
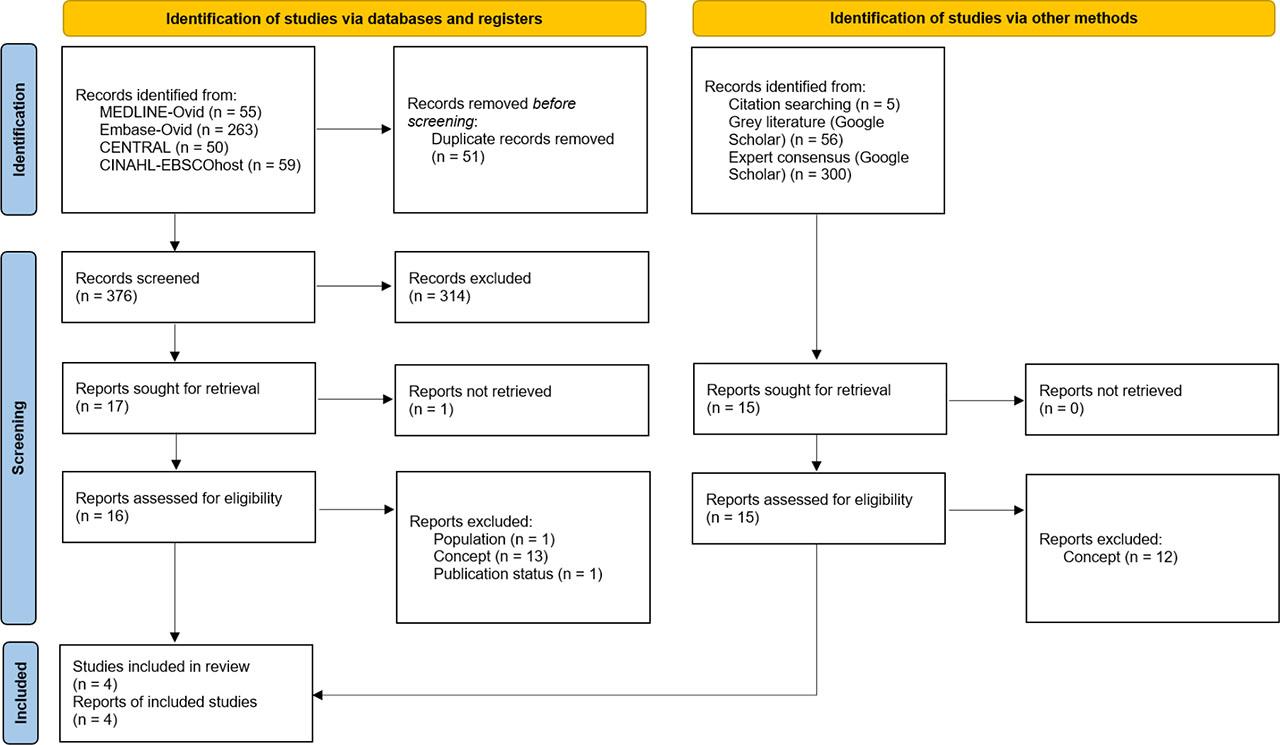
Fig. 1.
Strategy for discontinuing enteral tube feeding during chest physiotherapy
| Id | Strategy | Timing | Adverse events | Limitations |
|---|---|---|---|---|
| Savio 2020 [28] | Interruption of enteral feeding during chest physiotherapy in prone or supine MV patients | Chest physiotherapy was counted as a procedure in the ICU. Interruption of enteral feeding due to ICU procedures accounted for 72% of the total time in prone patients and 41% in supine patients | No patient experienced vomiting or nausea while in the prone position, but there were 12 instances of vomiting or nausea in the supine position. | The study fails to establish a direct connection between vomiting events and the administration of chest physiotherapy |
| van der Lee 2019 [29] | If the head-down tilt position is used to minimise the risk of aspiration of gastric contents into the lungs, it is best to either stop enteral feeds or ensure the stomach is emptied by aspirating the nasogastric tube | For at least 30 minutes before positioning | Not applicable | Not applicable |
| van der Lee 2020 [30] | If the head-down tilt position is used to minimise the risk of aspiration of gastric contents into the lungs, it is best to either stop enteral feeds or ensure the stomach is emptied by aspirating the nasogastric tube | For at least 30 minutes before positioning | Not applicable | Not applicable |
| van der Lee 2024 [31] | If the head-down tilt position is used, the enteral feed should either be withheld or the nasogastric tube aspirated to empty the stomach, to minimise the risk of aspiration of gastric contents into the lungs (Conditional recommendation; GRADE certainty of evidence: Very low) | For at least 30 minutes before positioning | Not applicable | Not applicable |
Characteristics of included studies
| Id | Design | Objective | Inclusion and exclusion criteria | Outcomes assessed |
|---|---|---|---|---|
| Savio 2020 [28] | Prospective observational study | To assess the feasibility, tolerance, and effectiveness of enteral nutrition in critically ill patients receiving invasive MV in the prone position for severe ARDS | Inclusion: Adult patients with ARDS who underwent invasive MV in the prone position. | Feasibility and tolerance of enteral nasogastric feeding |
| Exclusion: Patients who were not fed enterally due to significant hemodynamic instability | ||||
| van der Lee 2019 [29] | Expert consensus (modified Delphi technique) | To determine an expert consensus for respiratory physiotherapy management of intubated and mechanically ventilated adults with community-acquired pneumonia | Inclusion: minimum of 5 years as a qualified physiotherapist and a minimum of 3 years of experience in critical care and either (a) met the standards for qualification of “specialist” in cardiorespiratory physiotherapy within the Australian Physiotherapy Association or (b) had a minimum of 2 years of experience working in a senior position within critical care or a minimum of five publications on critical care physiotherapy (including coauthor) | Consensus statements for respiratory physiotherapy in adults with community-acquired pneumonia on MV. The statements were grouped into Physiotherapy assessment, Physiotherapy treatment, 2.1) Positioning, 2.2) Hyperinflation techniques, 2.3) Manual chest wall techniques, 2.4) Normal saline instillation, and 2.5) Active modes of treatment and mobilisation |
| van der Lee 2020 [30] | Qualitative mixed methods study | To conduct a peer review of the expert consensus statements for respiratory physiotherapy management of community-acquired pneumonia to determine their acceptability to Australian multidisciplinary ICU staff and to explore what adaptations might be required to enable them to be developed into a relevant and useful guideline for clinical practice | Senior medical, nursing and physiotherapy clinicians working in an Australian Level 2 or 3 ICU | Clinical validity and applicability of the expert consensus statements (van der Lee 2019). New factors perceived by participants to influence the application of the consensus statements into clinical practice |
| van der Lee 2024 [31] | Clinical practice guideline | To develop a clinical practice guideline for physiotherapy management of adults invasively ventilated with community-acquired pneumonia using the best available evidence | Not applicable | Twenty-six recommendations for clinical physiotherapy practice |