (%) | Time to onset of irAE (mean ± SD) [days] |
|---|---|---|---|
| irPneumonitis | 3 (4) | 0 | 104 ± 58 |
| irColitis | 4 (6) | 2 (3) | 101 ± 34 |
| Hypothyroidism | 10 (14) | 0 | 91 ± 40 |
| Hyperthyroidism | 7 (10) | 0 | 51 ± 50 |
Timing of 18F-FDG PET/CT relative to immune-checkpoint inhibitors (ICI) treatment initiation
| Number of patients | Range (min–max) (days) | Mean (days) | Median (days) | SD (days) | |
|---|---|---|---|---|---|
| Pre-Treatment | 71 | [−44, −1] | −16 | −16 | 10 |
| W4 (28 days) | 68 | [21, 62] | 34 | 34 | 7 |
| W16 (112 days) | 55 | [105,150] | 115 | 112 | 8 |
| W32 (224 days) | 48 | [196,280] | 226 | 224 | 12 |
Patient characteristics
| Characteristics | Count (proportion %) | |
|---|---|---|
| Number of patients | Total | 71 (100) |
| Age; mean (+/−sd) (yr) | 62 (12) | |
| Gender | Male | 43 (61) |
| Female | 28 (39) | |
| ECOG performance status | 0 | 30 (42) |
| 1 | 41 (58) | |
| AJCC | III.D | 1 (1) |
| M1a | 16 (23) | |
| M1b | 10 (14) | |
| M1c | 32 (45) | |
| M1d | 12 (17) | |
| Anatomic site of primary | Cutaneous | 58 (82) |
| Ocular | 4 (6) | |
| Mucosal | 3 (4) | |
| Unknown primary | 6 (8) | |
| Prior radical treatment | Surgical resection | 38 (54) |
| Surgical resection + adjuvant RT | 7 (10) | |
| Surgical resection + adjuvant RT + adjuvant ICI | 4 (6) | |
| Surgical resection + adjuvant RT + adjuvant TKI | 2 (3) | |
| Surgical resection + adjuvant TKI | 2 (3) | |
| Surgical resection + adjuvant interferon alpha | 2 (3) | |
| None | 16 (23) | |
| Line of systemic treatment for metastatic disease | 1st line | 63 (89) |
| 2nd line | 8 (11) | |
| Baseline LDH | Elevated | 22 (31) |
| Normal | 49 (69) | |
| Actionable mutation | BRAF wild type | 21 (30) |
| BRAF V600E | 28 (39) | |
| BRAF V600K | 10 (14) | |
| BRAF V600 - others | 1 (1) | |
| NRAS | 11 (16) | |
| Type of systemic treatment | PD-1 inhibitors | 47 (66) |
| Combination of PD-1 and CTLA-4 inhibitors | 24 (34) |