Hypertensive emergencies represent critical, life-threatening conditions characterized by severe elevations in blood pressure (BP) leading to acute target organ damage, such as encephalopathy, myocardial infarction, heart failure, stroke, or renal failure.1,2
Despite advancements in antihypertensive therapy and better awareness of hypertension as a global health burden, hypertensive emergencies occur in 1–2% of patients with hypertension, often precipitated by inadequate disease control, poor adherence to medications, or late recognition of hypertensive crises. Recent global estimates underscore that uncontrolled hypertension affects over one billion people worldwide, contributing to nearly half of all cardiovascular deaths, many of which are preventable with timely intervention and management.2,3
The clinical presentation of hypertensive emergencies is characterized by heterogeneity, necessitating rapid identification and tailored therapeutic approaches. They encompass diverse scenarios, including hypertensive encephalopathy, aortic dissection, preeclampsia, and acute coronary syndromes, each demanding specific diagnostic and therapeutic considerations. The management of a patient with acute pulmonary edema due to a hypertensive crisis differs fundamentally from that of a pregnant woman with preeclampsia, underscoring the necessity of individualized treatment strategies.1
Guidelines from the European Society of Cardiology (ESC), the European Society of Hypertension (ESH), and the American College of Cardiology/American Heart Association (ACC/AHA) provide foundational recommendations for diagnosing and managing hypertensive emergencies. These documents emphasize the importance of rapid BP reduction, but caution against excessive lowering to mitigate further organ damage while preserving perfusion to critical tissues. Notably, the 2024 ESC guidelines introduce refinements in stratifying risk and optimizing antihypertensive therapy, reflecting evolving evidence in clinical practices.1,4,5
The pathophysiology of hypertensive emergencies involves a complex interplay of endothelial dysfunction, overactivation of the renin–angiotensin–aldosterone system (RAAS), and increased sympathetic nervous system activity. These processes lead to acute increases in vascular resistance and direct injury to vital organs. Understanding these mechanisms has shaped therapeutic strategies and highlighted the limited evidence supporting tailored therapies, underscoring the need for further research.3,6,7
Although existing literature and guidelines provide robust frameworks for managing hypertensive emergencies, gaps remain in optimizing care pathways and personalizing treatment. This article aims to review current practices, explore emerging therapies, and address gaps in managing hypertensive emergencies, providing a comprehensive perspective that integrates existing knowledge with innovative strategies for future care.
Hypertensive emergencies are characterized by a rapid and severe increase in BP that leads to acute target organ damage. Conversely, hypertensive urgencies identify patients with significantly elevated BP but without immediate evidence of end-organ damage. Distinguishing between these conditions is essential, as it guides treatment intensity.1,3
Hypertensive emergencies include various clinical scenarios in which elevated BP directly causes or exacerbates acute organ damage, including hypertensive encephalopathy, acute aortic dissection, acute heart failure, myocardial ischemia, intracranial hemorrhage or ischemic stroke, acute kidney injury, preeclampsia or eclampsia.1,8
Hypertensive urgencies involve severe BP elevation (e.g., systolic BP >180 mmHg or diastolic BP >120 mmHg) without acute end-organ damage. These situations typically do not require emergency intervention but outpatient management to gradually reduce BP over hours to days, minimizing the risk of ischemic complications.1,3
Hypertensive emergencies, although less frequent than chronic hypertension, exert a significant healthcare burden due to their severe morbidity and mortality. It is estimated that 1–2% of individuals with hypertension will experience a hypertensive emergency during their life-time.3 The global prevalence is influenced by variations in healthcare access, socioeconomic conditions, and disparities in hypertension management. In high-income countries, improvements in public health measures, early screening, and effective treatment strategies have reduced the incidence of hypertensive emergencies. However, in low- and middle-income countries, limited healthcare infrastructure, low awareness, and economic constraints contribute to a higher prevalence.3
In a large multicenter study, the most common scenarios linked to hypertensive emergencies were acute pulmonary edema (30.9%), stroke (22%), and myocardial infarction (17.9%), followed by acute aortic dissection (7.9%), acute renal failure, and hypertensive encephalopathy (4.9%).9,10 Also, men had a 34% higher risk of experiencing hypertensive emergencies than women.9,10
In a meta-analysis of eight studies, the most frequent acute hypertensive-mediated organ damage (HMOD) were pulmonary edema and heart failure (32%), followed by ischemic stroke (29%), acute coronary syndrome (18%), hemorrhagic stroke (11%), acute aortic syndrome (2%), and hypertensive encephalopathy (2%).11 Notably, BP levels at presentation did not differ significantly between patients with hypertensive urgencies and emergencies, emphasizing that BP alone is not a reliable predictor of HMOD. Instead, presenting signs and symptoms play a more critical role in identifying emergencies.11
A recent preliminary report from the ERIDANO clinical trial revealed comparable findings, identifying heart failure as the most common HMOD (39%), followed by stroke (33%), acute coronary syndrome (11%), hypertensive encephalopathy (11%), and aortic dissection (6%).12
Demographic studies show that middle-aged and elderly populations are most commonly affected by hypertensive emergencies, likely due to long-standing vascular damage from poorly controlled hypertension. Ethnicity is also an important factor, as African-American populations are disproportionately affected due to higher baseline hypertension prevalence and associated conditions such as diabetes mellitus and chronic kidney disease.3,13
Uncontrolled hypertension remains the most significant risk factor for hypertensive emergencies, often resulting from medication non-compliance, insufficient follow-up, or lack of access to healthcare services. Secondary forms of hypertension, such as those caused by renovascular disease, primary aldosteronism, or pheochromocytoma, also contribute to an increased risk. Acute triggers, including abrupt withdrawal of antihypertensive medications, drug abuse (e.g., cocaine or amphetamines), and stressors such as surgery or infections, often precipitate these crises.3,14,15
Lifestyle factors, including high sodium diets, obesity, smoking, and excessive alcohol intake, constitute modifiable contributors related to poor blood pressure control. Public health initiatives focusing on these areas could significantly reduce the prevalence of hypertensive emergencies.3,13
The outcomes of patients presenting with hypertensive emergency or urgency are influenced by the choice and timing of antihypertensive therapy. A study involving patients with hypertensive crises discharged from the emergency department found significant differences in the management and associated outcomes between those receiving pharmacological intervention and those who did not. Patients who received antihypertensive medications during emergency department stay had an 11% lower risk of hospital revisit at 30 and 60 days. However, no significant differences were observed in long-term outcomes, such as cardiovascular mortality or stroke during 5 years of follow-up.16
A recent study compared 1-year cardiovascular outcomes in patients with hypertensive emergencies and urgencies. Among 272 patients, those with hypertensive emergency experienced significantly higher rates of cardiovascular events and mortality compared to the urgency group. Over the follow-up period, non-fatal cardiovascular events were observed in 29 patients from the emergency group, compared to 9 in the urgency group (HR 3.43, 95% CI 1.7–6.9; p = 0.001). Similarly, cardiovascular-related mortality was substantially greater in patients with hypertensive emergency (HR 13.2, 95% CI 1.57–110.8; p = 0.017).17 These results highlight the severe prognostic implications of hypertensive emergencies, reflecting the acute organ damage present at the time of diagnosis.
BP control during the initial hours of treatment poses greater challenges in hypertensive emergencies compared to urgencies. One study reported that only 50% of patients with hypertensive emergencies achieved BP levels below 180/110 mmHg, compared to 76.7% of those with hypertensive urgencies in 1 hour following ED admission.12 This discrepancy highlights the complexity of managing hypertensive emergencies, in which acute target organ damage often requires a more cautious approach to BP reduction to avoid compromising organ perfusion. Three days post-discharge, systolic BP improved further to a mean of 148 ± 22 mmHg, although only 34.4% of patients achieved normotensive status (BP < 140/90 mmHg). Patients with hypertensive urgencies were more likely to achieve normotensive levels compared to those with emergencies. Factors associated with uncontrolled BP included male sex and higher arterial stiffness, as evidenced by increased pulse wave velocity.12
These findings emphasize the critical importance of tailored therapeutic strategies in hypertensive emergencies, in which immediate BP reduction must be balanced against the risk of exacerbating organ damage. Long-term monitoring remains essential to ensure sustained BP control and prevent recurrence.12
Although acute pharmacological interventions effectively reduce short-term risks, long-term outcomes require a broader focus on sustained blood pressure control, prevention of HMOD progression, and management of comorbidities. Future research should explore the role of advanced diagnostic tools and precision medicine in improving both immediate and extended outcomes for these high-risk patients.
The pathophysiology of hypertensive emergency is complex and multifaceted, involving both vascular and systemic mechanisms. Two central processes – failure of vascular autoregulation and activation of the RAAS – have been identified as pivotal contributors to the development and progression of hypertensive crises (Figure 1).10,18
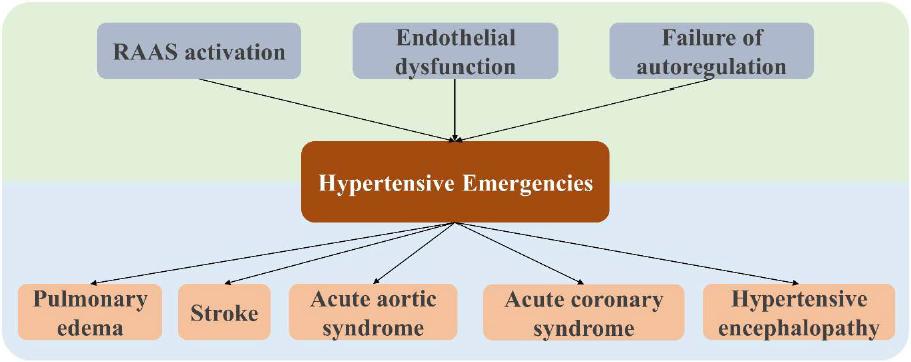
Pathophysiological mechanisms and clinical manifestations of hypertensive emergencies.
Autoregulation, the ability of vital organs such as the brain, heart, and kidneys to maintain stable blood flow despite fluctuations in perfusion pressure, plays a critical role. In normotensive individuals, this mechanism ensures that perfusion remains constant across a wide range of blood pressures. However, in patients with chronic hypertension, prolonged exposure to elevated blood pressure leads to vascular remodeling and impaired autoregulatory capacity. This shifts the autoregulatory threshold to higher blood pressure levels, leaving these individuals vulnerable to acute rises in systemic vascular resistance. The failure of autoregulation in hypertensive crises results in mechanical stress and endothelial injury, further exacerbating microvascular damage and organ dysfunction.10,18
The activation of the RAAS is another key mechanism. During hypertensive crises, excessive activation of this system amplifies vasoconstriction, promotes sodium retention, and leads to pressure natriuresis and volume depletion. This creates a loop that accelerates blood pressure elevation, contributing to the perpetuation of hypertensive emergencies. The resulting microcirculatory damage exacerbates organ ischemia and injury.10,18
Emerging evidence also suggests a prothrombotic state may play a role in hypertensive emergencies. A study highlighted significantly elevated levels of soluble P-selectin, a marker of platelet activation, in patients experiencing hypertensive crises compared to normotensive controls. This finding suggests that platelet activation is an early event in the pathophysiological cascade, potentially contributing to vascular injury and thrombosis.10,19
Recent evidence has highlighted the role of abnormal angiogenesis and endothelial dysfunction in the pathophysiology of hypertensive emergencies.20 One study reported persistently elevated levels of serum soluble Fms-like tyrosine kinase-1 (sFlt-1) in patients presenting with hypertensive emergencies. Notably, ADAMTS13 activity, although initially reduced in these patients, normalized over the course of 12 months and was significantly associated with improved kidney function and reduced risk of adverse renal outcomes.20
Understanding these mechanisms underscores the importance of cautious blood pressure management in hypertensive crises. Overly aggressive reductions can lead to organ hypoperfusion, particularly in patients with chronically elevated autoregulatory thresholds. Therapeutic strategies should aim to mitigate further endothelial injury while allowing autoregulatory mechanisms to stabilize over time.10’18
The management of hypertensive emergencies requires a carefully tailored approach to BP reduction. Intravenous medications with short half-lives are generally preferred, as they allow for precise control and titration while enabling close monitoring of the patient’s response.1,2
It is essential to avoid rapid or excessive BP reductions, as these can lead to complications, including ischemia or further organ damage. Although intravenous therapies are standard in most cases, oral antihypertensive agents, including angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), or beta-blockers, may also be used cautiously in this setting. A stepwise approach using low initial doses helps prevent adverse reactions while achieving effective BP stabilization.1,21
The choice of antihypertensive agent should be guided by the specific type of organ damage, as well as any contraindications to particular drugs or classes.2,21 Among the commonly used agents, labetalol stands out as a versatile and effective option with a favorable safety profile. Its combination of alpha- and beta-blocking properties makes it particularly suitable for a wide range of emergencies, including cases involving catecholamine excess. When administered intravenously, labetalol has a rapid onset of action, allowing for precise titration to achieve the desired BP target.2,22 This property makes it particularly advantageous for conditions such as hypertensive encephalopathy or stroke, as it does not affect cerebral blood flow or increase intracranial pressure.2,23
A retrospective multicenter study investigated the safety of high-dose labetalol in hypertensive crisis.24 The study included 188 patients who received cumulative labetalol doses exceeding the standard recommended maximum of 300 mg within 24 hours. Although adverse events were documented, including bradycardia (36.5%) and hypotension (18.6%), the majority of these incidents were clinically insignificant and did not result in hemodynamic instability. Notably, only 2.7% of patients required rescue medications for refractory adverse events, indicating that high-dose labetalol is generally well-tolerated despite the relatively high incidence of mild bradycardia and hypotension.24
A secondary analysis of the CLUE trial evaluated the comparative efficacy of nicardipine and labetalol for managing hypertensive patients presenting with suspected end-organ damage in emergency department settings.25 The findings revealed that patients receiving nicardipine were significantly more likely to reach the target BP range within 30 min compared to those treated with labetalol (91.4% vs. 76.1%; p = 0.01). In multivariable analysis, nicardipine-treated patients achieved the BP target within 30 min more frequently than patients in the labetalol group (OR 3.65, 95% CI 1.31–10.18).25
The efficacy and safety of intravenous labetalol and nitroglycerin for managing hypertensive crises were compared in a recent randomized clinical trial.26 The authors reported that labetalol achieved target BP control more rapidly than nitroglycerin. Within 1 hour, 96% of patients in the labetalol group reached the BP target, compared to only 44% in the nitroglycerin group. Also, no significant differences were observed between the two groups in terms of adverse events, which included hypotension, bradycardia, and headache. These results highlight the superior efficacy of labetalol in achieving rapid BP reduction in hypertensive emergencies.26
Effective BP management in cerebrovascular emergencies, such as ischemic stroke and intracerebral hemorrhage, requires a nuanced approach tailored to the underlying condition and treatment interventions. The ESC guideline recommendations emphasize balancing the benefits of BP reduction with the risks of compromised cerebral perfusion, particularly in the acute phase.1
In patients with acute ischemic stroke undergoing reperfusion therapy, BP control is critical to minimize the risk of intracranial hemorrhage and other complications. Current guidelines suggest that BP should be lowered to <180/105 mmHg for the first 24 hours post-treatment. This targeted BP reduces the risk of reperfusion injury while preserving adequate cerebral perfusion.1 For patients with ischemic stroke who are not undergoing reperfusion therapy and present with blood pressure levels of ≥220/110 mmHg, a cautious reduction of approximately 15% within the first 24 hours after stroke onset is advised.1
For patients with intracerebral hemorrhage, rapid BP reduction is often essential to prevent hematoma expansion and improve functional outcomes. BP should be lowered to a target range of 140–160 mmHg within the first 6 hours of symptom onset. This approach has demonstrated benefits in reducing the risk of further bleeding without significantly increasing the risk of hypoperfusion or other adverse effects. However, in cases in which systolic BP is ≥220 mmHg, aggressive reductions exceeding 70 mmHg within the first hour are discouraged, as they may lead to additional harm.1
A recent study compared the safety and efficacy of continuous infusion with labetalol and nicardipine for managing BP in patients with acute stroke.27 Both medications were found to be effective in achieving BP control, with no significant difference in the proportion of time spent within the target BP range. However, labetalol demonstrated a shorter time to reach the target BP compared to nicardipine (24 min vs. 40 min; p = 0.021), making it advantageous for situations requiring rapid BP stabilization. Also, nicardipine was associated with a higher incidence of tachycardia compared to labetalol (17% vs. 4%; p < 0.001), which may be a consideration when managing patients at risk of cardiac complications.27
Hypertensive crises during pregnancy, including severe hypertension and preeclampsia, require immediate intervention to mitigate risks to both the mother and fetus. Effective management involves carefully lowering BP while ensuring maternal and fetal safety, with delivery being the definitive treatment for preeclampsia in most cases.1
In the setting of preeclampsia, intravenous labetalol or nicardipine is strongly recommended as first-line therapy for BP control. Magnesium sulfate is also recommended in hypertensive emergencies during pregnancy. The goal of treatment is to reduce systolic BP to below 160 mmHg and diastolic BP to below 105 mmHg within 150–180 min. In cases in which pulmonary edema complicates preeclampsia, intravenous nitroglycerin is recommended as the preferred agent for BP control due to its rapid action and safety in this context.1
A recent multicenter randomized clinical trial compared the effectiveness of nifedipine, labetalol, and hydralazine for managing hypertensive emergencies in patients with severe preeclampsia.28 The study involved 60 pregnant women, who were randomly assigned to one of the three treatment groups. Each participant received up to three doses of the assigned medication within 1 hour. For single-dose administration, nifedipine emerged as the most effective agent, followed by labetalol and hydralazine. Conversely, for triple-dose administration, hydralazine outperformed the other drugs.28 Nifedipine may be preferred for rapid BP reduction with fewer doses, whereas hydralazine is more effective for sustained BP control over multiple doses. Labetalol, although less effective than the other agents in this study, remains a viable option due to its safety profile.28
Tailoring the choice of antihypertensive agent to the clinical scenario and treatment goals is essential for optimizing outcomes in hypertensive emergencies during pregnancy.28
Hypertensive emergencies remain a complex medical challenge, requiring rapid recognition and tailored management strategies. Despite advancements in antihypertensive therapies, the heterogeneity of clinical presentations and underlying mechanisms require an individualized approach to optimize outcomes. The outcomes of hypertensive emergencies continue to emphasize the critical importance of balancing effective blood pressure reduction with the risk of hypoperfusion, particularly in cerebrovascular and pregnancy-related emergencies. Long-term management strategies are essential to prevent recurrence, improve organ function, and reduce cardiovascular morbidity and mortality. Despite progress, significant gaps remain in the understanding of hypertensive emergencies, particularly regarding personalized treatment approaches and the role of emerging biomarkers in guiding therapy. Future research should focus on personalized therapeutic strategies, integrating innovative technologies, and addressing healthcare disparities to improve both, short- and long-term outcomes for patients with hypertensive emergencies.