
Fig. 1.
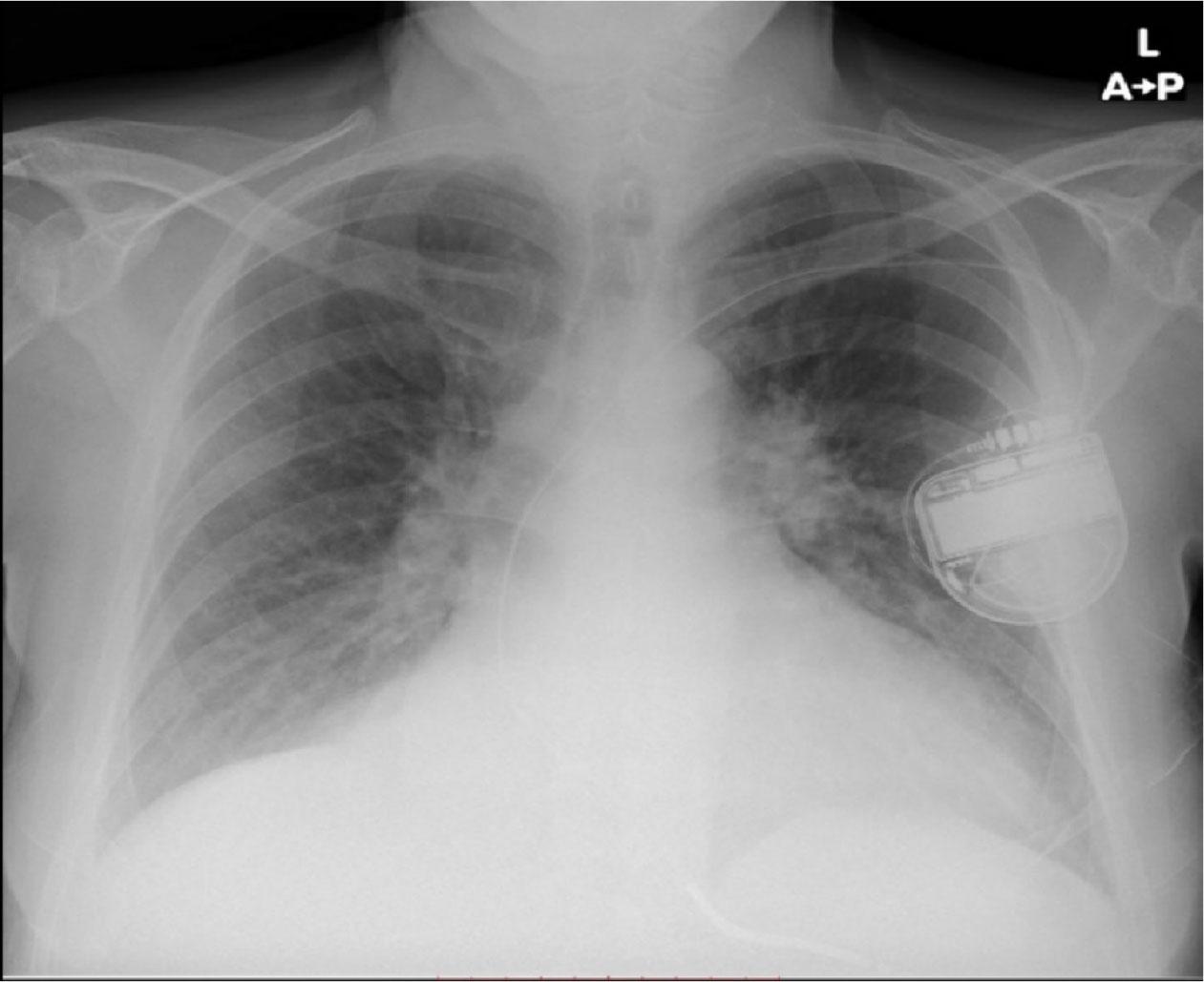
Fig. 2.
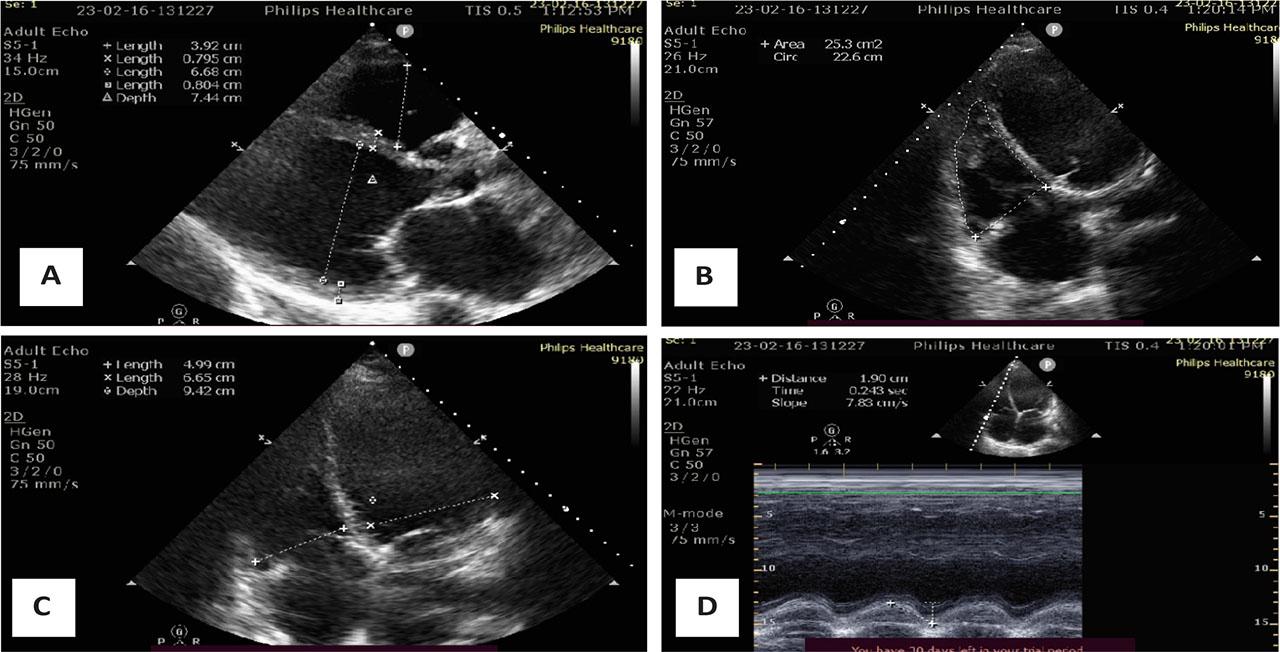
Fig. 3.
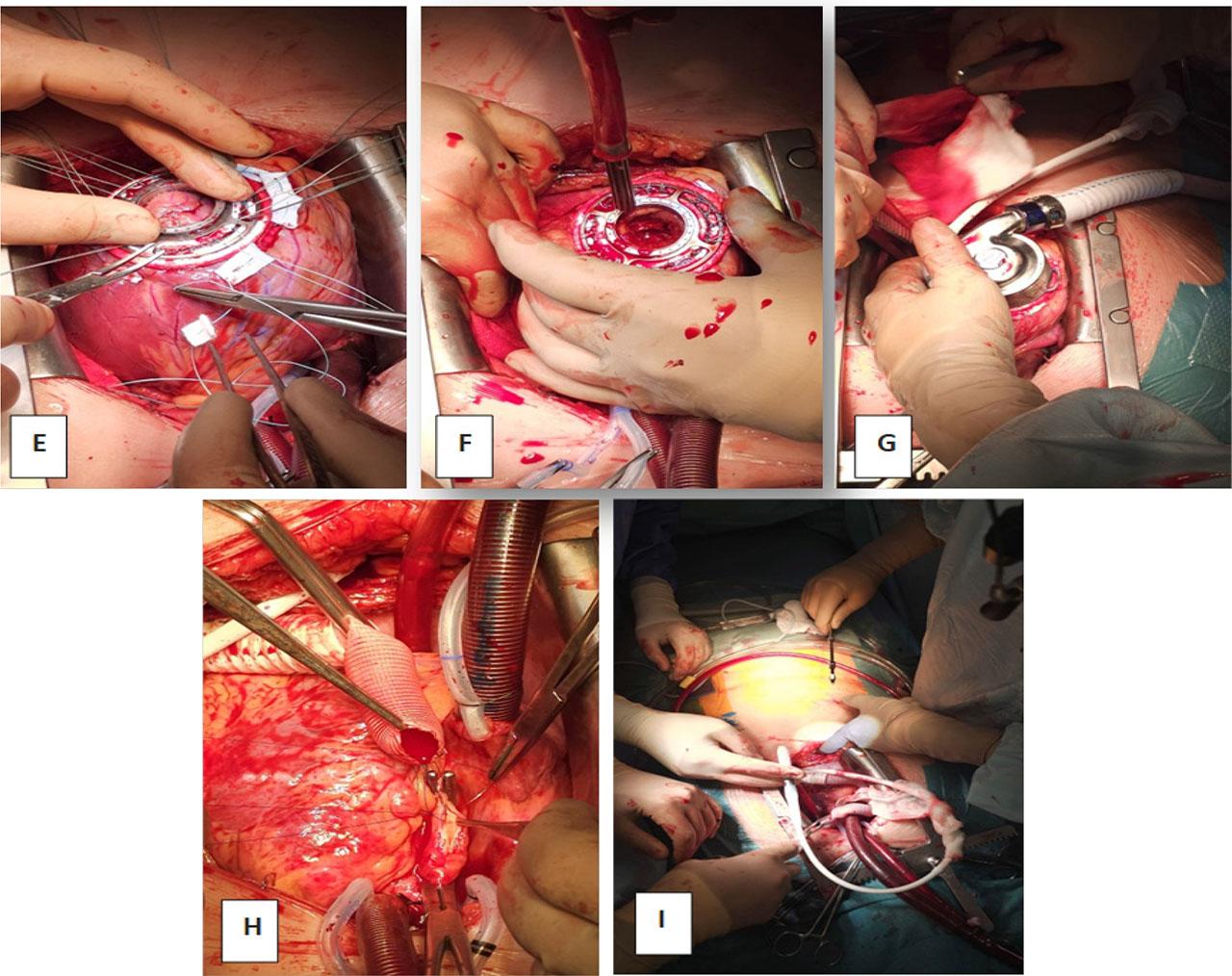
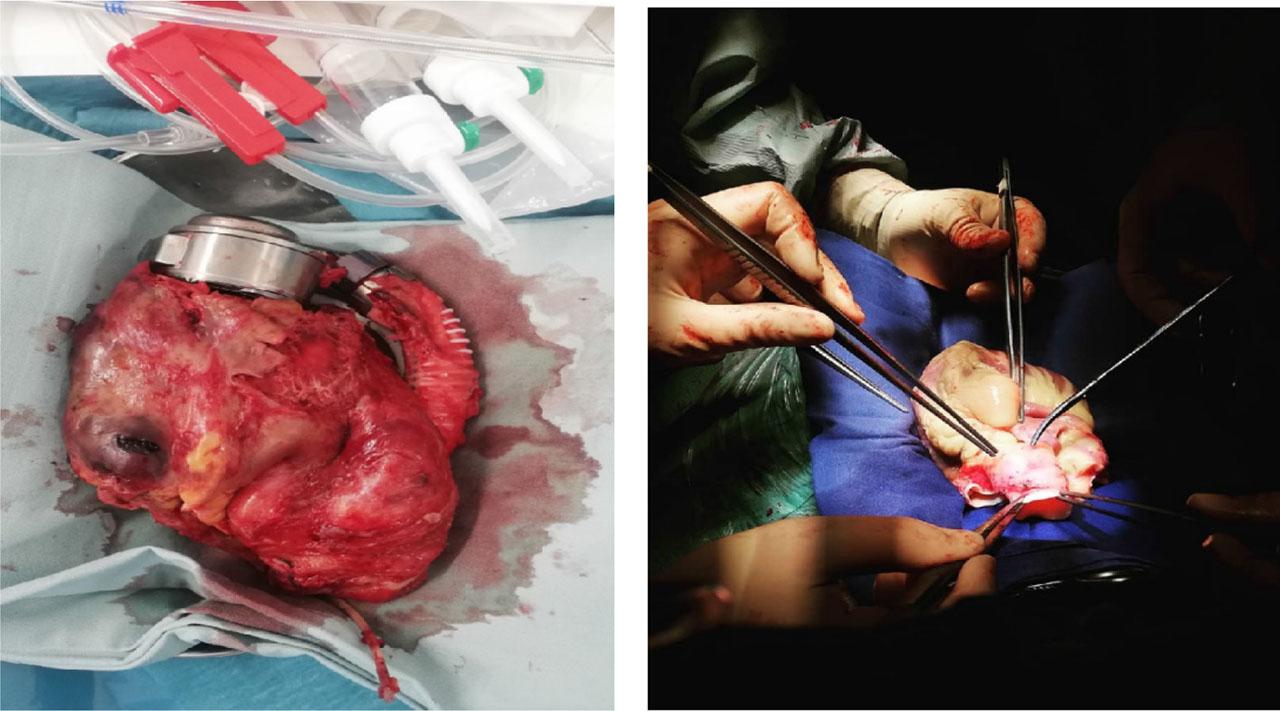
Fig. 4.
Timeline of Clinical Events
| Day / Time Point | Event / Intervention |
|---|---|
| 05.01.2023 | Re-hospitalization for acute heart failure, initiation of inotropic support |
| 15.02.2023 | Transfer to our center on Dobutamine and Furosemide continuous infusion |
| Admission Day | Severe hemodynamic instability, metabolic acidosis, renal dysfunction |
| Day 2–3 | Progressive decline despite escalation of inotropes; start of Levosimendan |
| Day 5 | Development pleural effusion; right thoracentesis (520 mL evacuated) |
| Day 7 | Worsening hemodynamics, need for non-invasive ventilation (CPAP) |
| Day 8 | Intubation, mechanical ventilation, renal replacement therapy initiated |
| Day 10 | INTERMACS II profile confirmed |
| Day 11 | HeartMate 3 LVAD implantation |
| Post-op Day 1–8 | Persistent right ventricular failure, high-dose inotropic and vasopressor support |
| Post-op Day 22–25 | Severe RV dysfunction persists; recurrent arrhythmias; hemodynamic instability |
| Day 27 | Heart transplantation performed |
| Post-TX Day 3 | Successful extubation |
| Post-TX Day 4 | Weaning off inotropes |
| Post-TX Day 13 | ICU discharge |
| Post-TX Day 44 | Hospital discharge |
| 4 Months Post-TX | Severe neutropenia, acute kidney injury; management and recovery |
| 6 Months Post-TX | Asymptomatic, stable graft function (ISHLT 0) |
| 7 Months Post-TX | Lobar pneumonia; antibiotic treatment and recovery |
| 2 Years post-TX | Excellent clinical condition, active lifestyle |