
Relapse is seen in 20–30% of classic Hodgkin lymphoma (cHL) cases, whereas 10% have refractory disease (1). Two randomized trials compared autologous stem cell transplant (ASCT) after high-dose chemotherapy (HDC) with conventional chemotherapy in relapsed/refractory (R/R) cHL. This demonstrated improved outcomes in the transplant arm, making HDC/ASCT the standard of care for R/R cHL (2, 3). Nearly half of the patients eventually relapse after ASCT due to different prognostic factors, such as persistent disease at the time of transplant, bulky disease or B symptoms, extranodal disease, early relapse post-initial treatment, and refractory disease status (4). Nevertheless, the transplant outcome in R/R cHL patients improved after the use of targeted therapy. On programmed cell death- 1 (PD-1) inhibitor, up to one-third of patients exhibit primary resistance, while 30%–40% eventually relapse (5). Brentuximab vedotin (BV), which is commonly used in pre- and post-transplant settings, has improved outcomes, but the European Blood and Marrow Transplantation (EBMT) still considers ASCT the standard of care for relapsed cHL (6). In Pakistan, ASCT began in the mid-90s, but, as in other low- and middle-income countries (LMICs), data scarcity makes it difficult to predict outcomes (7,8,9,10). Our study contributes to the limited national data and highlights the impact of various factors on ASCT for R/R cHL, thereby improving post-ASCT outcomes.
Our single-center retrospective cohort included 33 consecutive patients diagnosed with either relapsed or primary refractory cHL who received HDC/ASCT from January 2013 to December 2023 at Aga Khan University Hospital, Karachi, Pakistan.
Study exclusions included patients younger than 18 years, those with nodular lymphocyte-predominant HL, or those receiving checkpoint inhibitors (CPIs) or BV as primary therapy. Additionally, patients who failed to reach at least partial remission (PR) before HDC, as well as those who had tandem or allogeneic transplants, were ineligible.
We used the electronic medical record system to collect patient demographics, histopathological findings, B symptoms, comorbidities, and Eastern Cooperative Oncology Group (ECOG) performance status. Disease characteristics included bulky disease (nodal mass exceeding one-third of the maximum transverse diameter of the chest or measuring more than 10 centimeters), extranodal or bone marrow involvement, and hematopoietic cell transplantation comorbidity index (HCT-CI). Staging was based on the modified Ann Arbor staging system. Other data collected included salvage therapy, CD34 count, engraftment times for neutrophils and platelets, and transplant-related side effects. Patient staging and response evaluation originally relied on contrast-enhanced computed tomography (CT) scans of the neck, chest, abdomen, and pelvis. In 2015, our institution adopted positron emission tomography/computed tomography (PET/CT) as the standard.
We excluded patients with insufficient data from this retrospective analysis. The Ethical Review Committee of AKUH (AKU-ERC #: 2024-10616-31480) granted approval, including a waiver of informed consent. The data used in the analysis were anonymized. Overall and progression-free survival were our primary endpoints, and all subjects were censored at the last follow-up date, regardless of outcome.
The cHL diagnosis was based on routine histopathological examination of a biopsy of nodal or extranodal tissue classified according to the 2008 and 2016 Revised WHO Classification of Hematopoietic and Lymphoid Tumors (11, 12). A new biopsy was performed in relapsed or refractory patients, especially when new disease sites were identified. Patients’ staging was according to the modified Ann Arbor staging system, and they were stratified into risk categories according to the National Comprehensive Cancer Network (NCCN) guidelines (13). Clinical response was evaluated using the Lugano 2014 classification: Complete Response (CR) was defined as a Deauville score of 1–3, PR as a score of 4, and Stable (SD) or Progressive Disease (PD) as a score of 5 (14). Relapsed cHL was defined as either clinical or radiological evidence of disease after achieving complete remission and was proven by biopsy. Early relapse was defined as clinical or radiological recurrence between 3 and 12 months post-initial therapy, with late relapse occurring thereafter. Refractory cHL was characterized by disease progression within 3 months, failure to achieve a complete or partial response to first-line treatment, or a Deauville score of 4–5 per Lugano criteria (15, 16). Those who achieved CR or PR after the last salvage chemo regimen were considered chemosensitive, whereas all others were categorized as having chemoresistant disease. Progression-free survival (PFS) was determined from the date of transplant until disease progression or relapse, or death irrespective of cause, or last physician visit, whichever happened earlier. Overall survival (OS) was determined from the date of transplant until death from any cause, the last clinic visit, or censoring, whichever occurred first. Transplant-related mortality (TRM) was considered mortality within 100 days of transplant due to causes other than cHL. For survival analysis, 31st December 2023 was the cut-off.
Initial assessments of all patients and counseling involving their relatives regarding the potential risks and benefits of undergoing ASCT were done in the outpatient clinic. All the transplant candidates were evaluated for transplant fitness, and disease assessment was mandatory before ASCT to ensure remission.
The pre-transplant workup included a complete blood count and liver and kidney function tests. Prothrombin and activated partial thromboplastin time were checked. Viral serology included cytomegalovirus status, hepatitis B surface antigen, hepatitis C, varicella-zoster, and human immunodeficiency virus antibodies. Also, blood group determination, chest radiography, echocardiography, Mantoux test, and pulmonary function tests, followed by dental and psychiatric evaluation. Every single patient gave informed consent in writing for receiving blood products, chemotherapy, central venous access via Hickman’s catheter, and transplantation. Patients were kept in a single room equipped with a high-efficiency particulate air (HEPA) filter and were placed on a neutropenic diet. Over time, we observed a shift in stem cell mobilization practices. Initially, the patients received 1500 mg/m2 cyclophosphamide followed by 5 mg/ kg granulocyte colony-stimulating factor (G-CSF) subcutaneously two times a day for 6 days, and stem cells were harvested on days 5 to 7 via either a COMTEC (Fresenius Kabi, Bad Homberg, Germany) system or a Cobe Spectra AutoPBSC. With the passage of time, it was switched to G-CSF-based mobilization only, and later on, G-CSF 5 mg/kg twice daily with 0.24 mg/kg plerixafor subcutaneously on day 4, with the goal of achieving a cell dose of more than or equal to 2 × 106 CD34+ stem cells per kilogram of the patient’s weight.
Standard antimicrobial prophylaxis was used according to institutional policy. The transplant day was considered as 0, on which stem cells were infused via central line after premedication with pheniramine maleate (45.5 mg). From day +1, we initiated G-CSF (5 mg/kg) and were transfused with irradiated blood products as needed. A leukocyte filter was used with packed red cells. Our transplant protocol has been described previously, along with febrile neutropenia evaluations and treatment protocol (7). The BEAM (carmustine 300 mg/m2 on day -6, etoposide 200 mg/m2, and cytarabine 200 mg/m2 from day -5 to -2 while melphalan 140 mg/ m2 on day -1) protocol was used until 2014; since then, institutional preference has shifted towards Be-EAM (only replacing day -6 carmustine with bendamustine 150 mg/m2 from day -5 to -4, with the remaining drugs and doses being the same). Post-transplant response assessment was done in the outpatient setting after 4 weeks, then on day 100; subsequent visits were once a month for 3 months, then every 3 months for a year, and then every 6 months thereafter, either in person or via teleclinic. Therapeutic response was evaluated using either CT scans or PET/CT, depending on institutional availability. We defined toxicities as per the National Cancer Institute’s Common Terminology Criteria for Adverse Events Version 3.0 (2003).
Neutrophil engraftment was defined as an absolute neutrophil count (ANC) ≥ 0.5 × 109/L for three consecutive days post-transplant. Platelet engraftment was defined as achieving a count ≥ 20 × 109/L for seven days without transfusion support.
All patient characteristics were analyzed via descriptive statistics. Continuous variables were expressed as medians with ranges, while categorical variables were reported as frequencies or proportions. The Kaplan-Meier method and survival curves were used to estimate OS and PFS, and the log-rank test was used to assess differences in survival. OS was considered the interval from the transplant to death or last follow-up, whichever happened first. PFS was considered the interval between transplant and either PD, death, or the last follow-up, whichever occurred first. Those patients who survived without progression were censored at the last date they were known alive. Prognostic factors were identified via regression analyses, and hazard ratios (HRs) were estimated with 95% confidence intervals using a Cox regression model. We deemed the result significant if the p-value was below 0.05. Statistical calculations were performed on SPSS v.26 (IBM, USA) and R version 4.5.2 for Windows.
Patient characteristics are summarized in Table 1. The median age at diagnosis was 24 years (range, 18–53 years), with a male-to-female ratio of 1.75:1. Nodular sclerosis was the most common histologic subtype. According to Lugano staging, no patients presented with stage I disease, while the majority (n = 25, 75.8%) had advanced-stage disease.
Except for one patient who received liposomal doxorubicin due to documented cardiac disease, all patients were treated with frontline ABVD (adriamycin, bleomycin, vinblastine, and dacarbazine). The median number of salvage regimens was 1 (range, 1–4). Concomitant radiotherapy was administered to five patients (15.2%) during salvage treatment.
The median duration to first relapse was 12 months (range, 2–84 months), while 16 patients (48.5%) experienced an early relapse. All patients had chemosensitive disease (either CR or PR).
Transplant-related characteristics are detailed in Table 2. The median interval from diagnosis to transplantation was 19 months (range, 0–87 months), while 22 patients (66.7%) received HDC/ASCT within 24 months of diagnosis. Stem cell mobilization was achieved using G-CSF alone or in combination with cyclophosphamide or plerixafor, and all patients underwent peripheral stem cell harvesting. While two patients yielded a CD34+ stem cell dose below 2 × 106/kg, successful neutrophil and platelet engraftment was achieved within 2 and 3 weeks, respectively, and both patients remained alive.
Details are summarized in Table 2. Engraftment was successful in 31 patients (93.9%), with sepsis identified as the primary cause of engraftment failure. Twenty-six patients experienced febrile illness; microbiologically documented infections were confirmed in only 13 (39.4%). Escherichia coli was the most common bloodstream infection (BSI) isolate (n = 4). The median duration of intravenous antibiotic therapy for febrile neutropenia was 7 days (range, 3–18 days). Eight patients (24.2%) required amphotericin therapy, including one patient with an elevated beta-D-glucan level and another with Candida isolated from a mid-stream urine culture.
The median follow-up duration for the cohort was 42 months (range, 28–56 months), while the median OS and PFS were 65 and 31 months, respectively. As shown in Figure 1, the estimated 2- and 5-year OS were 77.9% (95% CI: 64.6–93.8%) and 65.4% (95% CI: 48.1–88.8%), respectively, while the corresponding PFS estimates were 62.1% (95% CI: 45.8–84.1%) and 45.8% (95% CI: 28.9–72.7%). As illustrated in Figures 2A and 2B, the 2-year OS was significantly higher in patients in CR (82.2%) than in those in PR (66.7%; p=0.031). Age, histological subtype, disease stage at relapse, and primary refractory vs relapsed disease were evaluated via log-rank analysis but did not reach statistical significance. Among the 10 patients treated with BV, 2 patients relapsed, reflecting an overall response rate of approximately 80%.
Table 3 presents the univariate Cox proportional hazards regression analyses for PFS and OS. Inferior OS was observed in patients experiencing early relapse prior to transplantation (HR 4.02; 95% CI: 1.00–16.08; p=0.049) and those failing to achieve pre-transplant CR (HR 3.69; 95% CI: 1.03–13.23; p=0.045). Failing to achieve CR post-transplant demonstrated borderline statistical significance (HR 3.87; 95% CI: 0.99–15.11; p=0.051). Although BEAM conditioning was statistically significant, its hazard ratio was less than 1 (HR 0.14; 95% CI: 0.04–0.53; p=0.004), likely skewed by its predominant use in 87.9% of patients. Inferior PFS was only seen with failure to achieve CR post-ASCT (HR 5.06; 95% CI: 1.95–13.15; p < 0.001).
Multivariate analysis was deferred due to an insufficient number of events per variable, as it would yield unreliable multivariable estimates and potential model instability. Similarly, the TRM in our study was 6.1% (2 deaths) within 100 days of ASCT. Due less than 1 (HR 0.14; 95% CI: 0.04–0.53; p=0.004), likely skewed by its predominant use in 87.9% of patients. Inferior PFS was only seen with failure to achieve CR post-ASCT (HR 5.06; 95% CI: 1.95–13.15; p < 0.001).
Patient characteristics.
| Characteristic | Number (range) | Percentage |
|---|---|---|
| Male | 21 | 63.6% |
| Female | 12 | 36.4% |
| B-symptoms | ||
| Diagnosis | 26 | 78.8% |
| Relapse | 13 | 39.4% |
| Bulky disease at relapse | 3 | 9.1% |
| Histological subtype | ||
| Nodular Sclerosis | 16 | 48.5% |
| Mixed Cellularity | 6 | 18.2% |
| Lymphocyte Rich | 2 | 6.1% |
| Unspecified cHL | 9 | 27.2% |
| Ann Arbor stage (at diagnosis) | ||
| II | 8 | 24.3% |
| III | 14 | 42.4% |
| IV | 11 | 33.3% |
| Ann Arbor stage (at relapse) | ||
| I | 6 | 18.2% |
| II | 8 | 24.2% |
| III | 12 | 36.4% |
| IV | 7 | 21.2% |
| Extranodal Disease | ||
| Diagnosis | 5 | 15.2% |
| Relapse | 14 | 42.4% |
| Bone marrow involvement (at diagnosis) | 7 | 21.2% |
| Duration of CR1 | ||
| < 12 months | 16 | 48.5% |
| ≥ 12 months | 17 | 51.5% |
| First salvage therapy | ||
| DHAP | 12 | 36.4% |
| ICE | 6 | 18.2% |
| IGEV | 5 | 15.1% |
| GDP | 2 | 6.1% |
| Brentuximab-Bendamustine | 7 | 21.2% |
| ESHAP | 1 | 3.0% |
| Brentuximab | ||
| Pre-transplant | 10 | 30.3% |
| Post-transplant | 4 | 12.1% |
| Pre-transplant disease status | ||
| CR | 24 | 72.7% |
| PR | 9 | 27.3% |
| Relapsed disease | 19 | 57.6% |
| Primary refractory disease | 14 | 42.4% |
Abbreviation key: CR: complete remission; cHL: classic Hodgkin lymphoma; DHAP: dexamethasone, high dose cytarabine and cisplatin; ESHAP etoposide, methylprednisolone, high-dose cytarabine, and cisplatin; GDP Gemcitabine, Dexamethasone, Cisplatin; ICE ifosfamide, carboplatin and etoposide; IGEV ifosfamide, vinorelbine, gemcitabine and prednisone; PR partial remission.
Transplant related characteristics
| Characteristic | Number | Percentage/range |
|---|---|---|
| ECOG | ||
| 0 | 33 | 100% |
| HCT-CI | ||
| 0 | 32 | 97% |
| 1 | 1 | 3.0% |
| Stem cell mobilization | ||
| G-CSF | 14 | 42.4% |
| Cyclophosphamide with G-CSF | 12 | 36.4% |
| G-CSF with plerixafor | 7 | 21.2% |
| Mean CD34 Count (106/kg) | 6.77 | 1 – 17.3 × 106/kg |
| Conditioning Regimen | ||
| Be-EAM | 29 | 87.9% |
| BEAM | 4 | 12.1% |
| Median Neutrophil engraftment (days) | 12 | 10–43 days |
| Median Platelet engraftment (days) | 16 | 11–45 days |
| Toxicities | ||
| Mucositis | ||
| Grade I | 14 | 42.4% |
| Grade II | 11 | 33.3% |
| Grade III | 4 | 12.1% |
| Grade IV | 2 | 6.1% |
| Diarrhea | 25 | 75.8% |
| Gastrointestinal bleeding | 3 | 9.1% |
| Post-transplant relapse | ||
| In less than Three months | 2 | 6.1% |
| Three to Twelve months | 6 | 18.2% |
| More than Twelve months | 6 | 18.2% |
| Post-transplant CR | 20 | 60.6% |
| Cause of death | ||
| Sepsis | 4 | 12.1% |
| Disease progression | 3 | 9.1% |
| COVID-19 | 1 | 3.0% |
| Primary graft failure | 2 | 6.1% |
Abbreviation key: Be-EAM: (Bendamustine, Etoposide, Cytarabine, Melphalan); BEAM: (Carmustine, Etoposide, Cytarabine, Melphalan); COVID-19: coronavirus disease of 2019; CR: complete remission; G-CSF: (Granulocyte Colony-Stimulating Factor); CD: Cluster of Differentiation; ECOG: Eastern Clinical Oncology Group; HCT-CI: hematopoietic cell transplantation specific comorbidity index.
Multivariate analysis was deferred due to an insufficient number of events per variable, as it would yield unreliable multivariable estimates and potential model instability. Similarly, the TRM in our study was 6.1% (2 deaths) within 100 days of ASCT. Due to the very low number of events, regression analysis was not performed. There was no reported second malignancy.
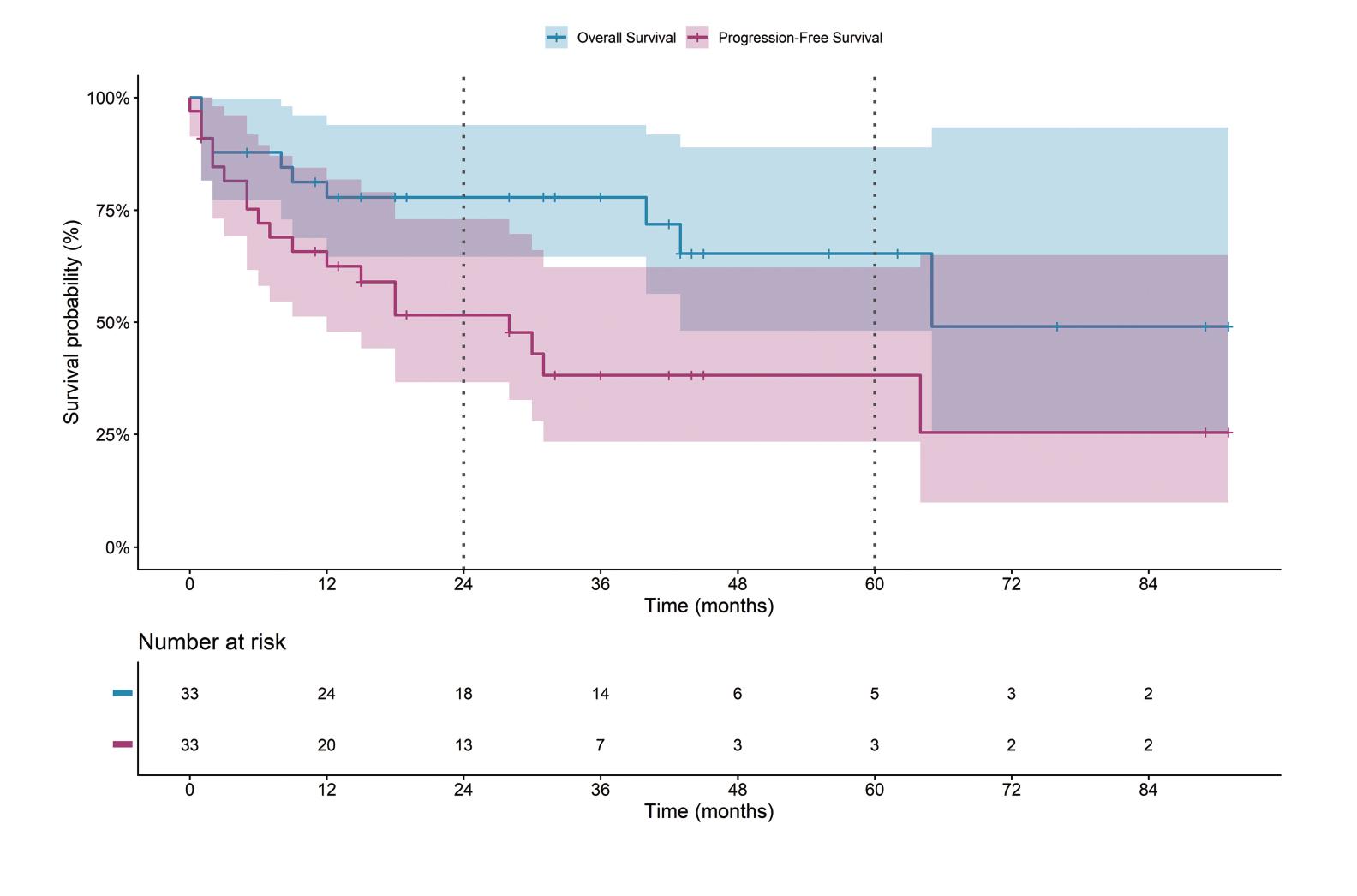
2 and 5 years of overall and progression free survival in R/R cHL who underwent HDC/ASCT.
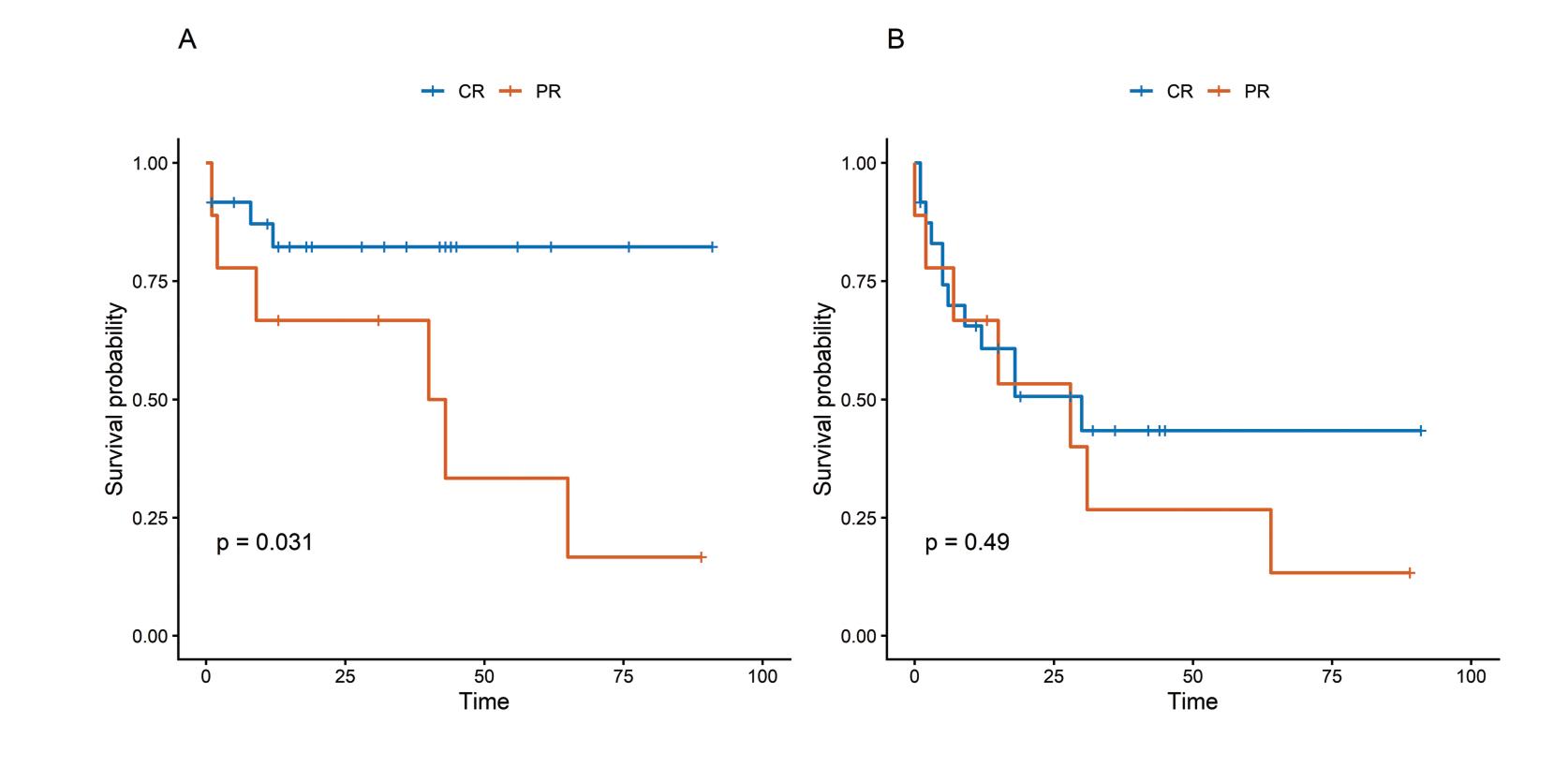
Kaplan-Meier estimates of survival according to pre-transplant disease status. (A) Overall survival and (B) progression-free survival stratified by complete response (CR) and partial response (PR) prior to HDC/ASCT.
Despite the small sample size, this study emphasizes the prognostic importance of pre-transplant status in R/R cHL. With a median follow-up of 42 months, our data show that early relapse and failure to achieve CR before transplant significantly worsen overall survival. Patients who achieved CR before ASCT had superior 2-year OS compared with those in PR.
In our cohort, nodular sclerosis (48.5%) did not significantly affect prognosis, contrasting with the findings of Akhtar et al. (17), who identified it as a poor prognostic factor. The predominance of advanced-stage disease at diagnosis (75.8%) is similar to other Pakistani studies, such as Hidayat et al. (9) and Iftikhar et al. (18), which reported 59% and81.1% of patients with advanced-stage disease at diagnosis, respectively. A recent study from India reported that 70.4% were advanced-stage HL patients on diagnosis (10). This highlights the diagnostic delay in LMICs, one of the contributory factors of poor outcomes (19, 20). Different salvage regimens have been developed, including the incorporation of novel agents to improve outcomes. But there is no standard conditioning regimen (21). Consistent with Bröckelmann et al. (22), DHAP was the most utilized salvage regimen in our cohort (36.4%). Although their study identified primary refractory status and stage IV disease at relapse as predictors of poor outcomes, our results showed no significant survival difference between relapsed and primary refractory cHL. This finding aligns with Nieto et al. (23), who reported comparable EFS rates for primary refractory and relapsed patients (47% vs. 45%, respectively). Moskowitz et al. (24) reported no difference in EFS or OS for relapsed versus primary refractory disease.
Univariate analysis for overall survival and progression-free survival
| Variable | Overall Survival | Progression-Free Survival | ||
|---|---|---|---|---|
| HR (95% CI) | p-value | HR (95% CI) | p-value | |
| Extranodal on relapse | 0.50 (0.13–1.94) | 0.318 | 1.50 (0.61–3.70) | 0.382 |
| Be-EAM conditioning | 0.14 (0.04–0.53) | 0.004 | 0.39 (0.13–1.20) | 0.102 |
| More than 24 months from diagnosis to transplant | 0.27 (0.05–1.36) | 0.112 | 0.51 (0.18–1.44) | 0.204 |
| Bulky disease | 0.35 (0.03–3.62) | 0.378 | 0.63 (0.13–3.01) | 0.560 |
| Nodular sclerosis | 0.85 (0.24–2.99) | 0.795 | 1.08 (0.44–2.66) | 0.873 |
| Age more than or equal 30 years | 0.92 (0.23–3.61) | 0.905 | 1.10 (0.42–2.91) | 0.840 |
| Pre-transplant >1 salvage | 1.73 (0.44–6.78) | 0.432 | 0.57 (0.17–1.96) | 0.371 |
| Primary refractory | 2.08 (0.59–7.33) | 0.257 | 1.41 (0.56–3.53) | 0.461 |
| Advanced stage on relapse | 2.61 (0.65–10.44) | 0.174 | 1.87 (0.73–4.79) | 0.192 |
| Pre-transplant less than CR | 3.69 (1.03–13.23) | 0.045 | 1.38 (0.53–3.55) | 0.510 |
| Post-transplant less than CR | 3.87 (0.99–15.11) | 0.051 | 5.06 (1.95–13.15) | <0.001 |
| Pre-transplant relapse in less than 12 months | 4.02 (1.00–16.08) | 0.049 | 1.13 (0.45–2.81) | 0.792 |
Significant p-value in bold.
Abbreviation key: CR complete remission; Be-EAM: (Bendamustine, Etoposide, Cytarabine, Melphalan); HR: Hazard ratio.
Early pre-transplant relapse (under 12 months) emerged as a significant predictor of poor OS (HR 4.02; 95% CI 1.00–16.08; p=0.04), reinforcing the prognostic importance of relapse timing as reported by Sureda et al. (25). The cohort consisted entirely of chemosensitive patients, with 72.7% reaching CR before undergoing ASCT. These data corroborate the existing literature, demonstrating that responsiveness to salvage therapy is a critical prognostic marker for superior OS (26–28). Roerden et al. (29) reported superior five-year PFS in patients who attained pre-ASCT CR (64.8% versus 39.3%, p=0.10). Husi et al. (30) highlighted an important difference in PFS based on BV therapy but, more importantly, reported improved 5-year OS and PFS in those with pre-ASCT CR. Senapati et al. (1) reported significantly better OS in those who achieved CR prior to ASCT (p=0.006). These findings align with our univariate analysis, which showed that pre-ASCT CR is significantly associated with better OS (p=0.045). This was also supported by Moskowitz et al., who reported that the 5-year EFS was better in PET-negative than PET-positive patients (75% vs 31%) prior to ASCT (31).
The predominance of Be-EAM (87.9%) reflects carmustine shortages and global shifts toward bendamustine-based regimens, with recent meta-analyses confirming comparable efficacy (32). Visani et al. (26) reported mucositis and gastroenteritis as the most common side effects of the BEAM regimen, with TRM at day 100 of 0%. Krawiec et al. (33) compared BEAM with Be-EAM and reported a greater risk of mucositis in Be-EAM patients. Similarly, the predominant conditioning toxicities in our cohort were mucositis (93.9%) and diarrhea (75.8%). The TRM in our study (6.1%) is similar to those reported in several recent studies (1, 9, 10, 18, 34).
With a median follow-up of 42 months, our estimated 5-year OS (65.4%) was better than 45.3% reported by Kumar et al. (10). However, BV usage, 30.3% pre-transplant and 40% for consolidation, remained lower than in developed regions, likely due to high drug costs limiting affordability in our setting. Post-transplant CR was borderline significant on univariate analysis for OS (HR 3.87; 95% CI 0.99–15.11; p=0.051) but was a significant factor for PFS (HR 5.06; 95% CI 1.95–13.15; p=0.001). These findings were consistent with those of other studies (10, 21). Sepsis caused four deaths (12.1%), primarily due to E. coli, consistent with our center’s previous data. Notably, TRM for cHL has improved over time from 12% to 6.1% (7).
Hodgkin Reed-Sternberg (HRS) cells express PD-L1, which suppresses T-cell antitumor responses and triggers retrograde signaling to sustain growth. The presence of tumor-associated macrophages is considered an adverse prognostic factor in patients receiving ABVD regimens (35,36,37). PET/CT detects tumor metabolic activity via FDG uptake, making it essential for diagnosis and response assessment. Treatment rapidly halts metabolism in HRS cells, resulting in PET negativity. Consequently, achieving CR or PR indicates chemosensitivity, which is a predictor of favorable outcomes following ASCT in R/R cHL (38).
Pre-transplant disease status is a valuable determinant of outcomes in R/R cHL. Prioritizing CR through response-adapted salvage is essential, particularly for high-risk subgroups like those with early relapse (<12 months). In LMICs, where access to novel agents is limited, maximizing pre-transplant chemosensitivity is vital.
This study has several limitations, notably its retrospective design, which introduces inherent limitations such as missing data, selection bias, and the inability to control for confounders. Another limitation was a small sample size and reduced number of events, which reduced statistical power and precluded multivariate analysis due to potential model instability. A significant selection bias arises from institutional policies that prioritize chemosensitive patients to ensure the most efficient use of limited resources in an LMIC setting. Additionally, the transition to PET/CT as the institutional standard in 2015 introduced variability, as patients treated before then were assessed with CT scans.
Our data align with international standards, highlighting that achieving pre-transplant CR improves survival. Bridging outcome disparities will require strengthening early diagnosis to avoid advanced-stage presentations and improving access to novel agents. Furthermore, given the challenges of PD-1 inhibitor resistance, future research should prioritize incorporating diverse novel agents into salvage regimens to optimize patient outcomes.