
Cardiovascular diseases remain the leading cause of mortality worldwide, accounting for more than one-third of all global deaths, with a disproportionately higher impact in low- and middle-income countries.1 Acute coronary syndrome (ACS) is often the first clinical manifestation of cardiovascular disease, and ST-elevation myocardial infarction (STEMI) represents one of the most severe forms, continuing to pose a major challenge to emergency medical systems. Over the past decades, the widespread adoption of early reperfusion strategies, including primary percutaneous coronary intervention (PCI) and fibrinolysis, has resulted in a substantial reduction in STEMI-related mortality. However, significant regional differences persist, with in-hospital mortality rates ranging from 3% to 12%.2,3 This declining trend has also been observed in Romania since 2010, coinciding with the national implementation of the RO-STEMI program.4 Regardless of the reperfusion strategy, total ischemic time remains a key determinant of infarct size, left ventricular dysfunction, and survival.5
ACS registries have been developed in recent years in line with the guidelines of the European Society of Cardiology (ESC) to evaluate their implementation in clinical practice. Despite clear recommendations, real-world registries remain essential tools for assessing quality of care. Ideally, every emergency university hospital should aim to develop ACS registries as part of standard patient care. Contemporary ESC guidelines emphasize rapid diagnosis, early activation of emergency medical services, and timely myocardial reperfusion as key quality indicators in STEMI management.1 While door-to-balloon times have improved considerably in PCI-capable centers, pre-hospital delays related to patient behavior and system organization remain highly variable across Europe.2,3
In Eastern European countries, including Romania, STEMI outcomes remain less favorable than in Western Europe, despite the implementation of the national RO–STEMI program, which has significantly expanded access to primary PCI and reduced mortality.4 However, comprehensive real-world data evaluating residual reperfusion delays and system-level barriers continue to be limited. The present study aims to characterize reperfusion timelines, clinical profiles, and in-hospital outcomes of patients with STEMI treated in a tertiary emergency hospital in Romania, with particular emphasis on identifying modifiable sources of delay.
This retrospective observational study included 151 consecutive patients aged ≥18 years diagnosed with STEMI who presented within 24 h of symptom onset and were admitted between April and October 2025 to the Dr. Carol Davila Central Military Emergency University Hospital, Bucharest. A local Acute Coronary Syndrome registry was established. Data were collected on demographic characteristics, cardiovascular risk factors, clinical presentation, infarct localization, left ventricular function, reperfusion strategy, reperfusion time intervals, and in hospital outcomes.
Reperfusion time intervals were defined as follows: pain-to-call (time from symptom onset to emergency call), call-to-first medical contact (FMC), FMC-to-door (time from FMC to arrival at the PCI-capable center), and door-to-balloon (time from hospital arrival to balloon in flation).
Statistical analysis was performed using SPSS v.26.0 (IBM). Continuous variables were tested for normality using the Shapiro–Wilk test. Normally distributed variables are presented as mean ± s.d., whereas non-normally distributed variables are presented as median and interquartile range (IQR). Categorical variables are expressed as counts and percentages. Given the descriptive and exploratory nature of this registry analysis, between-group comparisons are reported without formal hypothesis testing.
Of the 151 patients included, 69.5% were male, with a mean age of 61.8 ± 13.8 years. The most prevalent cardiovascular risk factors were hypertension (67%), dyslipidemia (68%), overweight or obesity (70%), smoking (55%), and diabetes mellitus (28%). At presentation, 69% of patients were classified as Killip class I, while 12% presented with advanced heart failure or cardiogenic shock (Killip III–IV).
Anterior STEMI accounted for 55.8% of cases, followed by inferior STEMI in 37.2%. Left ventricular ejection fraction was <40% in 41.4% of patients at admission.
A key finding relates to the mode of presentation to the emergency department (Figure 1). One-third of patients (n = 52, 33.77%) were transferred from regional non-PCI-capable hospitals. The largest proportion (n = 67, 44.37%) was transported directly to our hospital by the Bucharest emergency medical services (EMS). A smaller group (n = 26, 17.22%) was initially transported to a non-PCI-capable hospital within Bucharest and subsequently transferred, while a minority (n = 7, 4.64%) were self-presenters (six from Bucharest and one from a nearby city).
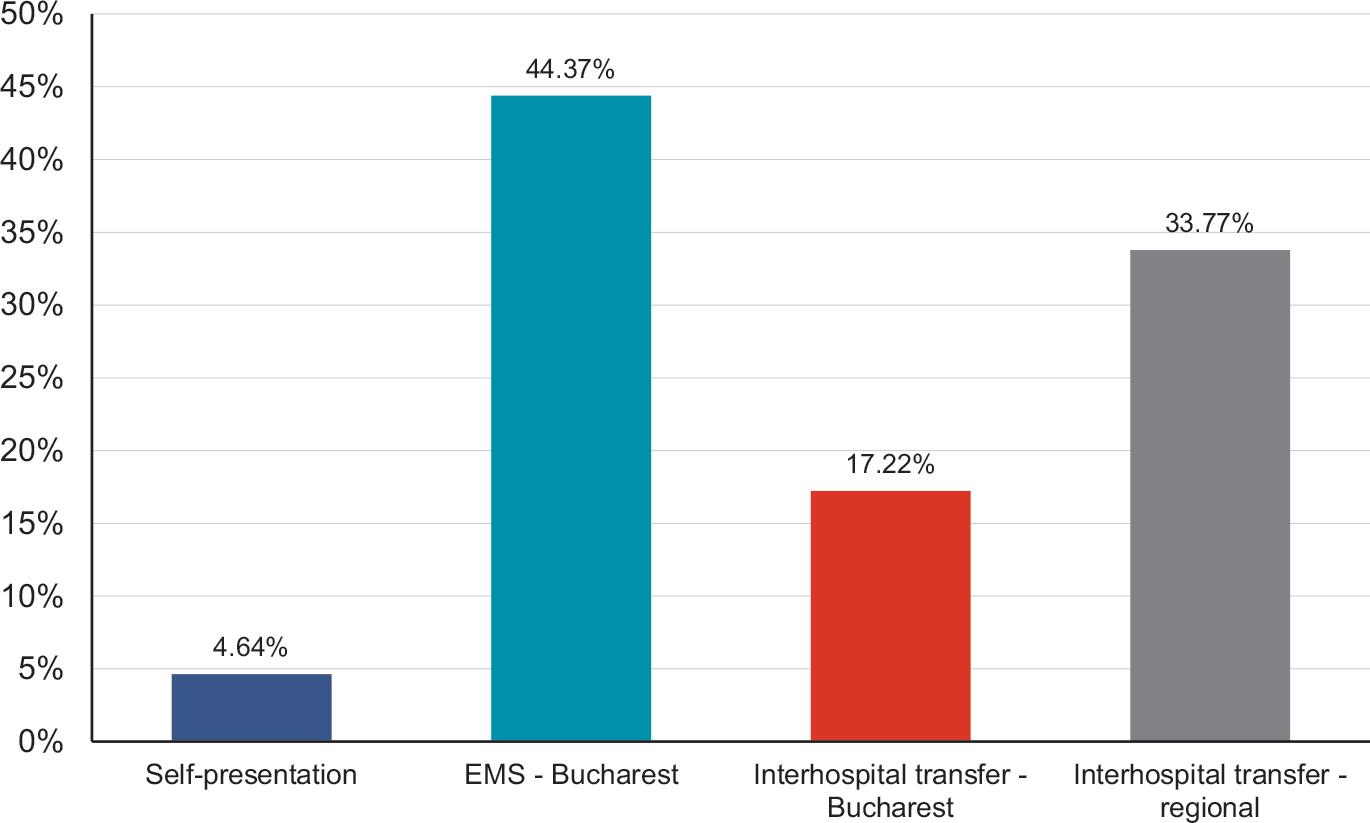
Presentation to the emergency department.
The median pain-to-call interval was 180 min (IQR 30–250), with a mean of 229 ± 424.7 min, reflecting the right-skewed distribution of pre-hospital delay times. The mean call-to-FMC, FMC–to–door, and door-to-balloon intervals were 46 ± 29.7 min, 102 ± 68.9 min, and 44 ± 19.6 min, respectively. The median total ischemic time was 370 min (IQR 220–530), with a corresponding mean of 421 ± 262.3 min.
Primary PCI was the dominant reperfusion strategy, while fibrinolytic therapy prior to transfer was administered in only 5.23% of cases. In-hospital mortality was 8.94%.
Reperfusion time intervals were compared between patients from Bucharest and those referred from regions assigned to Bucharest PCI centers. Patients from outside Bucharest experienced longer system-related delays, with call-to-FMC intervals of 51 ± 21 min vs. 29 ± 12 min, FMC–to–door intervals of 129 ± 28 min vs. 32 ± 11 min, and total ischemic time of 455 ± 119 min vs. 327 ± 77 min. In contrast, pain-to-call (232 ± 64 min vs. 221 ± 43 min) and door-to-balloon times (43 ± 9 min vs. 44 ± 10 min) were similar between groups.
This registry-based analysis provides clinically relevant insights into STEMI care within the current framework of the emergency healthcare system for ACS in Romania. The demographic characteristics of our cohort are consistent with those reported in major European registries, such as FAST-MI and ALKK, supporting the validity of our findings.6,7 Nevertheless, the high prevalence of modifiable cardiovascular risk factors highlights persistent gaps in primary prevention.
The reported in-hospital mortality of 8.94% was not stratified according to Killip class, reperfusion strategy, or infarct localization, which represents a limitation of the present analysis. However, this figure should be interpreted in the context of the relatively high-risk profile of the study population, with 12% of patients presenting in Killip class III–IV and 41.4% having reduced left ventricular ejection fraction at admission, suggesting that the observed mortality is consistent with the clinical severity of the cohort.
One of the most striking findings of this study is the markedly prolonged total ischemic time, exceeding 7 h on average. This observation is consistent with reports from other European healthcare systems with less optimized emergency networks and is strongly associated with adverse clinical outcomes.5,8 Patient-related delay, reflected by prolonged pain-to-call time, remains the dominant contributor to total ischemic time and likely reflects insufficient symptom awareness and delayed activation of emergency medical services, highlighting the need for sustained public education campaigns on chest pain recognition and response at the individual, familial, and community levels.9
System-related delays during the pre-hospital and inter-hospital phase further increase the ischemic burden. Geographic dispersion, inter-hospital transfer requirements, and variability in ambulance availability remain key challenges in regional STEMI networks. In contrast, once patients reached the PCI-capable center, in-hospital workflows were largely compliant with ESC-recommended door-to-balloon time targets, indicating efficient coordination between the emergency department, cardiology ward, and catheterization laboratory.1
The very low utilization of fibrinolytic therapy prior to transfer highlights the underuse of pharmaco-invasive strategies in settings where timely primary PCI cannot be achieved. Evidence from randomized trials indicates that early fibrinolysis followed by planned PCI can reduce ischemic time and improve clinical outcomes in such scenarios.10
Collectively, these findings underscore the need for an integrated national strategy combining public education initiatives, optimization of emergency medical service pathways, expansion of pharmaco-invasive protocols, and continuous registry-based quality monitoring.
This study has several limitations, including its singlecenter design and relatively small sample size. Symptom onset times were patient-reported and may therefore be subject to recall bias.
Another limitation relates to the specific referral pattern of this tertiary emergency hospital. Although the center also serves military personnel and their families, it is fully open to and routinely manages civilian emergency cases. As such, the findings are more likely to reflect the characteristics of the Bucharest urban STEMI network rather than nationwide patterns.
Additionally, long-term outcomes after hospital discharge were not available.
Despite these limitations, the study identifies clear and actionable targets for improvement. Reducing pre-hospital delays through structured public education campaigns, optimizing inter-hospital transfer protocols, and reinforcing guideline-based use of pharmaco-invasive reperfusion strategies may significantly improve STEMI outcomes in Romania and similar healthcare settings.
STEMI care in Romania is characterized by substantial pre-hospital delays despite efficient in-hospital reperfusion workflows. Addressing both patient- and system related delays represents the primary opportunity to reduce ischemic time and improve survival in this high-risk population.