
FIGURE 1.
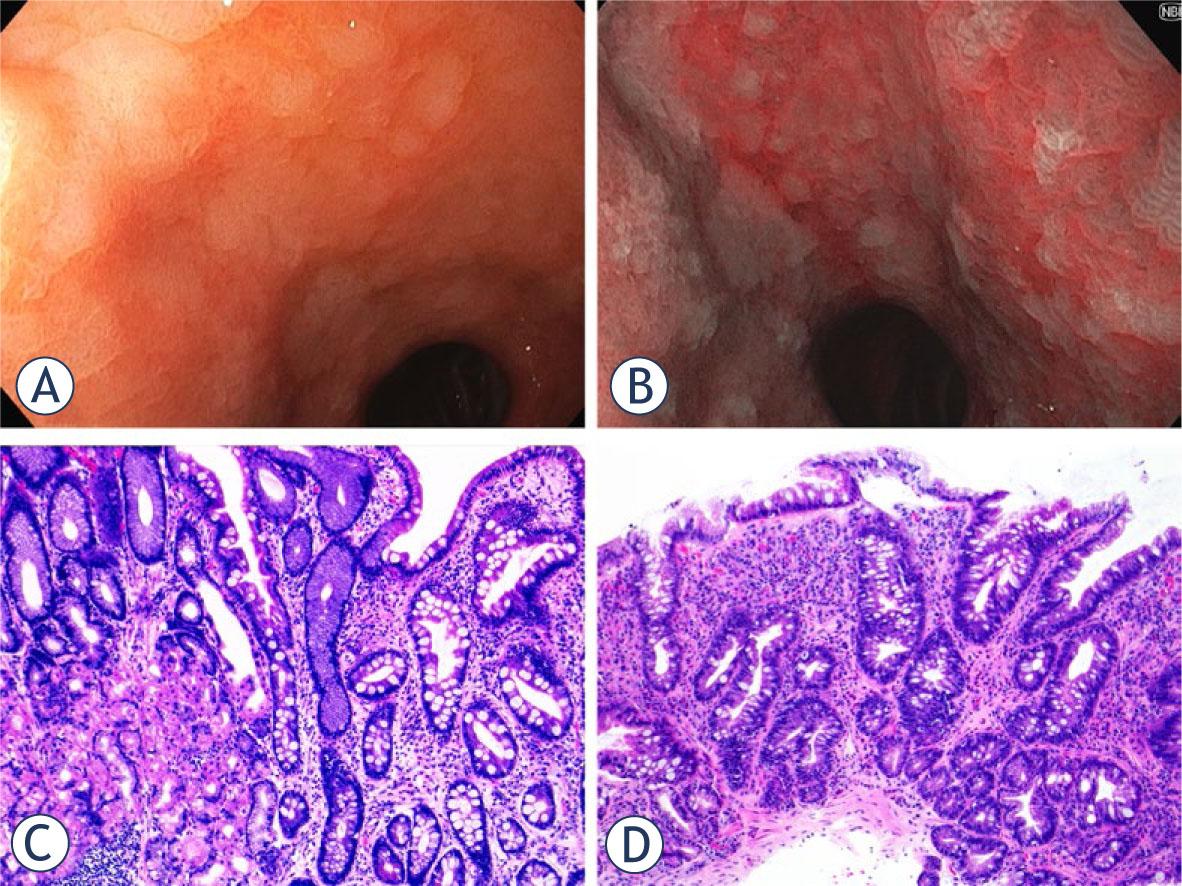
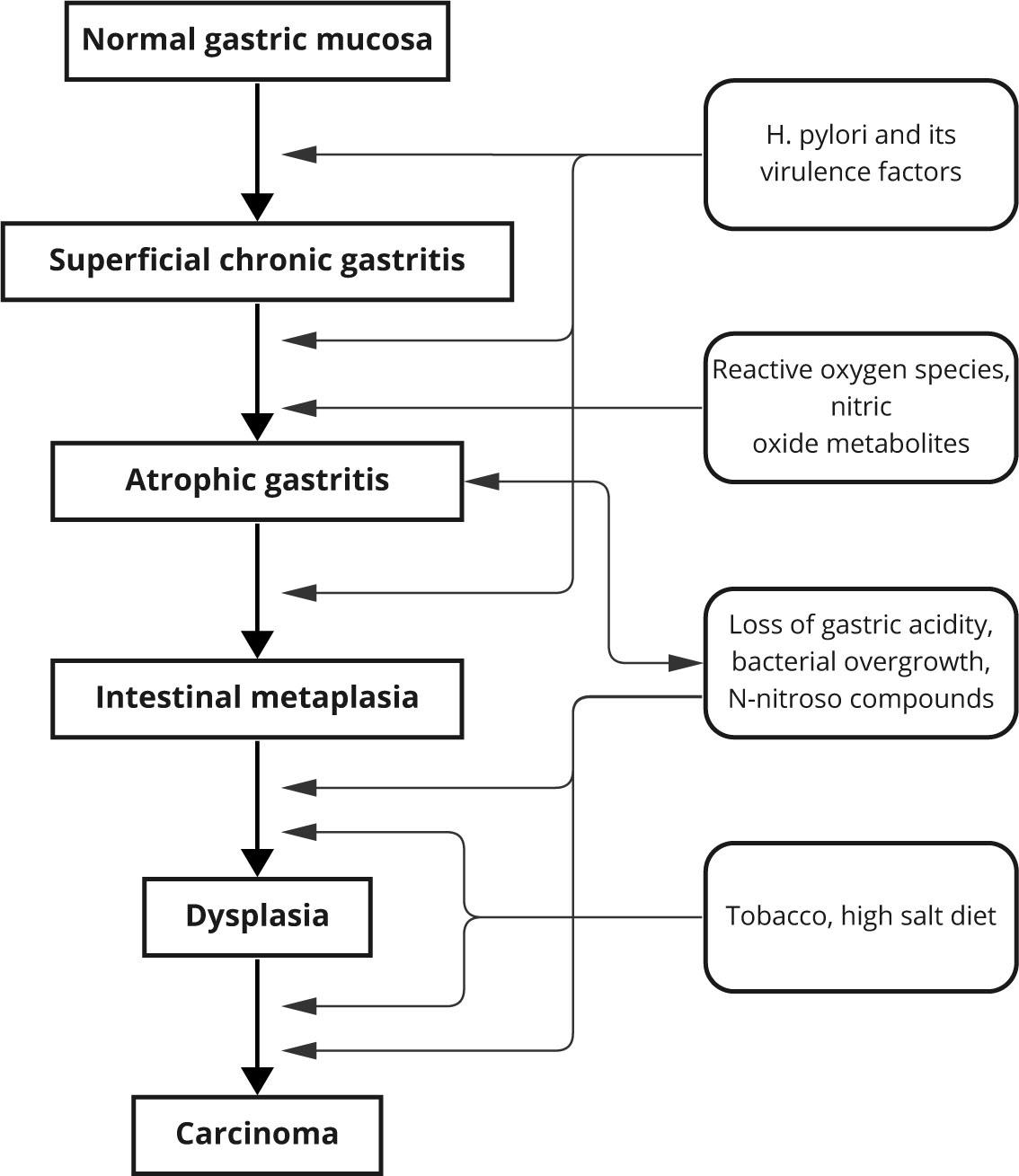
FIGURE 2.
Patients’ related predictive risk factors for gastric intestinal metaplasia
| Risk Factor | Odds ratio (OD) | Key findings | References |
|---|---|---|---|
| Race | |||
| White | 1 | Hispanic and Asian patients have an increased risk for GIM | Tan MC et al. (2022)94 |
| Asian | 2.83–3 | Akpoigbe K et al. (2022)95 | |
| Hispanic | 2.10–5.6 | ||
| Age (> 50 years) | 1.5–2.03 | Risk increases with age, possibly due to accumulated exposure to risk factors. | Aumpan N et al. (2021)96 |
| Tan MC et al. (2020)97 | |||
| Male gender | 1.55–2.09 | Probably due to genetics and exposure to other risk factors | Aumpan N et al. (2020)98 |
| Leung WK et al. (2005)99 | |||
| Chronic gastritis | 3.68–5.76 | Chronic inflammation is leads to IM. | Yoo YE et al. (2013)100 |
| Tatsuta M et al. (1993)101 | |||
| H. pylori infection | 2.47–3.65 | Strong correlation with IM, especially with CagA positive strains. | Aumpan N et al. (2021)96 |
| Nguyen T et al. (2021)102 | |||
| Family history of gastric cancer | 1.5–3.8 | Patients with a first-degree relative with gastric cancer have an increased risk of neoplastic progression | Nieuwenburg SAV et al. (2021)103 |
| Reddy KM et al. (2006)104 | |||
| Alcohol consumption | 1.27–1.54 | Alcohol intake was independently associated with increased risk of developing AG and IM | Holmes HM et al. (2021)105 |
| Kim K et al. (2020)106 | |||
| Tobacco smoking | 1.54–2.75 | Tobacco smoking is a risk factor for gastric IM. | Morais S et al. (2014)107 |
| Thrift AP et al. (2022)108 | |||
| Blood group A | 1.39–1.42 | Blood group A is associated with higher risk of GIM | Mao Y et al. (2019)109 |
| Rizatto C et al. (2013)110 | |||
| Bile reflux | unknown | Bile acids not only interefere with gastric mucosa but also regulate multiple carcinogenic pathways | Wang M et al. (2023)111 |
| Yu J et al. (2019)112 | |||
| Salt consumption | 0.37–1.53 | Salt intake may increase progression to advanced gastric precancerous lesions | Dias-Neto M et al. (2010)113 |
| Song JH et al. (2017)114 | |||
| Industrially processed food | unknown | Dietary exposure to N-nitroso–containing compounds has been shown to increase the promotion of gastric carcinogenesis | Wiseman M (2008)115 |
| Jencks DS et al. (2018)116 | |||