
Fig. 1

Fig. 2
Fig. 3
The mortality rate of acute mediastinitis reported in different studies [6–9]
| Author/s | Year | Number of cases | Mortality rate |
|---|---|---|---|
| Cherveniakov | 1992 | 147 | 14,4% |
| Marty-Ane et al | 1999 | 12 | 16,5% |
| Papalia et al | 2001 | 13 | 23% |
| Macrí P et al | 2003 | 26 | 15,4% |
| Vidarsdottir et al | 2010 | 29 | 31% |
Prognostic score for mortality in case of mediastinitis due to oesophageal perforation
| Points | Sign and symptoms |
|---|---|
| One point for each of the following | Age >75 years Tachycardia Leukocytosis Pleural effusions |
| Two points for each of the following | Fever Noncontained leak on barium esophagram Respiratory compromise Time to diagnosis >24 h |
| Three points for each of the following | Presence of malignancy Hypotension |
Microorganisms involved in the aetiology of acute mediastinitis due to oesophageal perforations [27–28]
| Germs | Gram-positive cocci | Gram-positive bacilli | Gram-negative cocci | Gram-negative bacilli |
|---|---|---|---|---|
| Anaerobic | Peptostreptococcus | Actinomyces Lactobacillus Eubacterium | Veillonella | Bacteroides Prevotella Porphyromonas Fusobacterium |
| Aerobic | Streptococci (including beta-hemolytic and S. viridans group), Staphylococci | Corynebacterium | Moraxella | Enterobacteriaceae Eikenella corrodens Pseudomonas |
| Fungi | Candida albicans | |||
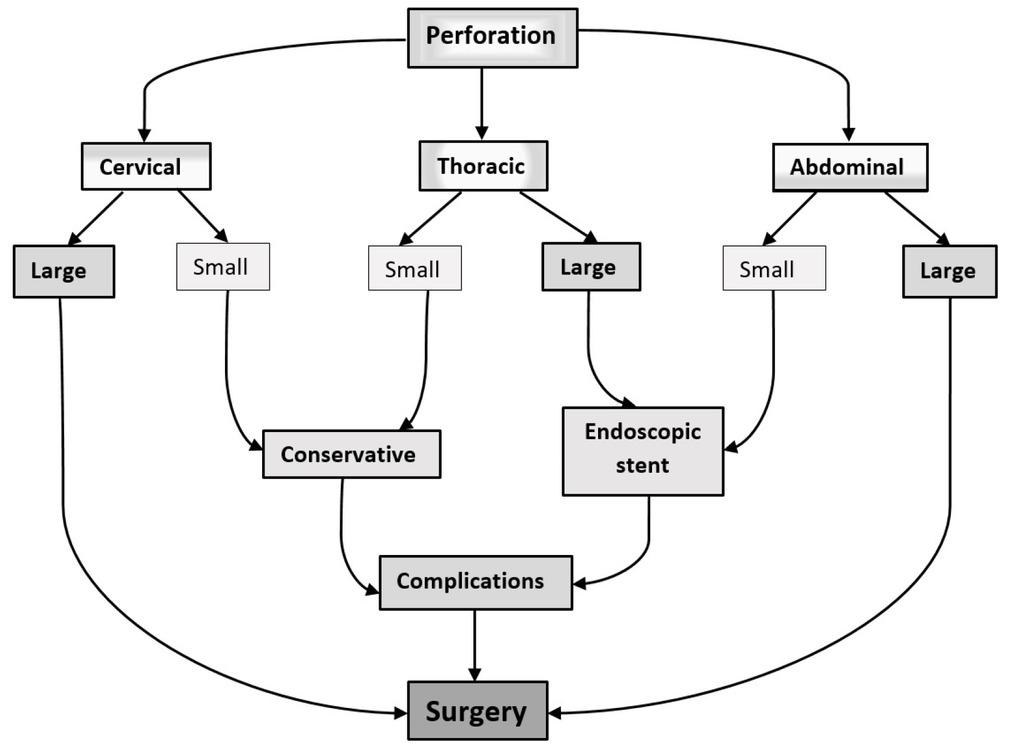
Surgical and endoscopic treatment: indications, class of evidence and recommendations
| Surgical treatment of oesophageal perforations | Recommended | Class of evidence* |
|---|---|---|
| IA | ||
| Perforation <24 h | IC | |
| Primary repair | Perforation <72 h | |
| Thoracic small perforation (failure off medical treatment) | NA** | |
| Abdominal perforations <24 h | IA | |
| Drainage only | Cervical perforations | IIC |
| Thoracic small perforations | NA | |
| Diversion without esophagectomy | Severe mediastinitis after large thoracic perforations in critical patient | IIC |
| Advance stages of oesophageal cancer perforations | IIC | |
| Severe mediastinitis after large thoracic perforations if general conditions | IIC | |
| Esophagectomy | allow | |
| Initially stages of oesophageal cancer | IA | |
| Endoscopic closure system vacuum-(E-VAC) assisted | Large perforations with an efficient peri-oesophageal drainage | IIC |
| Oesophageal stenting associated with pleural/mediastinal drainage | Thoracic perforations<24 h in stable patients Bridging method for critical patients | IIC |