
Commotio cordis (CC), or concussion of the heart, is typically characterized by a sudden impact to the chest wall precipitating ventricular fibrillation arrest. There have been very few documented cases of atrial fibrillation (AF) resulting from this mechanism.1–3 A relative consensus exists in the crucial nature of the timing of a blow at the vulnerable ventricular repolarization in the cardiac cycle, with suggestion of the impact occurring during atrial repolarization, triggering paroxysmal AF.4
Previous cardiac arrest algorithms from the American Heart Association (AHA) began with a “precordial thump” to the chest wall of a patient in ventricular fibrillation in witnessed arrest. This recommendation persisted even through the AHA’s resuscitation guidelines in conjunction with the International Liaison Committee on Resuscitation published in 2005.5 Although this maneuver is no longer generally recommended due to its haphazard reliability and wider availability of the automated external defibrillator, the mechanism whereby this recommendation arose is rooted in physics: conversion of mechanical pulse-pressure energy to electrical energy and depolarization in the cardiac myocyte, thereby restoring rhythm. This is intuitive based on the fundamental electromechanical coupling of the heart. This mechanical-to-electrical energy conversion, if timed correctly, may restore a normal rhythm, or it may trigger a lethal arrhythmia in an otherwise healthy patient. Enter CC.
CC is a rare, cardiac arrest-causing incident occurring after an impact to the chest that does not cause structural damage to the heart.4 Since the creation of the Commotio Cordis National Registry in 1995, a total of 224 cases has been reported, and for the first 15 years, there were an average of 15 cases annually.6 It is more common in the young participants of contact sports, with an average age incidence around 15 years and a men-to-women ratio of over 9:1.6 This predilection for men has been postulated by several sources to result simply from male predominance in contact sports.
Although this is likely a large contributing factor, it has also been proposed there may be a genetic channelopathy component, similar to the well-known Long-QT and Brugada syndromes.5,7 The exact mechanism has been extensively studied in animal models and requires two components: traumatic impact to the chest wall directly over the ventricles with projectile velocity fast enough to induce ventricular arrhythmia, without causing physical damage (30–50 mph); and timing of the strike in a 15-ms window of the cardiac cycle prior to the peak of the T-wave.5,8 To decrease morbidity and mortality, the most important management of this condition is immediate defibrillation performed within the first 3 minutes of cardiac arrest.9 Awareness for this condition in addition to increased efficiency and reliability of automated external defibrillators have greatly improved survival post return of spontaneous circulation from 10% in the two decades following 1970, to nearly 58% in recent years (2006–2012).9
By traditional definition, the ECG finding associated with CC is ventricular fibrillation, yet there have been reports of AF induced by the same concussive force to the heart, although all with spontaneous resolution.1–3 As an increasing number of cases are being documented in recent years by the same mechanism as CC with differing arrhythmogenic results, more collectively these may be referred to as “commotio cordis-like events” (CCLEs) for clarification. This allows for the discussion of the same mechanism of injury, found in similar circumstances with differing results, depending on the precise moment the blow occurs in the cardiac cycle. This mode of injury and its mixed arrhythmogenic results at various points in the cardiac cycle were studied extensively by Link et al. in their 2001 animal trials, showing multiple foci of irritability, both atrial and ventricular, depending on the area struck and timing.10
Here, we present a case of subsequent CCLEs in a young male patient with possible atrial injury and delayed development of AF.
A 17-year-old, previously healthy male patient presented to the emergency department after being struck over the anterior chest by the helmet of an opposing player during a high school football game. He reported sharp, sternal chest pain that worsened with movement and deep inspiration, describing the sensation as “having the wind knocked out [of me].” He denied palpitations, syncope, or dizziness.
On scene, emergency medical services noted a sinus bradycardia with ventricular bigeminy on the rhythm strip. Vital signs were notable only for bradycardia of 50 beats per minute (bpm). On examination, he appeared uncomfortable and had reproducible tenderness to palpation over the sternum and left parasternal region. Cardiac examination revealed bradycardia and an irregular rhythm without murmurs, rubs, or gallops. Peripheral perfusion was normal, and pulses were symmetric.
A 12-lead ECG showed sinus rhythm with frequent premature ventricular complexes (PVCs) and marked rhythm irregularity, including occasional premature atrial contractions (Figure 1). High-sensitivity troponin was mildly elevated at 17 ng/L (>14 ng/L). A computed tomography (CT) scan of the chest with i.v. contrast was obtained and showed no evidence of structural injury or vascular abnormality. Pediatric cardiology was consulted in the emergency department. Given the concerning arrhythmic pattern and mechanism of injury, the patient was advised to refrain from participating in sports and instructed to follow up with outpatient cardiology for further evaluation. He wore a Holter monitor for 24 h, after which he was cleared from further investigation and able to resume sports activities.
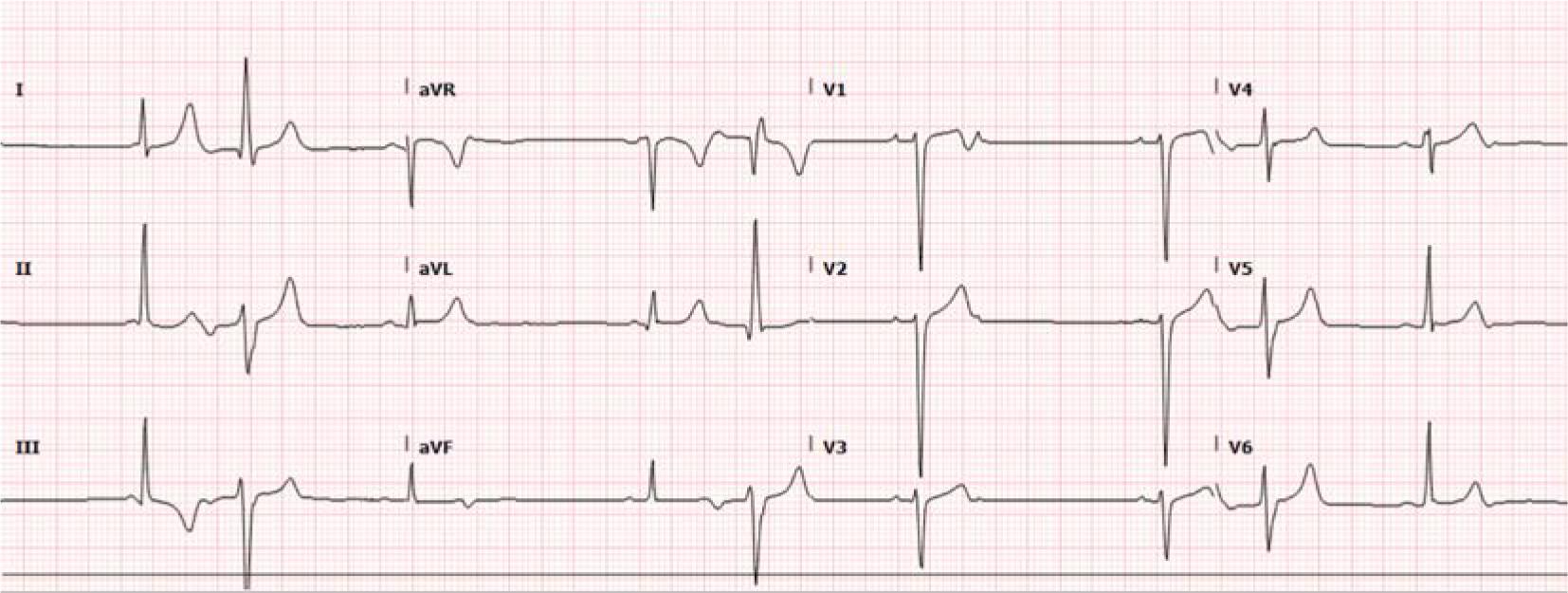
First presentation to emergency department.
The patient presented to the same emergency department 8 months later via ambulance after a bench press mishap caused a bar loaded with 405 pounds to strike his chest. He was complaining of chest pain and exquisite tenderness on deep inspiration, causing him to splint his respirations. His ECG displayed a sinus bradycardia at 40 bpm with multifocal and frequent PVCs. Heart rate noted on the cardiac monitor dropped as low as the mid-30s, though his blood pressure remained stable. When compared to his previous ECG, the similarities were striking (Figure 2). A bedside limited ultrasound did not demonstrate any pericardial effusion, pneumothorax, or wall motion abnormality.
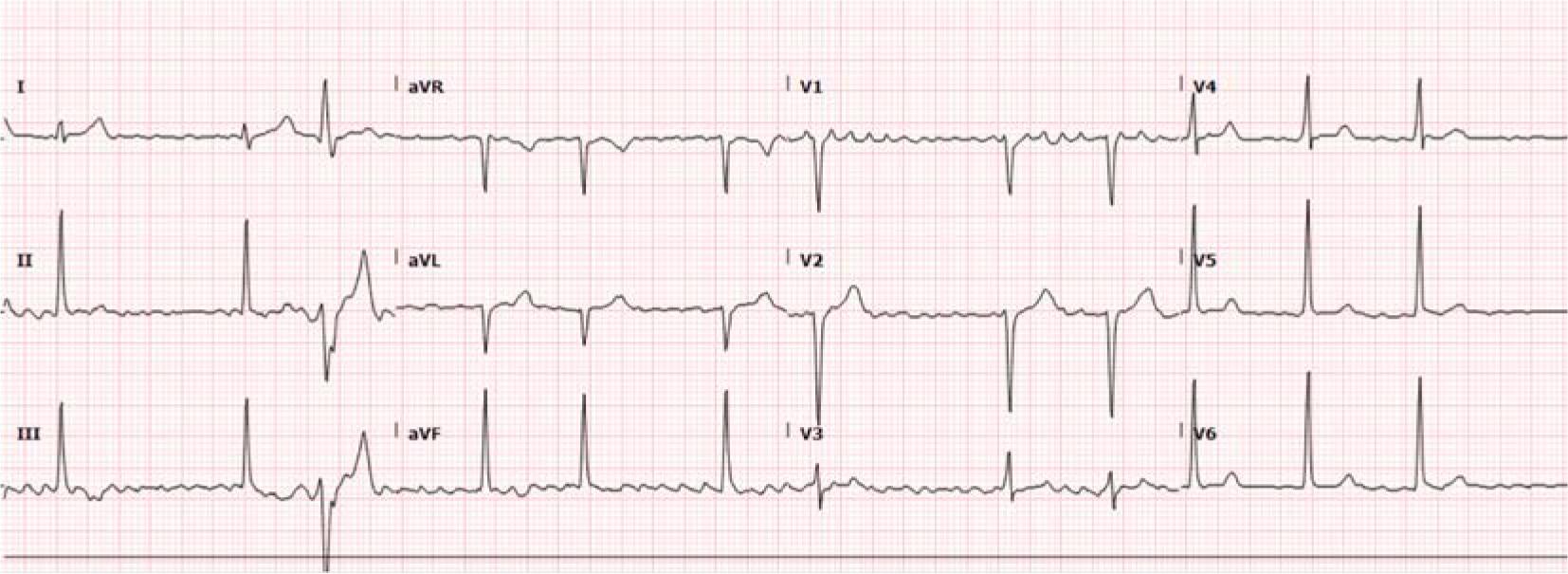
Second presentation to emergency department.
Vital signs were blood pressure 122/73 mmHg, pulse 58 bpm, respirations 18 per min, temperature 36.5 °C, SpO2 98% on room air. Chest x-ray did not demonstrate any rib fractures. Initial high-sensitivity troponin was 20 ng/L (>14 ng/L) and peaked at 23 ng/L. Pediatric cardiology was consulted, and a stat echocardiogram was performed, which did not demonstrate any wall motion abnormalities or valvular damage. The chest CT was unremarkable.
The patient was admitted to the trauma intensive care unit and subsequently developed paroxysmal AF without rapid ventricular response on day 3 of admission (Figure 3). Cardiology recommended 24 h of amiodarone drip for chemical cardioversion, but he remained in AF. The patient was transitioned to oral dronedarone 400 mg twice daily, and chemical cardioversion was achieved within 12 h, with restoration of normal sinus rhythm. He was discharged the next day on dronedarone and given follow-up with electrophysiology.
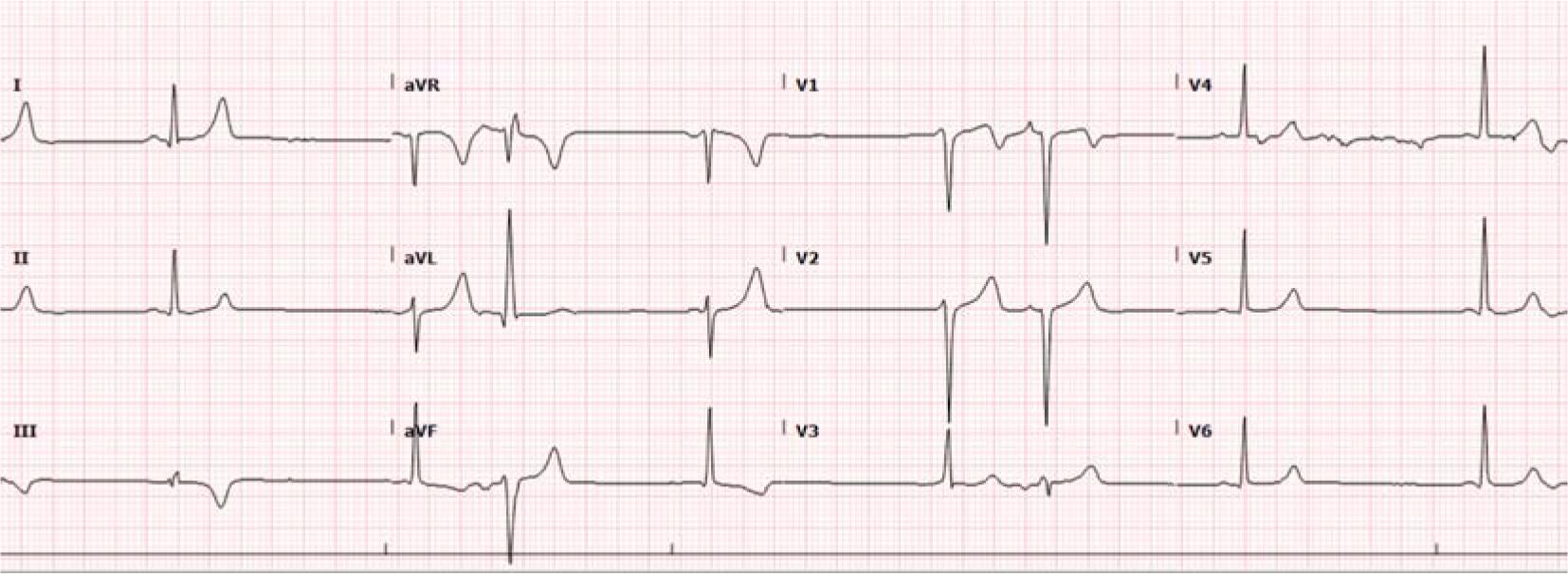
Subsequent development of atrial fibrillation.
CC is typically defined by cardiac arrest following a sudden chest blow, precipitating ventricular fibrillation.4 This is often in the setting of a sports injury, as a ball, helmet, or even a barbell may become the mechanism of force for a sudden impact. Typically, if the timing occurs at the vulnerable period of the cardiac cycle (the 15–30 ms upstroke of the T wave), sudden and potentially fatal ventricular arrhythmia occurs.
In the mechanism of ventricular arrhythmia production postulated by Link et al., there is a two-step process by which an initial depolarization is triggered from the traumatic impact during the vulnerable relative refractory period of the ventricles, with subsequent activation of the K+ATP channels, which are sensitive to stretch and pressure alterations.11 Animal testing has shown this to be specific in both the timing and location of the force.8
One previously published case of a teen developing AF in response to blunt helmet force during a football game suggests the process of a CCLE is likely a similar mechanism to traditional CC, only it is occurring in the atria.2 It was plausibly theorized that a blow at the vulnerable timing of atrial repolarization could precipitate an atrial arrhythmia like ventricular arrhythmias are induced in more typically documented CC cases. We propose the stretch-sensitive K+ATP channels present in the atria are predisposed to AF in athletes due to their increased vagal tone.12 Furthermore, the activation of these channels in the atria shortens the action potential and reduces the effective refractory period, increasing the risk of reentrant tachycardias, such as AF.13 Moreover, Link et al. demonstrated in their 2001 animal studies that not only timing is crucial but placement of the force. Only 9% of blows striking precordial sites that were not directly over the cardiac silhouette caused ventricular fibrillation; however, they did cause other arrhythmias, such as transient heart block and left bundle branch blocks.10
In this case, there was a significant delay in the onset of the atrial arrhythmia (over 24 h). Although only mildly elevated, there was a rise in troponin, which suggests some form of myocardial injury, even if only myocyte damage. Since no cardiac MRI was performed, we cannot rule out small-scale structural damage. It should be noted that even microscopic damage has been suggested as a cause for AF in the context of CCLE.1
On close examination of the presenting rhythm, a wandering atrial pacemaker demonstrated atrial irritability was also present, suggesting some level of disruption in the atria (Figure 1). Atrial stretch due to dilation has been recognized as a contributing factor in the initiation and maintenance of AF.14 The activation of stretch receptor activity, which may occur during a chest blow due to increased intra-atrial pressure, has been demonstrated in previous animal models to induce and maintain AF.15
The delayed onset of AF in this case occurred in the early morning hours during sleep, a circadian time known for its increased vagal tone, which has been demonstrated to contribute to AF, especially in young persons.13,16 Vagal stimulation, as previously demonstrated in animal studies, shortens the atrial action potential duration and refractory period by augmenting the acetylcholine-dependent potassium current influx.16 Additionally, conduction speed between and within the atria is reduced, along with scattered refractoriness, contributing to the initiation of AF.16 These key events all contribute to a sort of functional re-entry phenomenon that may occur during sleep, relating to the circadian rhythm. With ECG evidence of existing atrial irritability demonstrated at the initial insult, the likelihood of these factors causing an AF event are plausible in this case.
Another possible explanation is the development of a subclinical cardiac contusion due to blunt cardiac injury.17 Although the patient’s point-of-care ultrasound failed to demonstrate cardiac effusion, his chest CT was normal, and his echocardiogram was without wall motion defects to suggest structural damage, chest CT has a very low sensitivity, and echocardiography has only a moderate sensitivity in capturing characteristics consistent with a cardiac contusion.18 As cardiac MRI is the gold standard for detecting damage, and this was not performed, we cannot be sure structural cardiac insult was not sustained.19 Despite this limitation, the presence of immediate and prolific ventricular irritability, along with a delayed onset of atrial arrhythmia, suggest the cause was related to a blow significant enough to disrupt electrical conduction, but not delivered at the precise timing to cause ventricular fibrillation.20 Hemorrhage of the conduction system has been noted in animal trials after direct blows not resulting in ventricular fibrillation4 and could have occurred in this case. There is also the consideration of the previous similar blunt mechanism 8 months prior to this injury and the possibility of myocardial scar formation causing conduction anomalies from undetected damage at that time.21
CC is commonly characterized by collapse due to ventricular fibrillation, although atrioventricular block, ventricular irritability, and AF have been reported when blunt chest trauma occurs at other times in the cardiac cycle and may be considered in the category of CCLE. Whether stretch-sensitive channel activation occurs during the initial insult or microtrauma leads to conduction anomalies, monitoring of patients with CCLE for delayed development of or previously undetected atrial or ventricular arrhythmias is paramount in the emergency department.