
Fig. 1.
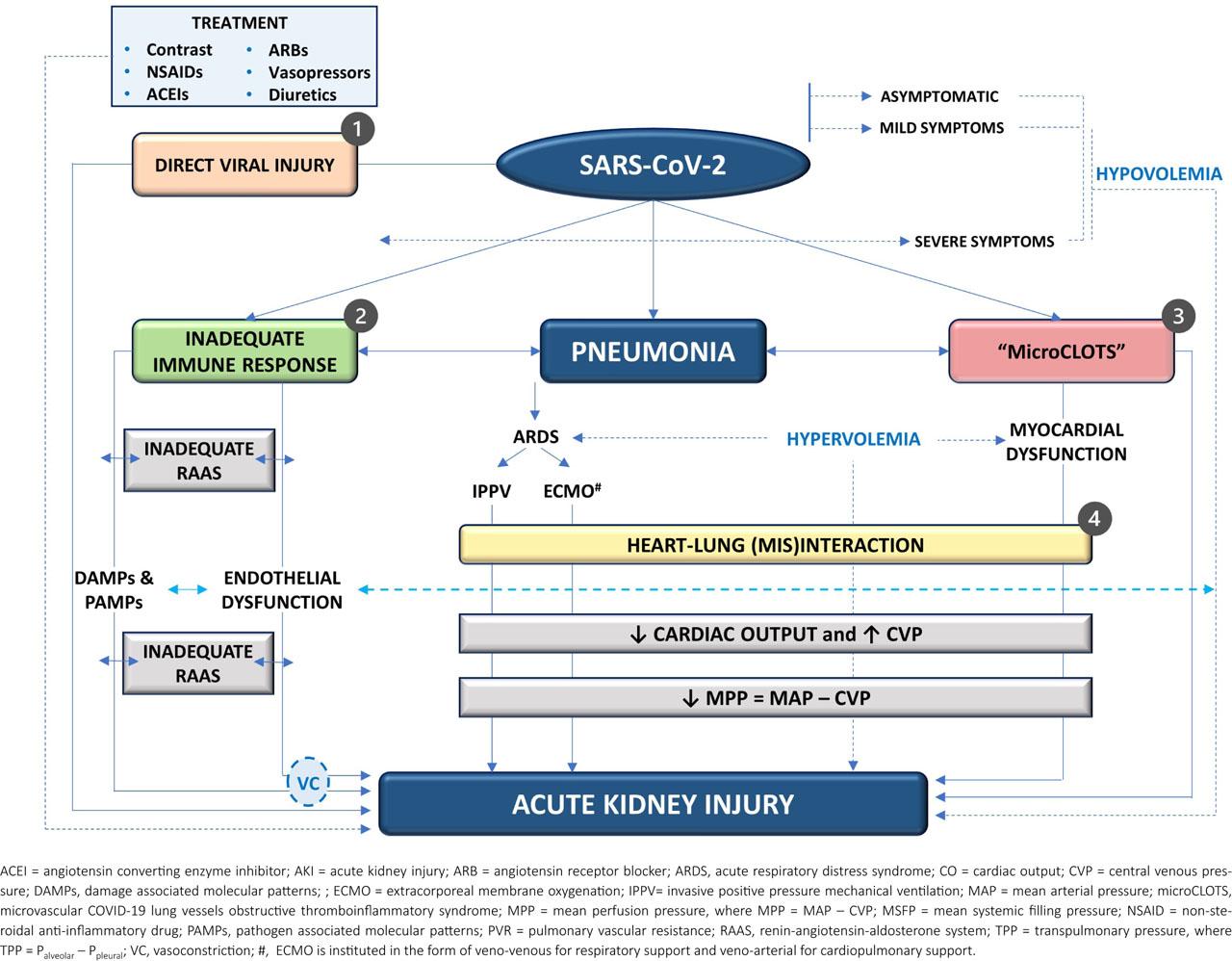
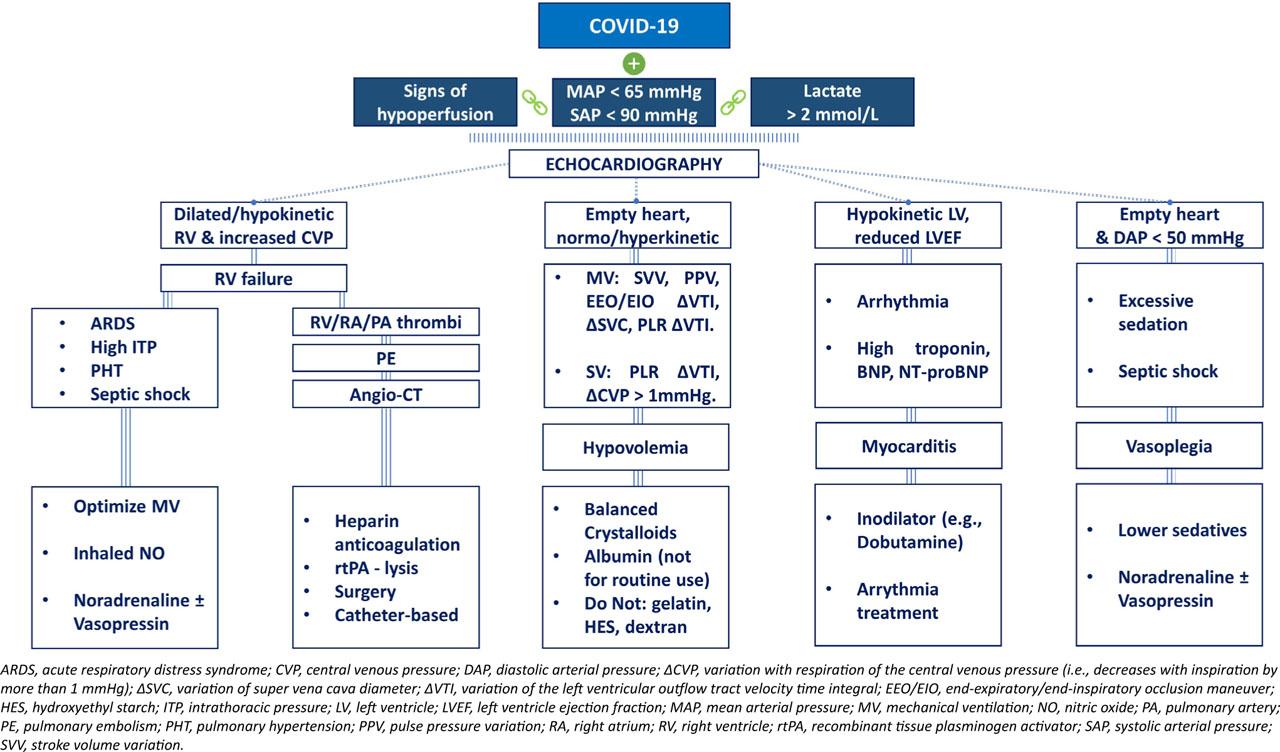
Fig. 2.
CARDS phenotyping – a mechanistic overview_
| Criterion | CARDS subphenotype | |
|---|---|---|
| L subphenotype | H subphenotype | |
| Pulmonary mechanics | EL and ECW are normal | EL is increased and ECW is normal |
| Computer Tomography | Aerated | Dependent atelectasis |
| Histopathologic substrate | microCLOTS | Diffuse alveolar damage |
| Gas exchange abnormality | V/Q mismatch | Shunt |
| Positive pressure transmission Ppleural = Palveolar × (ECW/ET) | Mainly in the pleural space | Mainly transpulmonary |
| Cardiac effects | RV preload is reduced | RV afterload is increased |
| Renal effects | Decreased arterial flow | Decreased arterial flow |
| Respiratory strategy | Low recruitment potential | High recruitment potential |
| Hemodynamic strategy | Prevent fluid overload. | Reduce lung water. |
| Hemodynamic monitoring | Ultrasound | Ultrasound |
Preventive measures in COVID-AKI
| Intervention | Argument | Recommendation |
|---|---|---|
| Renal function | Staging AKI and assessing clinical risk are epidemiological imperatives with crucial therapeutic implications. | Recommend the use of serum creatinine and urine output for monitoring renal function, paying attention to limitations of both parameters. |
| Hemodynamic profiling | Inadequate tissue perfusion contributes to the worsening of organ dysfunction (e.g., kidney, lung, liver, and heart). | Recommend an individualized hemodynamic strategy based on dynamic and quantitative indices of cardiovascular evaluation. (Level of evidence: 1B) |
| Fluids | Fluid composition has systemic consequences, including renal. High chloride content was associated with an increased incidence of AKI, and the use of hydroxyethyl starch derivatives in sepsis is contraindicated. | Recommend the use of balanced crystalloids for initial volume resuscitation in at-risk patients or those who develop COVID-AKI, in the absence of other specific indications. (Level of evidence: 1A) |
| Glycemic control | Insulin resistance and hypercatabolism are frequently encountered in patients with COVID-19. | Suggest the use of an intensive glycemic control strategy. (Level of evidence: 2C) |
| Nephrotoxins | Various nephrotoxins are commonly prescribed to patients with COVID-19. | Recommend limiting exposure to nephrotoxic medications and vigilant monitoring when they cannot be avoided. (Level of evidence: 1B) |
| Contrast agents | The relevance of contrast agent toxicity is uncertain. | Recommend optimizing intravascular volume as the only preventive measure. (Level of evidence: 1A) |
| Mechanical ventilation | Increased intrathoracic pressure results in: 1) elevated central venous pressures and peripheral venous congestion; 2) sympathetic adrenergic and renin-angiotensin-aldosterone system activation; 3) mechanical disadvantage, particularly for the right ventricle; 4) renal, hepatic, and splanchnic cross-talk. | Suggest the use of a protective ventilatory strategy for both the lungs and the right ventricle, individualized and continuously tailored to the patient's real-time physiology. (Level of evidence: 2C) |
Potential risk factors associated with COVID-AKI
| Socio-demographic risk factors | Risk factors at admission | Post-admission risk factors |
|---|---|---|
| Advanced age (> 70 years) | Elevated viremia | Nephrotoxins (e.g., contrast agents) |
| Diabetes mellitus | Leukocytosis and lymphopenia | Vasopressors |
| Hypertension | Increased levels of ferritin, CRP, and D-dimers | Mechanical ventilation |
| Congestive heart failure | Hypovolemia/dehydration | Hypovolemia |
| Obesity | Multiorgan involvement | Hypervolemia |
| Chronic kidney disease | Rhabdomyolysis | Metabolic disturbances (e.g., hyperglycemia) |
| Immunosuppression | Exposure to ACE inhibitors, ARBs, and NSAIDs | Fluid imbalances (e.g., use of hydroxyethyl starch, increased chloride levels) |
Recommendations for the good clinical practice of RRT
| RRT Component | Management |
|---|---|
| Indication | When metabolic byproducts (e.g., hyperkalemia, acidosis, hypervolemia) exceed renal clearance. |
| Modality | Selection of RRT technique depends on the metabolic and hemodynamic priorities of the patient, as well as on the local expertise and resources. |
| Dose | CRRT: effluent rate of 25–30 ml/kg/h. |
| Anticoagulation | Adjusted to coagulation status. |
| Vascular access | Ultrasound guidance reduces costs and complications. |
| Fluid removal | Functional hemodynamic monitoring is essential for optimizing fluid removal rate. |
AKI incidence in patients with COVID-19 disease
| Author and Reference | Location | Period | Definition | Patients no. | Critically ill no. | COVID-AKI no. (%) | COVID-AKI in ICU no. (%) | RRT no. (%) |
|---|---|---|---|---|---|---|---|---|
| Bubenek-Turconi [13] | Romania | 25.03.2020–26.03.2021 | KDIGO | 9058 | 9058 | 2183 (24.1) | 2183 (24.1) | 453 (5) |
| Huang [15] | Wuhan | 16.12.2019–02.01.2020 | KDIGO | 41 | 13 | 3 (7.31) | 3 (23.08) | 3 (7.31) |
| Richardson [16] | New York | 01.03.2020–04.04.2020 | KDIGO | 5700/2351# | 373 | 523 (22.2) | NR | 81 (3.4) |
| Hirsch [17] | New York | 01.03.2020–05.04.2020 | KDIGO + all stages | 5449 | 1395 | 1993 (36.6) | 1060 (76) | 285 (5.2) |
| Gupta [18] | USA | 04.03.2020–04.04.2020 | KDIGO stage 2/3 | 2215 | 2215 | 952 (43) | 952 (43) | 443 (20) |
| Mohamed [19] | Louisiana | 01.03.2020–31.03.2020 | KDIGO | 575 | 173 | 161 (28) | 105 (61) | 89 (15.5) |
| Schaubroeck [20] | Belgium | 01.02.2020–31.01.2021 | KDIGO + all stages | 1286 | 1286 | 1094 (85.1) | 1094 (85.1) | 126 (9.8) |
| Sullivan [21] | United Kingdom | 17.01.2020–5.12.2020 | KDIGO + all stages | 85687 | NR | 13000 (31.5) | NR | 2198 (2.6%) |
| Wang [22] | Wuhan | 01.01.2020–03.02.2020 | KDIGO | 138 | 36 | 5 (3.62) | 3 (8.33) | 2 (1.45) |
| Guan [23] | China | 11.12.2019–29.01.2020 | KDIGO | 1099 | 173 | 12 (1.09) | 6 (3.47) | 9 (0.82) |
| Cao [24] | Wuhan | 03.01.2020–01.02.2020 | KDIGO | 102 | 18 | 20 (19.61) | 8 (44.44) | 6 (5.88) |
| Zhang [25] | Wuhan | 02.01.2020–10.02.2020 | KDIGO | 221 | 55 | 10 (4.52) | 8 (14.55) | 5 (2.26) |
| Xu [26] | China | 01.01.2020–20.02.2020 | NR | 355 | 71 | 56 (15.77) | 21(29.58) | NR |
| Li Z [27] | China | 06.01.2020–21.02.2020 | KDIGO | 193 | 65 | 55 (28.5) | 43(66.15) | 7 (3.63) |
| Zheng [28] | Hangzhou | 22.01.2020–05.03.2020 | KDIGO | 34 | 34 | 7 (20.59) | 7 (20.59) | 5 (14.71) |
| Arentz [29] | Seattle | 20.02.2020–05.03.2020 | KDIGO | 21 | 21 | 4 (19.05) | 4 (19.05) | NR |