
Acute limb ischemia (ALI) and chronic limb-threatening ischemia (CLTI) are severe vascular conditions that can lead to amputation and even death if left untreated.1,2 ALI is characterized by a sudden blockage of arterial blood flow, which can cause pain, loss of function, and skin pallor.1 CLTI is the final stage of peripheral arterial disease and is characterized by symptoms such as persistent pain, trophic disorders, and impaired mobility.2
The inflammatory state that dominates ALI increases the number of neutrophils, which are the primary responders to the site of injury, and platelets that adhere to the activated endothelium.3 Additionally, numerous articles have demonstrated that neutrophils have an essential role in the acute phase of certain thromboembolic events, such as myocardial infarction,4,5,6 both in patient cohorts4 and in experimental models.5,6 Furthermore, the crucial role of lymphocytes in both the inflammatory and repair phase following an acute event is well established.7,8
The neutrophil-to-lymphocyte ratio (NLR) biomarker has gained significant attention due to its ability to indicate poor outcomes in patients with various diseases. It is derived from the total number of neutrophils and lymphocytes and is a prognostic factor in end-stage kidney disease,9,10,11 atherosclerotic diseases,12,13 COVID-19,14–16 and other pathologies.17,18 Additionally, it was demonstrated that the COVID-19 pandemic led to an increase in the incidence of patients with ALI19 as well as thromboembolic events,20,21,22,23,24,25,26 and recently, Arbănași et al.16 demonstrated that high NLR values are associated with the risk of developing ALI in a cohort of 510 patients with COVID-19.
The aim of this systematic review was to analyze the prognostic role of the NLR regarding the risk of amputation and mortality in patients diagnosed with ALI and CLTI.
We carried out a systematic review of the literature according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, using articles from the PubMed database and the search terms ‘acute limb ischemia’ or ‘chronic limb-threatening ischemia’ and ‘NLR’.
Two independent reviewers (B.L. and E.R.) conducted the literature search. We included all articles with relevant titles published from January 1, 2010 to January 1, 2023. Only articles published in English were considered. Studies written in languages other than English, studies unrelated to this topic or with insufficient data, as well non-confirmatory cases and duplicate articles were excluded.
We found 2,301 articles that met the search criteria and added eight articles from the reference lists of these articles. We excluded 835 duplicates and 1,449 articles that did not meet the inclusion criteria. From the remaining 25 articles we excluded seven with unclear methodology, four diagnostic-type studies, and two articles that involved patients with COVID-19. The PRISMA flow chart of the investigation plan is shown in Figure 1.
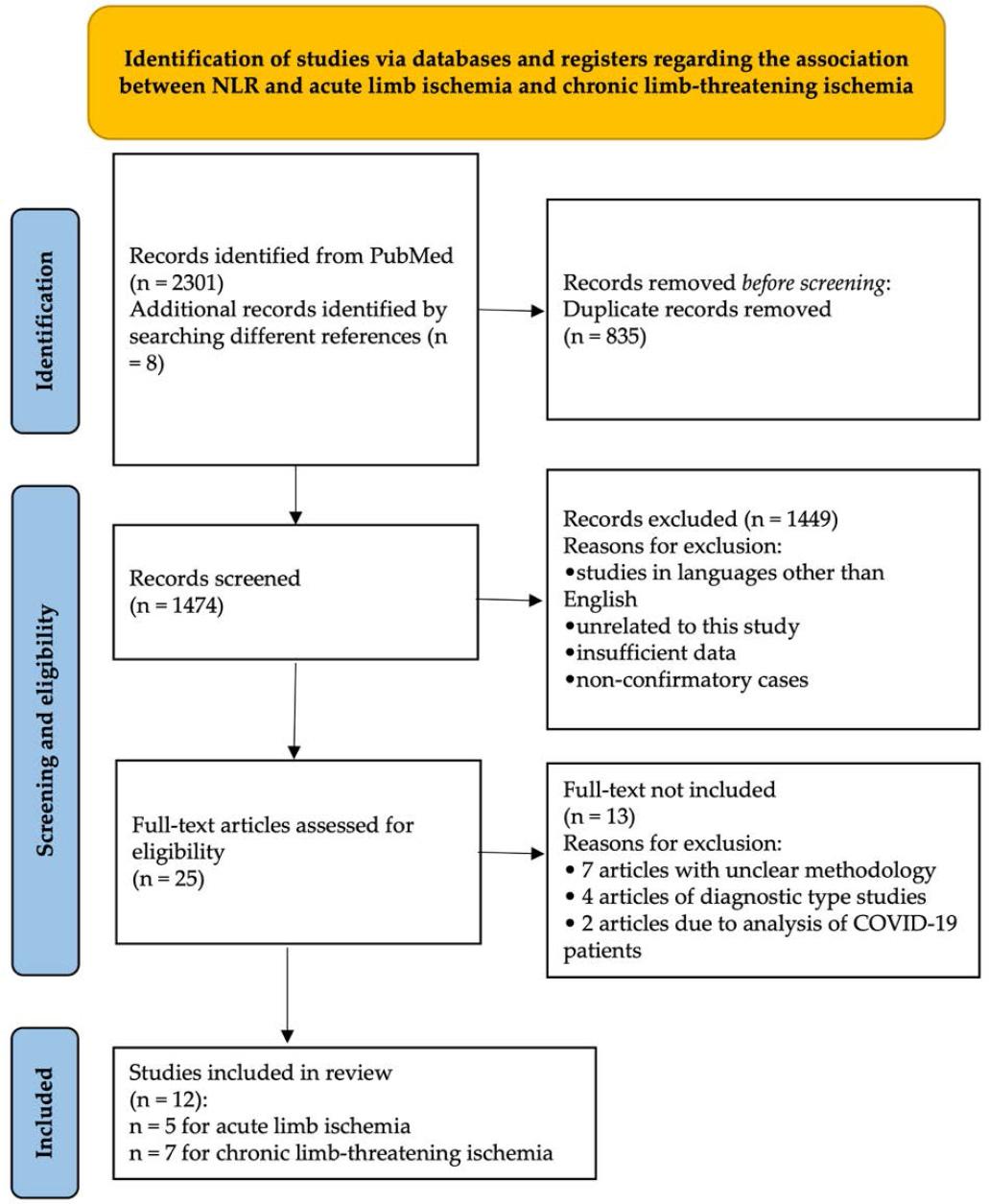
PRISMA flow chart of studies included in the systematic review
We included 12 studies in this systematic review, of which five were related to ALI, with a total of 1,145 patients, and seven were related to CLTI, with a total of 1,838 patients.
In terms of demographic data, the average age of patients with ALI was 73.06 years (range 66–79), with 717 (62.62%) of these patients being male. The average age of patients with CLTI was 71.96 years (range 64–81), with 1,282 (69.75%) being male. In terms of comorbidities, 869 patients with ALI (75.9%) had hypertension, 387 (33.8%) had diabetes, 371 (32.4%) had ischemic heart disease, and 458 (40%) were active smokers. Of the patients with CLTI, 1,151 (62.62%) had hypertension, 844 (45.92%) had diabetes, 643 (34.98%) had ischemic heart disease, and 992 (53.97%) were active smokers (Table 1).
The general characteristics of the studies included in the review
| Study | Year | Country | No. of patients | Mean age (years) | Male sex, n (%) | Hypertension, n (%) | Ischemic heart disease, n (%) | Diabetes, n (%) | Active smoking, n (%) |
|---|---|---|---|---|---|---|---|---|---|
| ALI | |||||||||
| Taşoğlu et al.27 | 2013 | Turkey | 245 | 66.04 | 152 (62%) | 144 (59%) | – | 60 (24%) | 170 (70%) |
| Coelho et al.28 | 2021 | Portugal | 345 | 73 | 188 (54.5%) | 277 (83.5%) | 157 (45.5%) | 92 (27.5%) | 136 (39.4%) |
| Taurino et al.29 | 2021 | Italy | 177 | 78.9 | 115 (65%) | 145 (81.9%) | – | 70 (39.5%) | – |
| Pasqui et al.30 | 2021 | Italy | 168 | 77.8 | 109 (64.9%) | 128 (76.1%) | 45 (26.7%) | 54 (32.1%) | 18 (10.7%) |
| Arbănași et al.31 | 2022 | Romania | 210 | 69.56 | 153 (72.86%) | 175 (83.33%) | 169 (80.48%) | 111 (52.86%) | 134 (63.81%) |
| CLTI | |||||||||
| Spark et al.32 | 2010 | UK | 149 | 72 | – | 83 (55.7%) | – | 44 (29.53%) | 103 (69.12%) |
| Chan et al.33 | 2014 | Australia | 97 | 81 | 50 (64.9%) | 42 (54.6%) | 49 (63.6%) | 46 (59.7%) | – |
| Gonzalez-Fajardo et al.34 | 2014 | Spain | 561 | 74 | 465 (83%) | 354 (63.10%) | 131 (23.35%) | 258 (45.98%) | 362 (64.52%) |
| Erturk et al.35 | 2014 | Turkey | 508 | 64 | 413 (81.3%) | 311 (61.22%) | 207 (40.74%) | 213 (41.92%) | 266 (52.36%) |
| Taşoğlu et al.36 | 2014 | Turkey | 104 | 69 | 86 (82.7%) | 46 (44.2%) | – | 39 (37.5%) | 74 (71.2%) |
| Su et al.37 | 2021 | Taiwan | 195 | 74 | 102 (52.3%) | 129 (66.15%) | 75 (38.46%) | 134 (68.71%) | 46 (23.58%) |
| Russu et al.38 | 2022 | Romania | 224 | 69.72 | 166 (74.11%) | 186 (83.04%) | 181 (80.8%) | 110 (49.11%) | 141 (62.95%) |
The disease etiology, treatment, and outcomes of the 1,145 patients with ALI are presented in Table 2. The disease had an embolic etiology in 521 patients (45.5%) and a thrombotic etiology in 434 patients (37.9%). As far as localization is concerned, 588 patients (51.35%) presented a thrombosis located at the femoral-popliteal axis, 123 (10.74%) at the aorto-iliac axis, and 35 (3.06%) below the knee artery. Treatment included embolectomy in 62.62% (n = 717), bypass in 9% (n = 103), and hybrid techniques or other treatments in 9.61% (n = 110) of patients. Regarding the outcomes, 19.04% (n = 218) had to undergo major amputation after surgery, and 15.55% (n = 178) did not survive.
Disease etiology, treatment, and outcomes of patients with ALI
| Study | Study group value | Control group value | Cut-off value | AUC/ROC analysis | Sensitivity (%) | Specificity (%) | Outcome |
|---|---|---|---|---|---|---|---|
| ALI | |||||||
| Taşoğlu et al.27 | 9.7 | 6.1 | 5.2 | 0.7 | 63% | 63% | Amputation |
| Coelho et al.28 | 8.8 | 3.6 | 5.4 | 0.860 | 90.5% | 73.6% | Death or major amputation at 30 days |
| Taurino et al.29 | – | – | 5 | 0,823 | – | – | Amputation at 30 days |
| – | – | 5 | 0.776 | – | – | Mortality at 30 days | |
| Pasqui et al.30 | 8.9 | 6.5 | 6.66 | 0.712 | 77.8% | 65.3% | Amputation at 26.9 ± 22.1 months |
| 8.08 | 5.6 | 5.57 | 0.639 | 62.3% | 56.04% | Mortality at 26.9 ± 22.1 months | |
| Arbănași et al.31 | 5.78 | 2.61 | 4.23 | 0.829 | 70.2% | 83% | Major amputation at 30 days |
| CLTI | |||||||
| Spark et al.32 | – | – | 5.25 | 0.690 | 69% | 71% | Mortality at 8.7 months (3.1–16 months) |
| Chan et al.33 | – | – | 5.25 | – | – | – | Mortality at 12 months |
| Gonzalez-Fajardo et al.34 | – | – | 5 | 0.64 | 32% | 87.5% | Amputation-free survival at 31 months |
| Erturk et al.35 | – | – | 3 | – | – | – | Cardiovascular death at 20 months (12–27 months) |
| Taşoğlu et al.36 | 3.8 | 2.4 | 3.2 | 0.71 | – | – | Major amputation at 46 months |
| Su et al.37 | – | – | 8 | – | 62% | 82.1% | Mortality at 12 months |
| Russu et al.38 | 6.40 | 2.21 | 3.95 | 0.821 | 82.6% | 89.9% | Primary patency at 12 months |
The results of the receiver operating characteristic (ROC) analysis specific to each study are presented in Table 3. In patients with ALI, the average optimal cut-off value of NLR was 5.49 (range 4.23–6.66), with an average area under the curve (AUC) of 0.730 (range 0.639–0.860), an average sensitivity of 70.10%, and a specificity of 68.11 %. In patients with CLTI, the average optimal cut-off value of NLR was 4.8 (range 3.2–8), with an average AUC of 0.715 (range 0.640–0.821), an average sensitivity of 61.4%, and a specificity of 82.62%.
Clinical cases and surgical procedures for ALI
| Study | Cause | Location | Treatment | Complication | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Embolic, n (%) | Thrombotic, n (%) | Aorto-iliac, n (%) | Femoral-popliteal axis, n (%) | Below the knee artery, n (%) | Embolectomy, n (%) | Bypass, n (%) | Other, n (%) | Amputation, n (%) | Mortality, n (%) | |
| Taşoğlu et al.27 | 224 (92%) | 21 (8%) | 44 (18%) | 189 (78%) | – | 224 (92%) | 21 (8%) | – | 36 (14.69%) | 25 (10%) |
| Coelho et al.28 | 157 (45.5%) | 188 (54.5%) | 60 (17.4%) | 261 (75.7%) | 24 (7%) | 280 (81.2%) | 35 (10.1%) | 30 (8.7%) | 84 (24.34%) | – |
| Taurino et al.29 | 73 (41.3%) | 104 (58.7%) | – | – | – | 95 (53.7%) | 9 (5.1%) | 73 (41.2%) | 23 (12.9%) | 29 (16.4%) |
| Pasqui et al.30 | 67 (39.9%) | 121 (60.1%) | 19 (11.3%) | 138 (82.1%) | 11 (6.5%) | – | – | – | 18 (10.7%) | 77 (45.8%) |
| Arbănași et al.31 | – | – | – | – | – | 118 (72.39%) | 38 (23.31%) | 7 (4.29%) | 57 (27.14%) | 47 (22.38%) |
In this systematic review, we examined the role of NLR in the post-revascularization progression of patients with ALI and CLTI. We found that high NLR values are associated with an increased risk of amputation and/or mortality, with pooled odds ratios ranging from 1.28 to 11.09 in patients with ALI, and from 1.97 to 5.6 in patients with CLTI. Additionally, the ROC analysis identified optimal cut-off values for NLR, with a narrow distribution. The average cut-off value was 5.49 (range 4.23–6.66) for patients with ALI and 4.8 (range 3.2–8) for patients with CLTI.
This biomarker has already been proven to be useful in the prediction of poor outcomes in the context of other vascular diseases such as stroke, acute pulmonary embolism, abdominal aortic aneurysm, and numerous cardiac pathologies. In a study involving 448 patients with acute ischemic stroke,39 Chen et al. analyzed the relationship between NLR and outcomes, and demonstrated that high NLR values are associated with poor functional outcomes 3 months after the index events, identifying an optimal cut-off value of 3.51 (78.1% sensitivity and 83.2% specificity). Similarly, in a study involving 116 patients with stroke, Brooks et al.40 demonstrated that high NLR values at admission are associated with poor recovery and mortality following endovascular therapy. More recently, Xu et al.41 identified in a cohort of 341 of patients diagnosed with stroke that a baseline value of NLR higher than the optimal cut-off value of 4.21 (52.7% sensitivity and 72% specificity) is associated with the risk of stroke progression in the first week after admission.
Another vascular pathology in which the prognostic role of NLR has been demonstrated is abdominal aortic aneurysm (AAA).42,43,44 Kardzadeh et al.42 have shown in a cohort of 80 patients with ruptured AAA that high preoperative values of NLR (OR 4.28, p = 0.02) are associated with the risk of morbidity 30 days post operation. Similarly, Aurelian et al.43 have shown that NLR values above the cut-off value of 5 are associated with a five times higher risk of AAA rupture. In a cohort of 350 patients, Appleton et al. demonstrated that preoperative NLR values greater than 5 are associated with 30-day mortality (p = 0.0007) and 10-year mortality (p = 0.043) after AAA repair.
Regarding cardiac pathology, numerous studies have examined the local and systemic inflammatory response in the remodeling of cardiac function and poor outcomes of patients with acute coronary syndrome.6,45,46,47,48,49,50 However, the cost of identifying these biomarkers is high and their availability in current practice is very limited; hence, NLR has recently been intensively analyzed and studied.51,52,53,54,55,56
This systematic review emphasizes the importance of NLR in the prognosis of both ALI and CLTI. Elevated NLR levels were consistently associated with an increased risk of amputation and death. This indicates that NLR may serve as a useful tool for decision-making in the management of these patients.