
Pulmonary embolism (PE) is a serious and potentially life-threatening condition characterized by the blockage of one or more pulmonary arteries due to embolic material, typically a thrombus originating from the deep veins of the legs or pelvis. Large emboli can obstruct the main pulmonary artery, forming a saddle embolus that can trigger a sudden and sustained increase in pulmonary artery pressure, potentially resulting in circulatory collapse. Smaller emboli, on the other hand, typically obstruct peripheral arteries and can lead to pulmonary infarction, which occurs in approximately 10–50% of patients.1
The annual incidence of PE ranges from 39 to 115 cases per 100,000 people.2 Following coronary artery disease and stroke, acute PE is the third most prevalent cardiovascular condition.3,4 Despite the high effectiveness of early treatment, PE is often underdiagnosed and therefore remains a significant health issue.
PE is now understood to result from an interplay between patient–specific and situational risk factors, although it can also occur in individuals without identifiable predisposing factors. Several inherited conditions can elevate a patient’s risk of PE, including factor V Leiden, the prothrombin gene mutation (G20210A), antithrombin deficiency, protein C deficiency, and protein S deficiency, with the latter two being the most common.5 Acquired risk factors include trauma, surgery, malignancy, peripartum state, estrogen therapy, aging, infection, cancer, and obesity.6
The diagnosis of PE is frequently considered in patients presenting to the emergency department or admitted to the hospital. However, the symptoms of PE lack both sensitivity and specificity. In most cases, PE is suspected due to pleuritic chest pain, with or without accompanying dyspnea.7 Dyspnea can be acute and severe in central PE, whereas in individuals with preexisting heart failure or pulmonary disease, worsening dyspnea may be the only noticeable symptom. Syncope and shock are less common clinical manifestations.
The management of acute PE involves risk stratification, diagnosis, and treatment. Various tools have been developed to classify patients into high-, intermediate-, and low-risk groups. Multidetector computed tomography pulmonary angiography is the preferred diagnostic method, as it provides detailed visualization of the pulmonary arteries.8
This study examines PE with a focus on the role of inflammatory biomarkers in improving strategies for prevention, diagnosis, and treatment. In addition, we highlight that during the COVID-19 pandemic, the rise in case numbers was accompanied by more frequent reports of PE.
We conducted a retrospective observational study using data from medical records archived at the County Emergency Clinical Hospital Brașov. The study population included 97 patients diagnosed with PE who were admitted to the Cardiology Department between 1 March 2021 and 30 April 2022. We chose this study period because it overlapped with the COVID-19 pandemic, during which we observed an increase in the number of PE cases in our department.
Patients were included based on their order of admission, and their data were retrieved from archived medical records. For each patient, clinical and demographic parameters were collected and recorded in a Microsoft Excel database, including: age, gender, personal medical history, and risk factors (advanced age, hypertension, obesity, chronic kidney disease, smoking, prolonged immobilization, postoperative state, malignancies, history of previous venous thromboembolism, diabetes mellitus, heart failure, atrial fibrillation, neurological impairment, infection, including SARS-CoV-2 infection, and chronic obstructive pulmonary disease). Signs and symptoms at admission were also documented, such as dyspnea, chest pain, syncope, fever, hemoptysis, and unilateral lower limb pain or edema.
In addition, a comprehensive analysis was conducted on biological parameters, including D-dimer and troponin levels, as well as inflammatory biomarkers such as leukocyte and neutrophil counts, C-reactive protein (CRP), and fibrinogen levels.
The semiquantitative latex agglutination plasma fibrin D-dimer assay was used to determine D-dimer plasma levels (normal value <20 mg/L). D-dimer testing is mandatory in the diagnosis of arterial and venous thromboses, including PE, due to its high sensitivity but low specificity and intrinsically poor positive predictive value. Elevated D-dimer levels are not specific to thromboembolic disease, as they can also be observed in other conditions such as disseminated intravascular coagulation, infections, and malignant neoplasms. Conversely, a normal D–dimer value effectively excludes thrombosis and PE, given its high negative predictive value.9 Troponin T, a biomarker of myocardial necrosis and a prognostic factor in PE, was evaluated by ECLIA assay (normal value <0.1 ng/dL). Inflammatory biomarkers were also analyzed: CRP by immunoturbidimetric assay (normal values 0–0.5 mg/dl) and fibrinogen by continuous sequential photo-optical method (normal values 200–400 mg/dl).10−15 No patient included in this study had signs, symptoms, laboratory results, or imaging findings suggestive of sepsis that would require procalcitonin testing. Therapeutic management approaches were also systematically evaluated.
Given the ongoing debate regarding the role of SARS-CoV-2 infection and vaccination against SARS-CoV-2 in amplifying the systemic inflammatory response and thereby promoting arterial or venous thrombosis,16–18 we performed a comparative observational analysis in this retrospective study between patients exposed to infection at admission or vaccination within 4 months.
The statistical analysis methods were selected in accordance with research methodology. GraphPad Prism version 10.4.1 and Microsoft Excel Office 2019 were used. Clinical characteristics and demographic data of the study population were analyzed using descriptive statistics, expressed as percentages for categorical variables. Fisher’s exact test was applied to assess differences in categorical variables, Pearson’s correlation to evaluate relationships between variables, and multiple linear regression to assess independent predictors. A p value <0.05 was considered statistically significant for all tests.
The study group consisted of 97 patients: 47 males (48.45%) and 50 females (51.54%). Patient ages ranged from 31 to 88 years, with a mean age of 66.83 years. They were divided into five age categories (Figure 1). The first group included 5 patients (5.15%) aged 30–39 years, the second group 5 patients (5.15%) aged 40–49 years, and the third group 11 patients (11.34%) aged 50–59 years. No significant sex-related differences in the incidence of pulmonary embolism were observed in these age groups. The fourth category comprised 34 patients (35.05%) aged 60–69 years, while the fifth group included 42 patients (43.29%) aged ≥70 years. The incidence of pulmonary embolism increased significantly after the age of 60 (n = 76, 78.35%; p < 0.05), without notable sex–related differences.
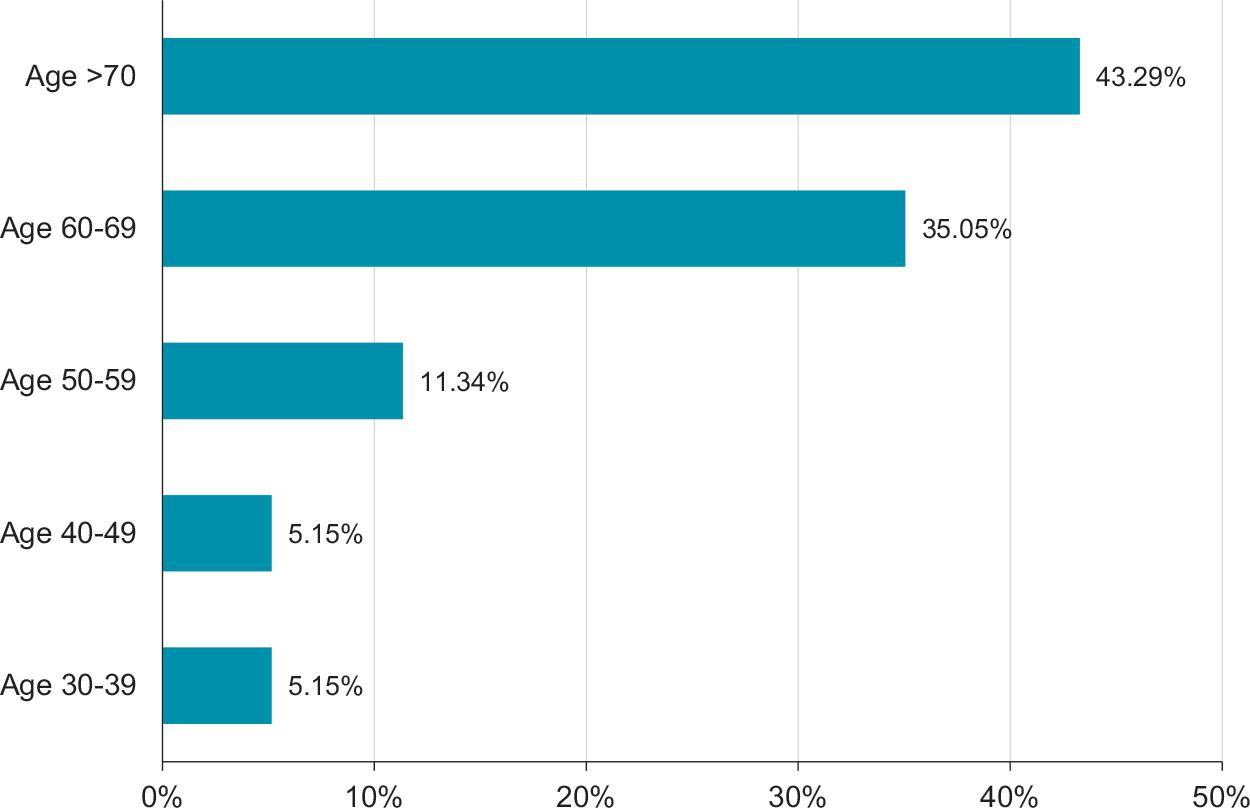
Distribution of patients with PE by age group.
The most frequently identified risk factors were age > 60 years (n = 76, 78.35%), hypertension (n = 53, 54.63%), obesity (n = 35, 36.08%), chronic kidney disease (n = 28, 28.86%), smoking (n = 26, 26.86%), prolonged immobilization (n = 22, 22.68%), postoperative state (n = 21, 21.64%), and malignancies (n = 20, 20.61%). Less frequent risk factors included a history of venous thromboembolism (n = 16, 16.49%), diabetes mellitus (n = 16, 16.49%), recent SARS-CoV-2 infection confirmed by RT-PCR at admission (n = 12, 12.37%), vaccination against SARS-CoV-2 within the past 4 months (n = 14, 14.43%), heart failure (n = 10, 10.30%), atrial fibrillation (n = 10, 10.30%), neurological impairment (n = 10, 10.30%), infection (n = 9, 9.27%), and chronic obstructive pulmonary disease (n = 4, 4.12%) (Figure 2).
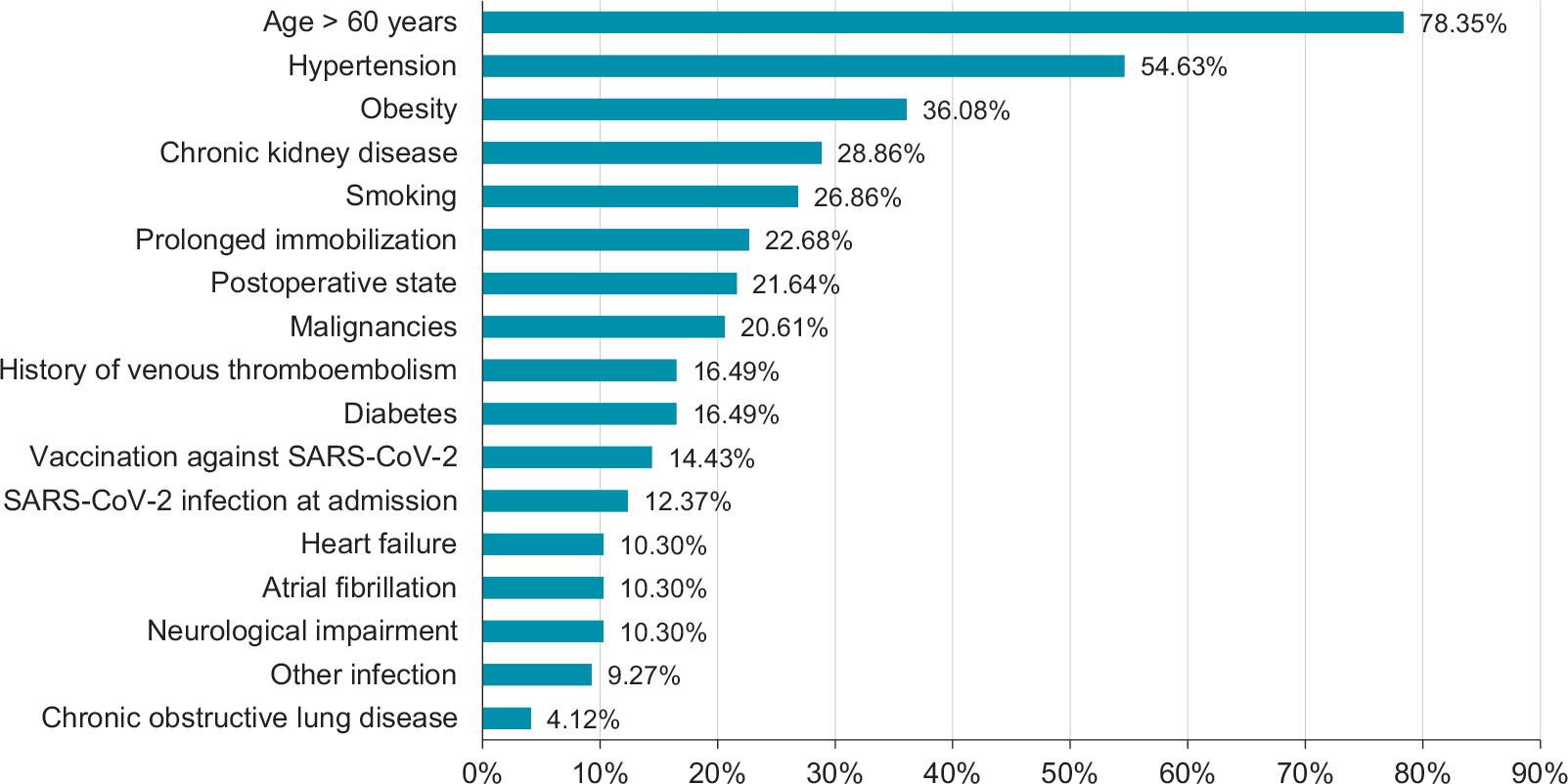
Most frequently identified risk factors for PE.
As shown, numerous risk factors were identified in patients diagnosed with PE in our study group. These factors ranged from the most frequent (age >60 years) to the least frequent (chronic obstructive pulmonary disease), and all were associated with varying degrees of inflammation. Inflammation, as consistently demonstrated in the medical literature, can be considered the “red line” underlying the thrombotic event.
More than one–quarter of patients diagnosed with PE (26/97, 26.80%), defined as the COVID-19 subgroup, either had a recent positive SARS-CoV-2 RT-PCR test at admission (n = 12, 12.37%) or had been vaccinated within the past four months (n = 14, 14.43%) at the time of the thromboembolic event. The data obtained from this subgroup were compared with those of the remaining 71 patients (73.20%), defined as the non-COVID-19 subgroup (Figure 3).
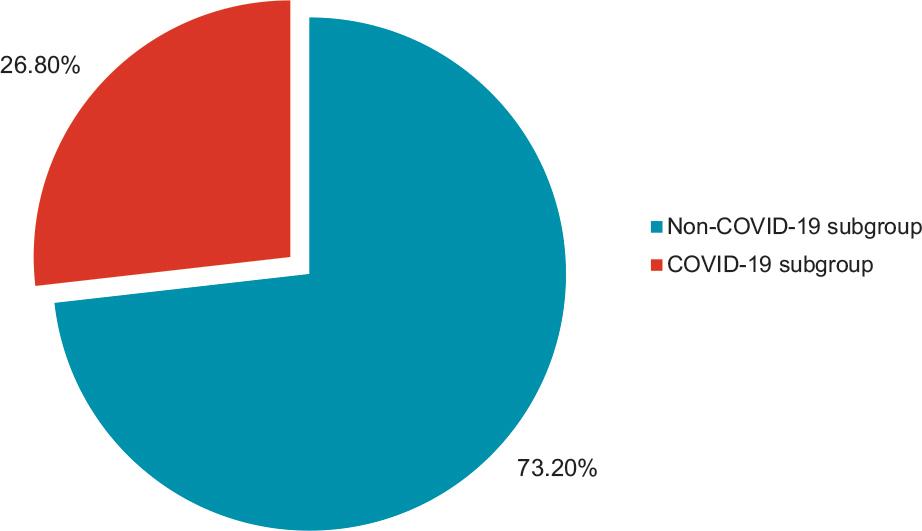
Incidence of PE in relation to COVID-19 infection or vaccination.
The most common symptoms of pulmonary embolism (Table 1) identified in the patient cohort were dyspnea (n = 64, 65.97%), chest pain (n = 34, 35.05%), syncope (n = 10, 10.30%), and fever (n = 10, 10.30%), while hemoptysis was observed in only three patients (3.09%). On clinical examination, 43 patients (44.33%) presented with unilateral lower limb pain or edema; however, deep venous thrombosis was confirmed by compression ultrasonography in only 29 of these cases (29.89%). At admission, 21 patients (21.67%) showed signs of heart failure, of whom 11 (11.34%) had no prior history of the condition. Cardiogenic shock was the initial manifestation of pulmonary embolism in only one patient.
The prevalence of signs and symptoms of PE.
| Sign or symptom | n | % |
|---|---|---|
| Dyspnea | 64 | 65.97 |
| Lower limb pain or edema | 43 | 44.33 |
| Chest pain | 34 | 35.05 |
| Syncope | 10 | 10.30 |
| Fever | 10 | 10.30 |
| Hemoptysis | 3 | 3.09 |
Although a comprehensive clinical examination is essential for suspecting pulmonary embolism, diagnostic confirmation requires laboratory and imaging investigations. In our study group, D-dimer measurement was performed in all patients in the emergency department, and elevated levels were recorded in every case. Serum troponin was elevated in 14 patients (14.43%) with moderate or large pulmonary embolism who also presented with right ventricular dysfunction. A normal D-dimer level was considered an exclusion criterion for PE diagnosis.
The study group was also assessed for inflammatory biomarkers. In the COVID-19 subgroup (26 patients, 26.80%), alterations included leukocytosis in 15 patients (57.69%), neutrophilia in 16 patients (61.54%), elevated C-reactive protein levels in 19 patients (73.08%), and increased fibrinogen levels in 18 patients (69.23%). In the non-COVID-19 subgroup (71 patients, 73.20%), leukocytosis was detected in 31 patients (43.66%), neutrophilia in 25 patients (35.21%), elevated C-reactive protein levels in 48 patients (67.61%), and increased fibrinogen levels in 45 patients (63.38%) (Figure 4).
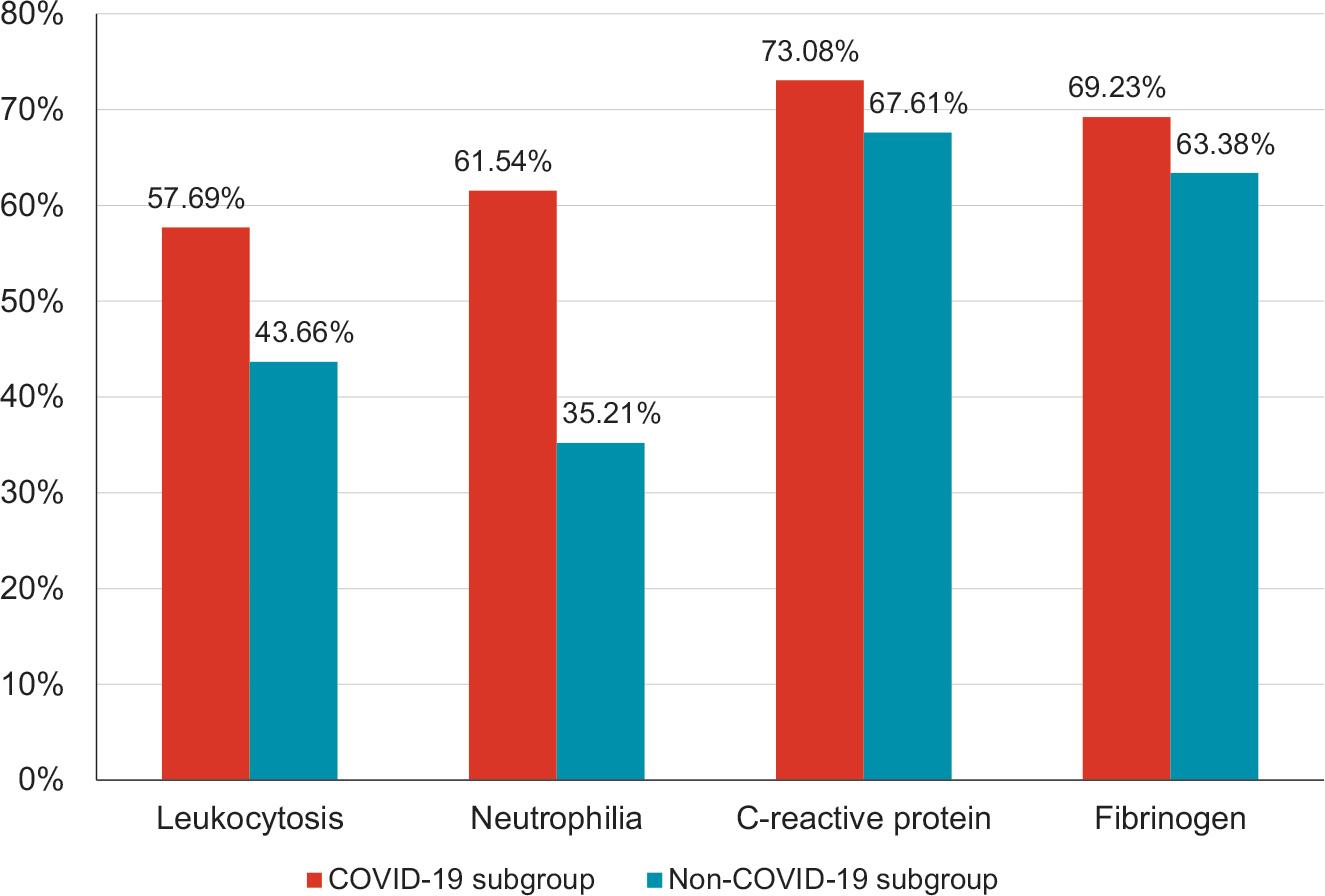
Inflammatory markers in COVID-19 and non-COVID-19 subgroups.
There were no reported cases of septic shock or septic embolism. Among patients with massive pulmonary embolism, elevated serum levels of aspartate aminotransferase (n = 8, 8.24%) and lactate dehydrogenase (n = 8, 8.24%) were recorded. The diagnosis of pulmonary embolism was confirmed using computed tomography angiography in all patients. Imaging reports enabled classification of pulmonary embolism cases based on the anatomical location of the embolus as follows: main pulmonary artery (n = 66, 68.04%), lobar pulmonary artery (n = 27, 27.83%), and segmental pulmonary artery (n = 4, 4.12%) (Figure 5).
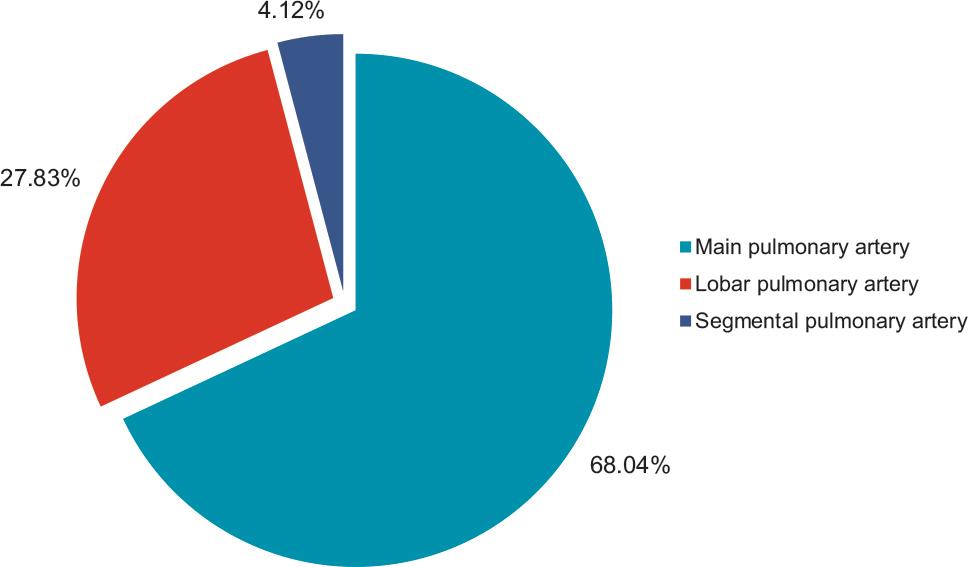
Anatomical location of PE.
The most common initial treatment was therapeutic dose LMWH (Low Molecular Weight Heparin), administered in 83 cases (85.56%). Additionally, 14 patients (14.43%) required thrombolysis at onset. Among treatment-related complications, 10 patients (10.31%) experienced mild thrombocytopenia, including 3 patients (21.4%) who had undergone thrombolysis. None of these cases required platelet transfusion, but this finding highlights the need for careful monitoring of thrombolyzed patients, particularly since anticoagulant therapy with LMWH, usually administered after thrombolysis, can further reduce platelet counts. Of the 97 patients included in the study cohort, 23 (23.7%) presented with anemia upon admission, of whom 3 (3.09%) required red blood cell transfusion due to exacerbation of anemia during anticoagulant therapy with LMWH. Furthermore, three of the 14 patients (21.4%) who received thrombolysis developed mild anemia, which did not necessitate transfusion.
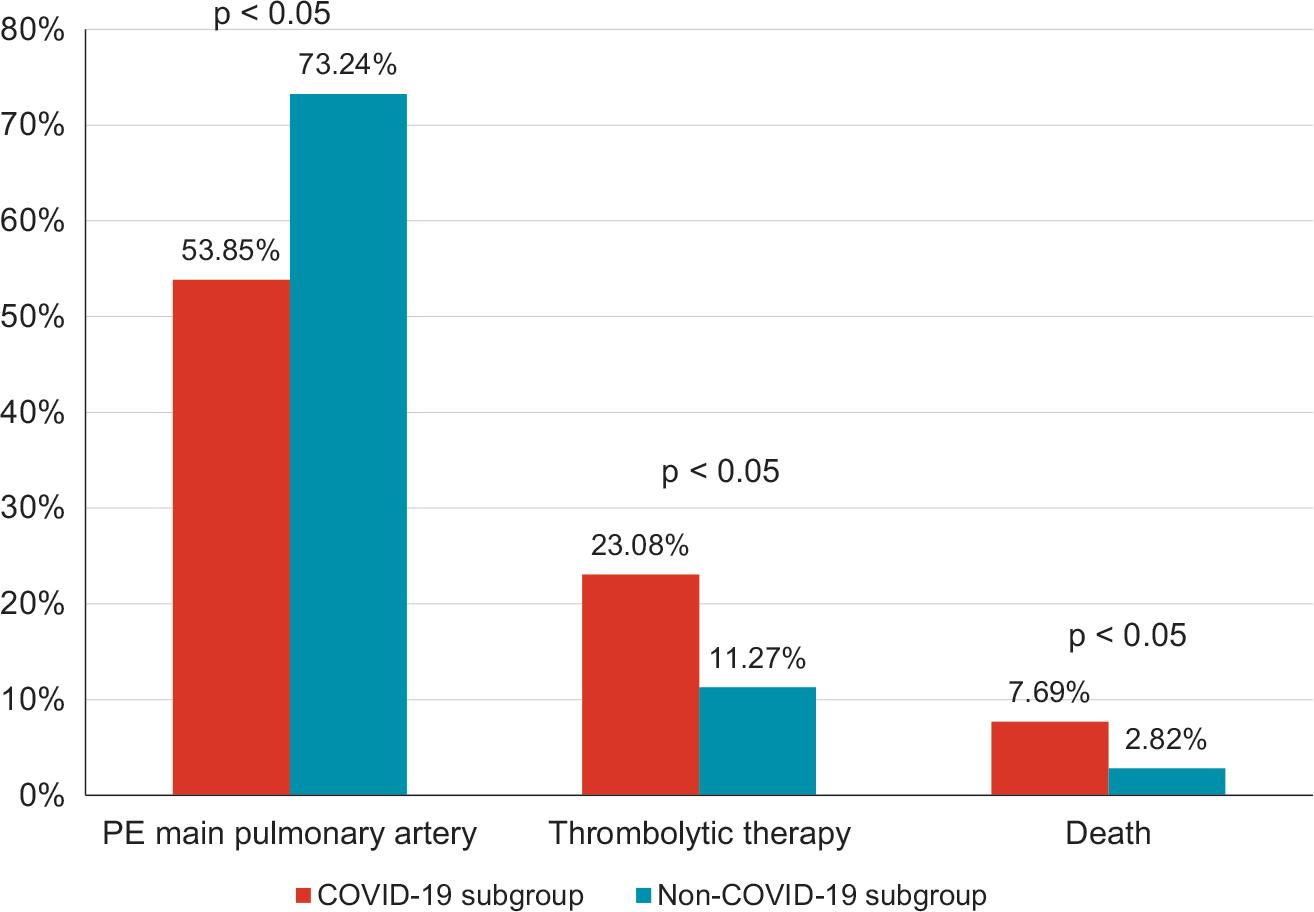
Prognostic characteristics of COVID-19 and non-COVID-19 subgroups.
The average duration of hospitalization was 8.29 days. During the hospital stay, four patients died (4.12% in-hospital mortality). The mean age of these patients was 68.75 years. Two were diagnosed with main pulmonary artery embolism on computed tomography pulmonary angiography and progressed to cardiogenic shock. Notably, none of the patients who died had received thrombolytic therapy.
Patients in the COVID-19 subgroup experienced more severe forms of PE. Although a smaller proportion of patients in this subgroup (14 patients, 53.85%) were diagnosed with pulmonary embolism affecting the main pulmonary artery compared with 52 patients (73.24%, p < 0.05) in the non-COVID-19 subgroup, their clinical course was more severe. In the COVID-19 subgroup, six patients (23.08%) required thrombolytic therapy compared with eight patients (11.27%, p < 0.05) in the non-COVID-19 subgroup. In-hospital mortality was also higher: two patients (7.69%) in the COVID-19 subgroup compared with two patients (2.82%, p < 0.05) in the non-COVID-19 subgroup.
This study seeks to elucidate the clinical manifestations and diagnostic approaches in PE, while also examining the medical practices used in its management.
The mean age of the cohort was 66.83 years, slightly higher than the average reported in other registries, such as the Garfield-VTE Registry (60.2 years).19 Nonetheless, the near-equal distribution of sexes in our group (51.54% female and 48.45% male) was consistent with other studies. A slightly higher prevalence of women has also been reported in other PE registries, including ICOPER (55%)20 and JASPER (60.5%).21
PE is a multifactorial disease with an etiological profile similar to other cardiovascular conditions, such as coronary and cerebral ischemia, hypertension, and metabolic disorders including diabetes mellitus and dyslipidemia. In recent years, SARS-CoV-2 infection and vaccination have emerged as additional risk factors.10,22 In our study, patients in the COVID-19 subgroup, defined as those with PE occurring during or after SARS-CoV-2 infection or within 4 months of vaccination, exhibited higher levels of inflammatory markers, further reinforcing the pathophysiological role of inflammation in the development of PE.23
It is imperative for clinicians to adopt a comprehensive approach, integrating established cardiovascular risk reduction strategies into the prevention of venous thrombo-embolism.24,25 Our study highlighted the most frequently implicated risk factors, with the leading contributors being advanced age (>60 years; 78.35%), hypertension (54.63%), obesity (36.08%), chronic kidney disease (28.86%), COVID-19 infection/vaccination or infection within 4 months after vaccination (26.80%), smoking (26.86%), prolonged immobilization (22.68%), postoperative status (21.64%), and malignancies (20.61%). These findings are consistent with those from other registries.26,27 However, the present study does not provide a comprehensive assessment of all risk factors, as certain critical contributors, such as thrombophilia, were not evaluated.28
Nearly a quarter of the patients in our study diagnosed with PE had underlying neoplasms (20.61%), findings consistent with other registries such as ICOPER (22.5%)20 and JASPER (23%).21 Cancer cells can activate the coagulation cascade and enhance the prothrombotic properties of host cells. In addition, several anticancer therapies have been identified as independent contributors to thrombogenesis.29,30 Tumors may also exert compressive effects on adjacent structures, leading to venous stasis and consequently thrombosis.31,32
Venous thromboembolism significantly contributes to morbidity and mortality among cancer patients, with fatal PE occurring three times more frequently in those with malignancy compared to non-cancer patients. Furthermore, individuals diagnosed with malignancy in the context of acute venous thromboembolism have a substantially poorer prognosis than cancer patients without thrombotic events.33
In COVID-19-associated coagulopathy, the trigger is vascular inflammation and endothelial dysfunction, followed by venous, arterial, or microcirculatory thrombosis. This coagulopathy is characterized by markedly elevated fibrin degradation products such as D-dimers, platelet aggregation, thrombin generation, and subsequent thrombus formation. Endothelial inflammation is considered the cornerstone of this process.34,35 Moreover, SARS-CoV-2 infection induces both immune and non-immune cellular responses, leading to an imbalance between procoagulant and anticoagulant factors, a key mechanism of thrombus formation in COVID-19.36 The physiological response to excessive activation of the coagulation cascade results in fibrin clot breakdown and D-dimer release.35 In patients with COVID-19, D-dimer levels have predictive value for thrombosis and correlate with disease severity, acute respiratory distress syndrome, and mortality.10,37
Patients with active SARS-CoV-2 infection (or in the peri-disease state) share many risk factors for venous thromboembolism with those unaffected by the condition.38 Severe SARS-CoV-2 infection, however, has been linked to coagulopathy and an increased risk of thromboembolic events. Early reports during the COVID-19 pandemic by Cui et al.39 described a correlation between thromboembolic risk in patients with severe novel coronavirus pneumonia and hematological/coagulation abnormalities such as lymphocytopenia, elevated D-dimer levels, and prolonged prothrombin time. Subsequent studies, however, have shown substantial variability, likely explained by differences in hospital practices regarding venous thromboembolism prophylaxis, deep vein thrombosis screening protocols, anticoagulation strategies in confirmed COVID-19 cases, and heterogeneity in study designs and durations. In our cohort, 26 patients (mean age 62.69 years) were diagnosed with SARS-CoV-2 infection confirmed via RT-PCR testing (n = 12) or had received vaccination within the previous 4 months (n = 14). Of these, 12 patients had PE involving the main pulmonary artery, and 4 required thrombolytic therapy. Inflammatory markers were more frequently elevated in the COVID-19 subgroup compared to the non-COVID-19 subgroup. Both severe disease course and mortality were also significantly higher in the COVID-19 subgroup.
Smoking is an independent and modifiable risk factor for PE. In our study, 26.86% of patients reported a history of smoking. The metabolic risk factors evaluated included obesity, defined as a body mass index of ≥30.0 (36.08%), and diabetes mellitus (16.49%). Obesity is associated with physical inactivity, increased intra-abdominal pressure, chronic systemic inflammation, and impaired fibrinolysis. These mechanisms are further exacerbated by elevated circulating levels of von Willebrand factor and factor VIII, collectively contributing to a heightened prothrombotic risk.40,41
Chronic respiratory failure in the context of chronic obstructive lung disease was observed in 4.12% of cases in our cohort, a lower prevalence compared to other observational studies, such as the ICOPER Registry, which reported a 12% incidence.9 Venous thromboembolism is a frequent complication in patients with respiratory dysfunction, with evidence indicating that 1-year mortality significantly increases after a thrombotic event. Therefore, effective prophylaxis and maintaining a high index of suspicion for venous thromboembolism are strongly recommended, particularly in patients with acute exacerbations of chronic obstructive lung disease.42
At admission, 21.67% of patients in our study group showed signs of heart failure, with 10.30% having a prior history of the condition. The relationship between heart failure and venous thromboembolism is not yet fully understood, but several mechanisms have been proposed: blood stasis due to ventricular dilation, reduced myocardial contractility, elevated central and intracardiac venous pressures, increased plasma viscosity and coagulability, neurohormonal activation, and, in particular, the inflammatory processes consistently associated with endothelial dysfunction. Together, these factors promote a hypercoagulable state, significantly elevating cardiovascular risk.43 Some studies suggest that chronic heart failure confers a greater predisposition to venous thromboembolism than acute heart failure. Moreover, patients with heart failure appear more likely to develop PE than deep vein thrombosis.44
Among the 10 patients with a history of stroke or transient ischemic attack, only five were receiving antiplatelet or anticoagulant therapy prior to admission, and one had a documented history of malignancy. This subgroup had a mean age of 74.8 years and an equal distribution of sexes. All patients were hemodynamically stable at admission, and 60% showed involvement of at least one main branch of the pulmonary artery. Patients with a history of stroke are often characterized by significant multimorbidity. However, the relatively low prevalence of thromboembolic events in this subgroup may be partly explained by the routine use of antiplatelet therapy, which plays a critical role in thrombosis prevention. Despite this, venous thromboembolism remains a serious complication during the post-stroke recovery phase, substantially increasing both mortality and long-term disability.
According to other registries, most patients with PE present with at least one of four symptoms: sudden-onset dyspnea, chest pain, syncope, and hemoptysis. The presence of these symptoms, when not attributable to other causes, should prompt clinicians to include PE in the differential diagnosis and initiate appropriate diagnostic testing.45 In our patient cohort, the most reported symptoms were also dyspnea (65.97%), chest pain (35.05%), syncope (10.30%) and hemoptysis (3.09%). Cardiogenic shock was the initial presentation of PE in only one patient. On clinical examination, 44.33% of patients exhibited unilateral lower limb pain or edema; however, compression ultrasonography confirmed deep vein thrombosis in only 29.89% of these cases.
Anticoagulation remains the cornerstone of treatment for acute PE. Both low–molecular–weight heparin and unfractionated heparin are viable options for anticoagulation in acute PE. However, low–molecular–weight heparin is generally favored due to its lower risk of major bleeding and heparin-induced thrombocytopenia. In our study, the majority of patients (85.56%) received anticoagulant therapy with low–molecular–weight heparin.
Only 14 patients (14.44%) met the criteria for thrombolytic therapy. This is consistent with expectations, as most patients presented with low- or intermediate-risk PE, in line with current clinical guidelines.33 No major hemorrhagic events occurred during hospitalization, including among those who received thrombolysis. The treatment of high-risk PE – and selected intermediaterisk patients with clinical deterioration – relies on fibrinolysis, the gold-standard intervention for reducing mortality, albeit with the cost of an increased bleeding risk. This approach has been shown to reduce all–cause mortality, PE-related mortality, and recurrence compared with unfractionated heparin alone.4,46,47 However, it is associated with a high risk of bleeding: a meta-analysis of 16 randomized controlled trials (2,057 patients) reported a number needed to treat (NNT) of 59 for allcause mortality and a number needed to harm (NNH) of 18 for major bleeding.19 Reduced-dose thrombolysis is not recommended, as no significant differences were observed in rates of major bleeding or all-cause death when comparing low-dose rt-PA with standard heparin therapy.4,48,49
The mean hospital stay was 8.29 days. The four patients who died during hospitalization had a mean age of 68.75 years. Two presented with main pulmonary artery embolism and developed cardiogenic shock; notably, none of them received thrombolytic therapy. Hemodynamic instability, though uncommon, is a critical clinical presentation that often reflects central or extensive PE with severely compromised hemodynamic reserve.50 Consequently, timely diagnosis of PE is imperative, given its significant associated morbidity and mortality.
As a retrospective registry with a predefined cohort and specific timeframe, this study has inherent limitations. However, unlike randomized clinical trials, it offers the advantage of reflecting clinical management decisions made independently by physicians, thereby providing valuable insights into real-world scenarios. This is particularly relevant given the novel challenges posed to healthcare systems during the COVID-19 pandemic. Moreover, this study highlights contemporary clinical practices, sheds light on treatment strategies and decision-making processes during hospitalization, and identifies patient-specific factors associated with unfavorable prognoses.
Another limitation is the lack of NT-proBNP data due to inconsistent reagent supply during the difficult postpandemic period of 2021–2022. Right ventricular strain, an important prognostic parameter, could also not be assessed, as this evaluation only became available in our hospital in 2024.
Regarding NT-proBNP, the 2019 guidelines of the European Society of Cardiology for the diagnosis and management of acute PE (developed in collaboration with the European Respiratory Society),49 note findings from a subsequent non-inferiority trial that randomized 550 patients based on the Hestia criteria alone vs. Hestia plus NT-proBNP testing (<500 pg/ml as a discharge criterion). The primary outcome (30-day PE or bleeding-related mortality, cardiopulmonary resuscitation, or intensive care admission) was very low in both arms. These results suggest no incremental value of NT-proBNP testing, although the study was not powered to definitively exclude a benefit.49,51
Echocardiographic parameters of right ventricular function derived from Doppler tissue imaging and wall strain assessment may also be affected by the presence of acute PE. However, their sensitivity as stand-alone findings is likely low, as they have been reported to remain normal in hemodynamically stable patients despite confirmed PE.49,52,53
As previously noted, during the immediate post–COVID-19 pandemic period, reduced reagent availability on the Romanian market and the relatively high cost of NT–proBNP testing limited its widespread use. Consequently, many hospitals in our country, including ours, were unable to routinely purchase NT-proBNP reagents. Furthermore, according to institutional procedures and national protocols, NT-proBNP testing is primarily recommended for patients with heart failure.
In addition, due to the unprecedented financial challenges of the pandemic and post-pandemic period, our hospital was only able to acquire updated software for wall strain assessment in 2024. By contrast, the present study reports data from 2021–2022, a period marked by a high incidence of pulmonary embolism.
Despite these limitations, retrospective studies such as ours can still provide valuable insights for clinicians in their daily practice. At the same time, large, multicenter prospective trials remain necessary to validate these real world observations.
In our study, the most frequently identified risk factors were advanced age (>60 years), hypertension, and obesity. Additionally, individuals with SARS-CoV-2 infection at admission or within 4 months after vaccination had an increased risk of thromboembolic events, with a significantly higher likelihood of severe evolution and death. Among laboratory investigations, inflammation emerged as a key element in the early diagnosis and management of PE, particularly in patients within the COVID-19 subgroup. D-dimer testing demonstrated a high negative predictive value; thus, a normal result effectively reduces the probability of acute PE. Anticoagulant therapy remains the cornerstone of treatment, while thrombolysis is reserved for cases with hemodynamic instability. These findings, derived from retrospective observational research, require validation through large-scale clinical studies.