
Fig. 1.
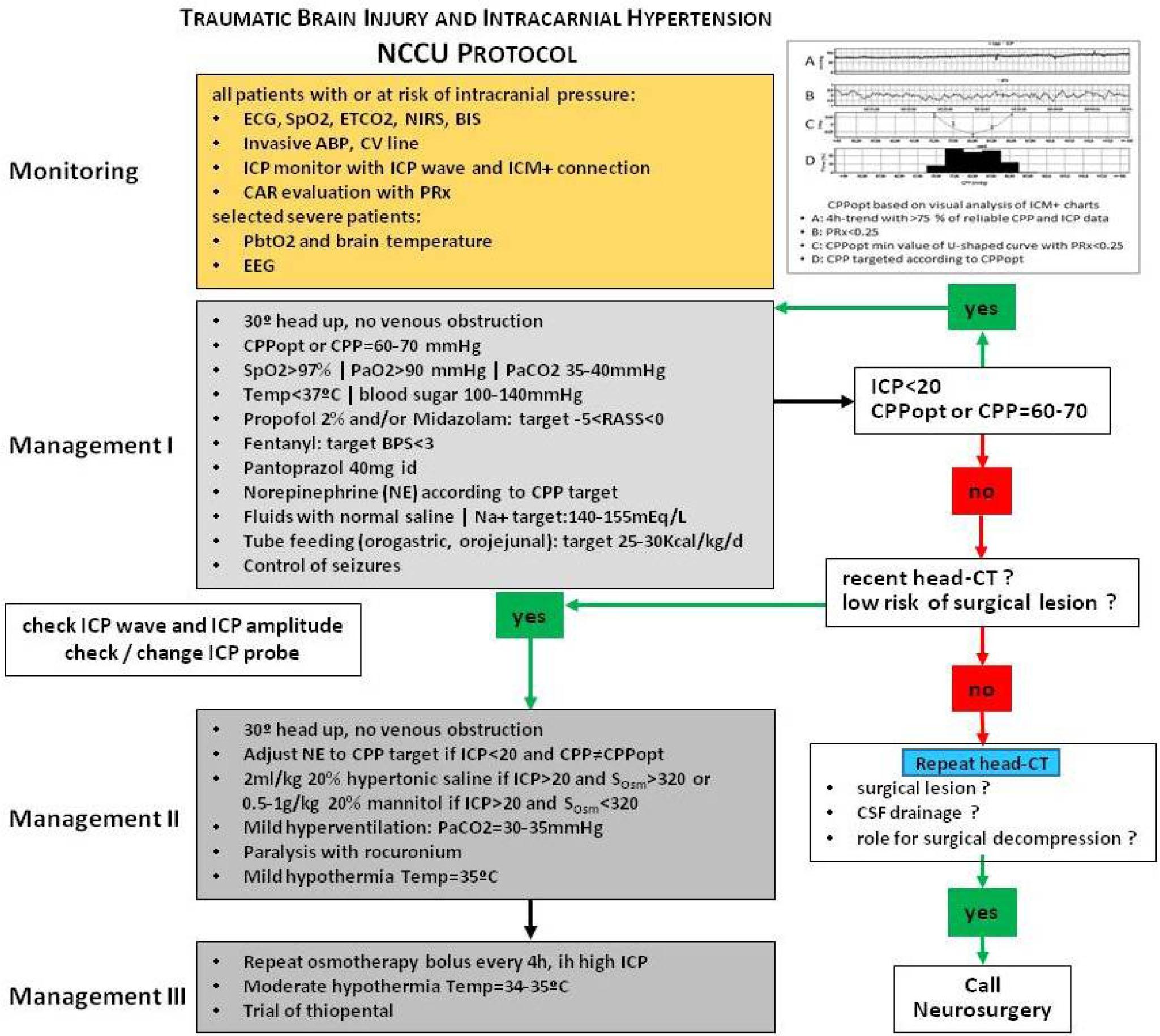
Fig. 2.
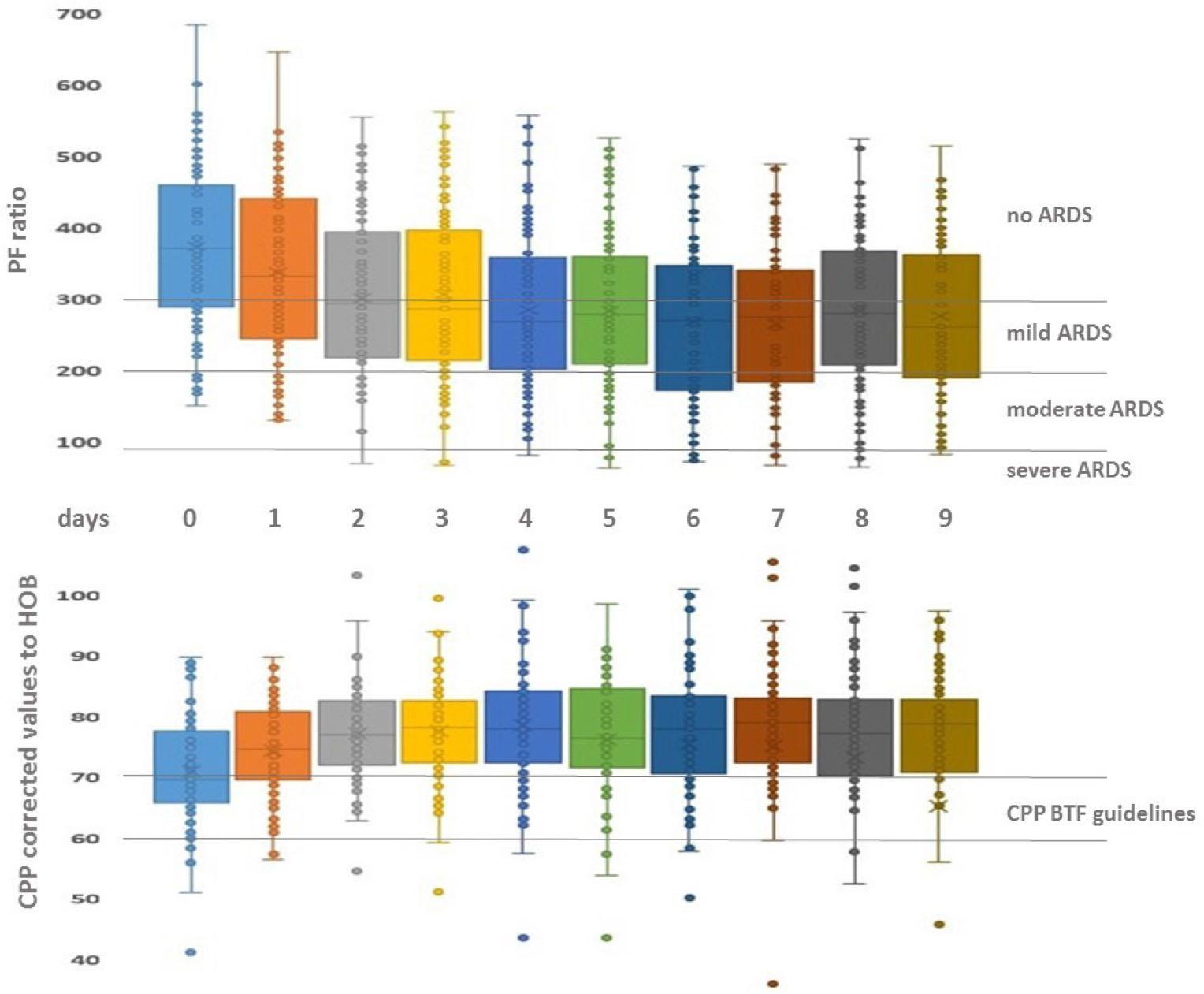
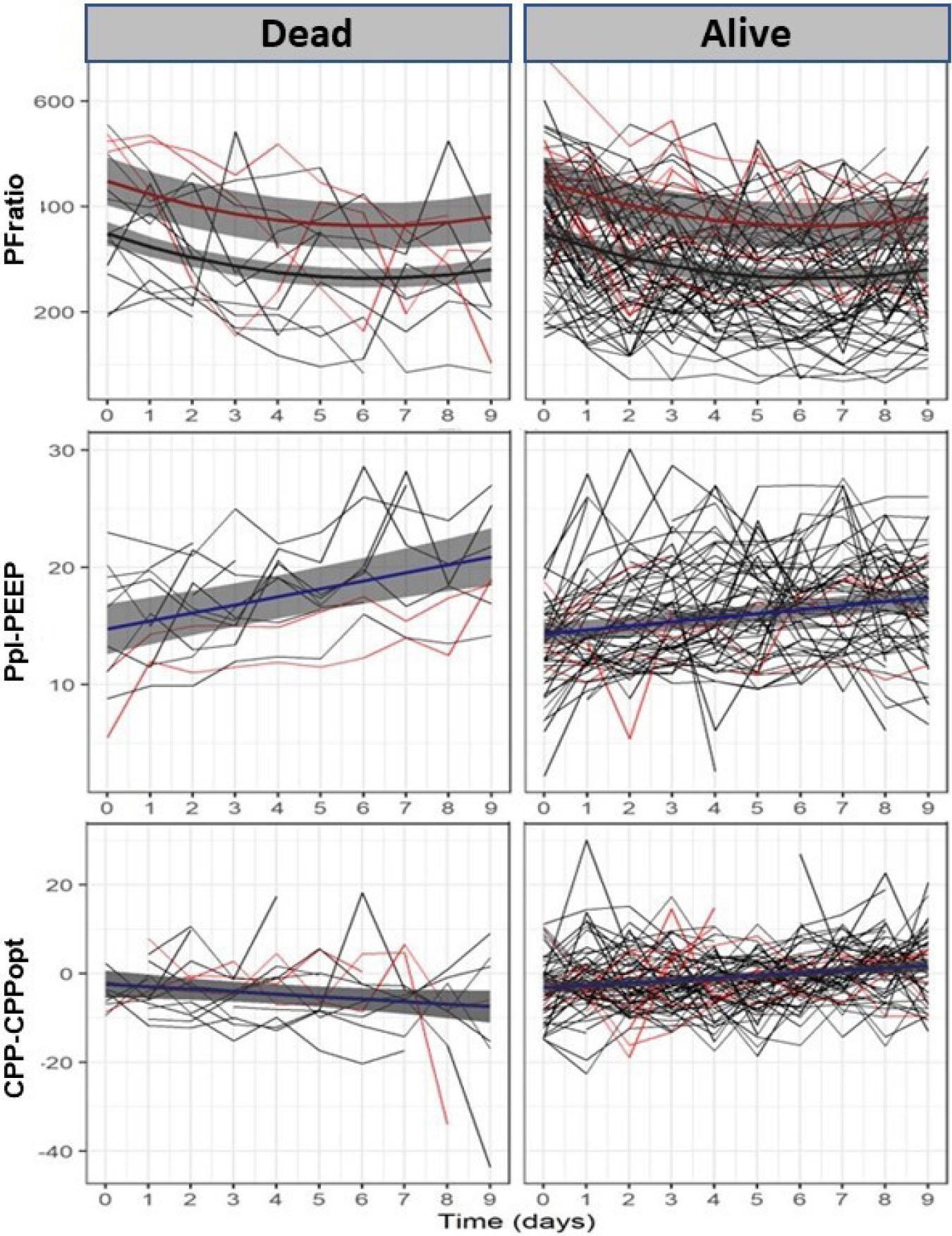
Fig. 3.
Demographic, Monitoring, Management and Outcome data of patients with severe acute Traumatic Brain Injury_
| Variables | Mean±sd /Median (IQR) | |
|---|---|---|
| Demographic Data | ||
| Number of Patients | Total | 92 |
| Multiple Trauma | 45 (49%) | |
| Thoracic Trauma | 19 (21%) | |
| Age (Years) | 53 ± 21 | |
| Gender | Male | 79 (86%) |
| Female | 13 (14%) | |
| GCS at admission | 7 (IQR 5) | |
| APACHE II | 19 ± 6 | |
| Apache II mortality (%) | 33 ± 17 | |
| CT Marshall Classification | 3 (IQR 2) | |
| Monitoring and Management Data | ||
| FiO2 | 0.5 ± 0.13 | |
| PFratio | 305 ± 88 | |
| PaO2(mmHg) | 146.5 ± 28.5 | |
| PaCO2(mmHg) | 38.1 ± 3.7 | |
| SaO2(%) | 98.6 ± 0.74 | |
| RR (cycles/min) | 17 ± 4 | |
| MV (L/min) | 9.45 ± 2.18 | |
| PEEP (cmH20) | 6,2 ± 1,3 | |
| Ppl (cmH20) | 19.7 ± 4.8 | |
| DP=Ppl-PEEP (cmH20) | 15.9 ± 3.5 | |
| Shunt fraction (Qs/Qt) (%) | 16.3±6.7 | |
| Compliance | 43 ± 13.8 | |
| Fluid Balance (ml/d) | 171 ± 564 | |
| Therapy Intensity Level (TIL) | 2 (IQR 1) | |
| HR (bpm) | 71.9 ± 10.5 | |
| ABP (mmHg) | 96.7 ± 7.0 | |
| ICP (mmHg) | 11.2 ± 5.8 | |
| CPP(mmHg) | 85.9 ± 7.4 | |
| PRx | 0.03 ± 0.19 | |
| CPPopt (mmHg) | 88.7 ± 8.5 | |
| CPP-CPPopt (mmHg) | −2.8 ± 10.2 | |
| Outcome Data | ||
| LOS ICU (days) | 22 ± 26 | |
| LOS Hosp (days) | 48 ± 48 | |
| Mortality | 14 (15.2%) | |
| GOS at 3 months | 3 (IQR 2) | |
Estimates from the final mixed-effects regression models for PFratio, CPP-CPPopt and Driving Pressure across time (10 days), adjusted for other variables of interest_
| Variables | FIXED EFFECTS | RANDOM EFFECT | ||
|---|---|---|---|---|
| Coefficient | St Error | p-value | St deviation | |
| Model for the time-effect on PFratio | ||||
| Intercept | 436.42 | 17.63 | <0.001 | 59.25 |
| Time (days) | −27.12 | 4.56 | <0.001 | |
| Days2 | 2.175 | 0.48 | <0.001 | |
| Female | 99.28 | 23.39 | <0.001 | |
| PRx | −49.99 | 15.68 | 0.002 | |
| Ppl-Peep | −5.34 | 0.97 | <0.001 | |
| Model for the time-effect of outcome on CPP-CPPopt | ||||
| Intercept | −2.37 | 1.58 | 0.133 | 2.95 |
| Dead | −0.79 | 1.72 | 0.647 | |
| Time (days) | −0.56 | 0.28 | 0.048 | |
| Time*Dead | 1.10 | 0.31 | <0.001 | |
| Model for the time-effect of outcome on Driving Pressure | ||||
| Intercept | 14.76 | 1.10 | <0.001 | 2.85 |
| Dead | −0.43 | 1.20 | 0.718 | |
| Time (days) | 0.68 | 0.15 | <0.001 | |
| Time*Dead | −0.34 | 0.17 | 0.041 | |