Acute myocardial infarction is generally a complication of coronary artery disease due to the acute rupture of an unstable atherosclerotic plaque.1,2 Post-traumatic coronary artery dissection is a rare but potentially life-threatening condition, with an estimated prevalence of approximately 0.1%.3 As there is no clear relationship between the severity of chest wall trauma and the extent of coronary lesions, this diagnosis may not be initially considered in the emergency department, mainly due to the broad differential diagnosis4 and the distracting pain symptoms that overlap with cardiac pain in high-energy trauma.5 Furthermore, in cases of low-energy trauma, this diagnosis is even more likely to be missed.6 Coronary artery dissection causes acute myocardial ischemia, with ST-segment elevation and elevated cardiac enzymes. This mimic of acute coronary syndrome is caused by the compression of the true coronary lumen by the false lumen created after trauma.7,8
This study aims to illustrate, through a clinical case, the clinical presentation, diagnostic challenges, and management strategies of traumatic coronary artery dissection leading to acute myocardial infarction, emphasizing the importance of prompt recognition and timely intervention to improve patient outcomes in these rare but critical cases.
A 30-year-old male patient, smoker, with no significant history of cardiovascular disease or other risk factors, presented to the emergency department with localized anterior chest pain following a direct blunt thoracic trauma caused by a pig, which had occurred 2 hours prior to admission.
On physical examination, the patient appeared in mild distress due to the pain, which he described as constrictive, non-radiating, and partially relieved by anti-inflammatory medication. No external signs of thoracic trauma were observed. His vital signs were as follows: blood pressure 156/92 mmHg, heart rate 60 bpm, and oxygen saturation 99% on room air. The clinical examination, including cardiac, pulmonary, abdominal, and renal assessments, was unremarkable.
The initial blood tests revealed leukocytosis (13,400/μL), with marked neutrophilia (12,000/μL), elevated potassium levels (5.39 mmol/L), increased aspartate aminotransferase (227 U/L), and mild hyperglycemia (115 mg/dl). Renal function was within normal limits, and there were no signs of metabolic or respiratory impairment.
Given the nature of the traumatic agent and the location of the pain, a chest radiograph was performed. It excluded rib fractures, pneumothorax, or other acute pulmonary lesions. As part of the general work-up, an electrocardiogram (ECG) was also performed, which unexpectedly revealed ST-segment elevation and Q waves in the inferior leads. Consequently, cardiac biomarkers were measured, showing markedly elevated high-sensitivity troponin I (hs-cTnI, 5,529 ng/L) and creatine kinase-MB (CK-MB, 110.4 ng/mL), suggestive of myocardial injury.
To assess left ventricular function, a transthoracic echocardiogram was performed in the emergency department. Notably, it revealed hypokinesia of the inferior left ventricular wall, with no evidence of pericardial effusion or papillary muscle rupture related to the trauma. To complete the differential diagnosis in this traumatic context, a cardiothoracic computed tomography angiography was performed, which ruled out aortic dissection and pulmonary embolism.
At this point, the differential diagnosis included various causes of acute chest pain, such as acute coronary syndrome, pulmonary embolism, aortic dissection, and pneumothorax. However, considering the elevated serum cardiac enzyme levels, the ECG findings, and the echocardiographic and imaging features, an acute coronary event was considered the most likely cause.
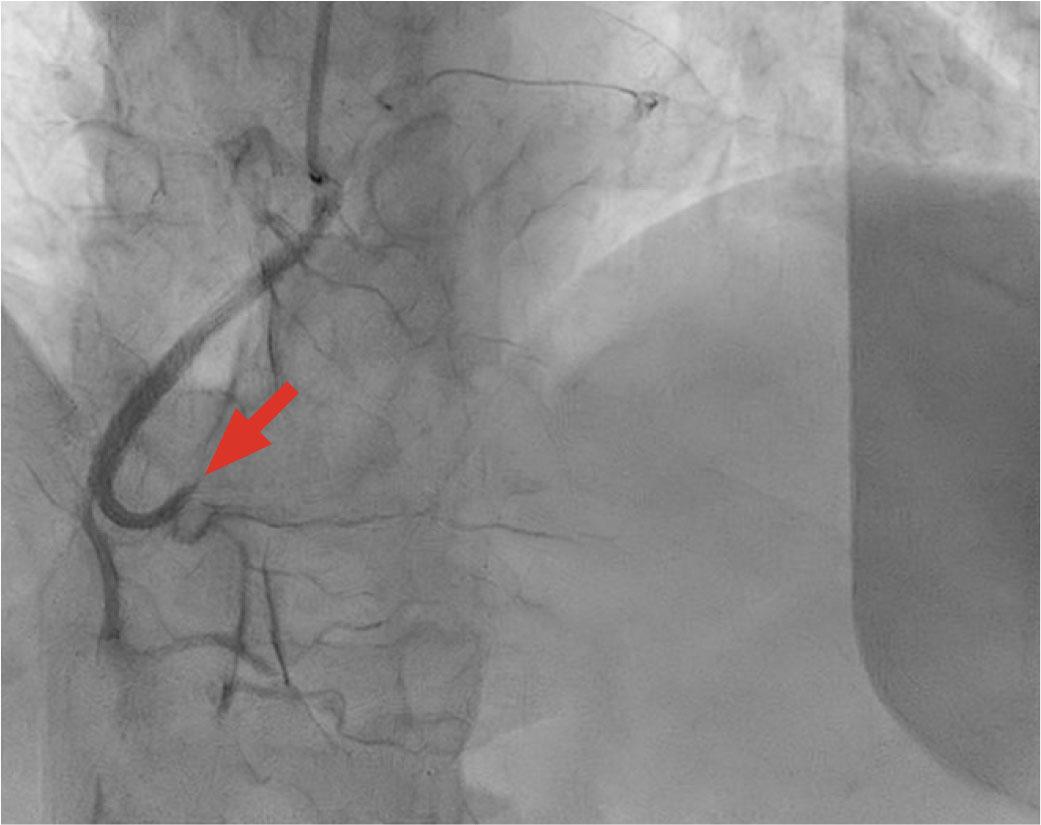
Coronary angiography showing right coronary artery occlusion (arrow).
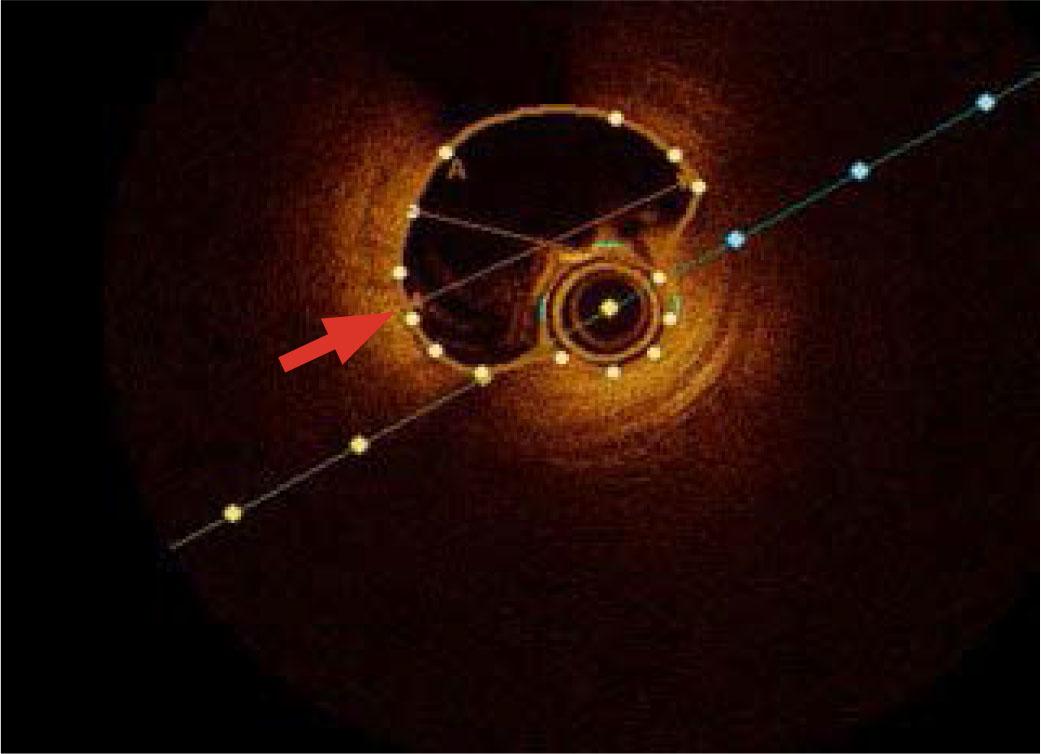
Optical coherence tomography of the right coronary artery revealing coronary dissection with intramural hematoma (arrow).
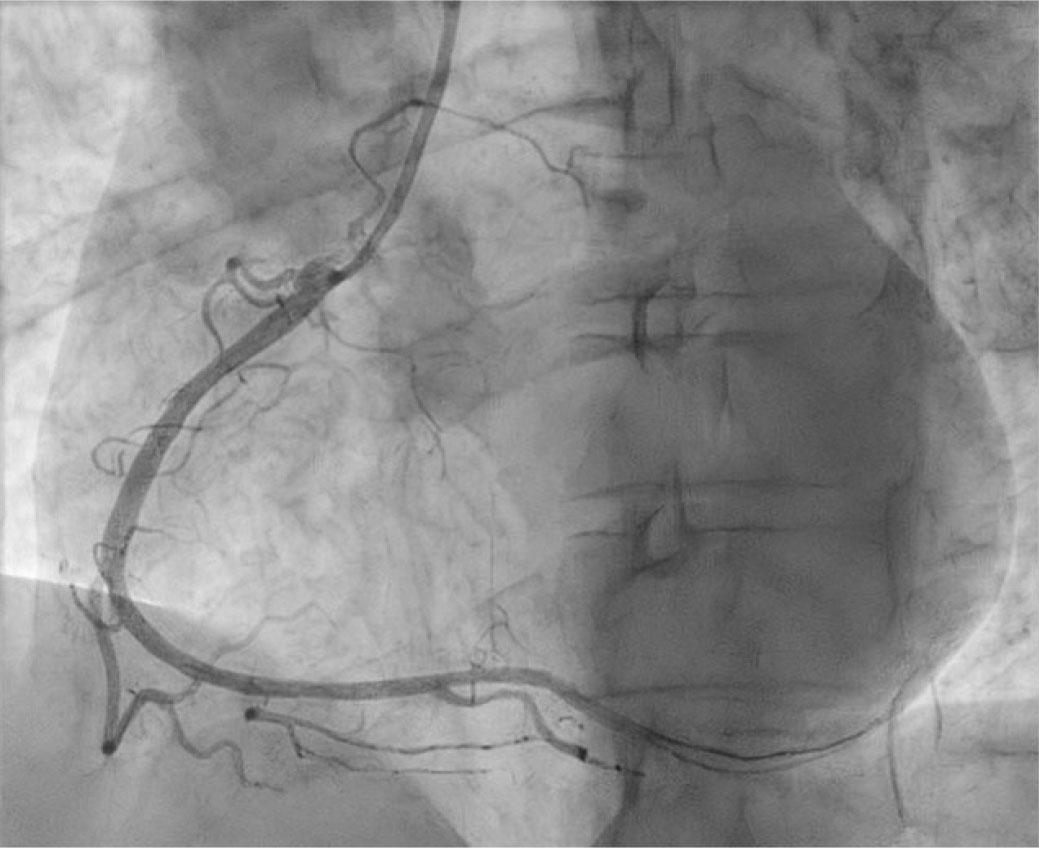
Coronary angiography revealed successful reperfusion of the right coronary artery.
Considering the patient's young age and the severity of the acute presentation, he was transferred to the catheterization laboratory, where a coronary angiography was performed. The angiogram revealed occlusion of the right coronary artery at the crux cordis, likely due to a posttraumatic intramural hematoma, with no distal flow (Figure 1). The left coronary system appeared angiographically normal. To further investigate the cause of the right coronary artery occlusion, optical coherence tomography was performed, which confirmed a coronary dissection with an intramural hematoma (Figure 2). Consequently, a drug-eluting stent (DES Xience pro 3 × 38 mm) was implanted, successfully restoring full vessel patency (Figure 3).
Following the procedure, the patient was monitored in the intensive care unit. He was started on double antiplatelet therapy with aspirin (75 mg daily) and ticagrelor (90 mg twice daily), along with lipid-lowering therapy (rosuvastatin 20 mg once daily) and a beta-blocker (metoprolol 25 mg twice daily). Adequate antibiotic prophylaxis was administered, and intravenous fluids were given to maintain proper hydration and renal perfusion.
Traumatic coronary artery dissection is a rare and life-threatening condition resulting from blunt chest trauma. The mechanisms underlying arterial dissection include intraluminal thrombosis or hematoma, often associated with intimal tearing due to increased shear forces on the endothelium and elevated coronary blood pressure secondary to heightened sympathetic activity.6
Although coronary artery dissection is more commonly associated with high-energy impacts, there is no clear relationship between the intensity of thoracic trauma and the development of coronary lesions. Coronary injury has also been reported following low-speed collisions, as was the case in our patient.3,4
The major clinical consequence of right coronary artery dissection is acute myocardial infarction due to subtotal or complete occlusion of the coronary lumen.9 Our patient presented with constrictive anterior chest pain and elevated cardiac enzyme levels, findings suggestive of an acute coronary event. The presence of ST-segment elevation and Q waves in the inferior leads on the ECG raised strong suspicion for myocardial infarction and warranted emergency coronary angiography.
Although coronary angiography remains the main diagnostic approach, it provides only two-dimensional images of the coronary arteries, without the ability to directly visualize the intravascular lumen, which is a significant limitation in identifying the precise cause of dissection. Consequently, we performed optical coherence tomography to accurately visualize the location of the coronary dissection and the morphology of the residual intramural hematoma. Additionally, this imaging technique played an important role in guiding interventional treatment decisions. It facilitated the selection of an appropriate stent type and ensured its proper positioning against the arterial wall.6
Despite the reduced ventricular function observed at presentation, which is typically associated with a poor prognosis,10 a pre-discharge echocardiographic examination revealed preserved ventricular function and no wall motion abnormalities. This underscores the importance of prompt diagnosis and timely interventional treatment in achieving a favorable patient outcome.
In conclusion, coronary artery dissection in the context of acute thoracic trauma is a diagnosis that must be considered in the emergency department because of the severe and potentially life-threatening consequences that may occur if prompt intervention is not undertaken.