
Malignant ovarian germ cell tumors are rare tumors that originate from primordial germ cells in the embryonal gonad and exhibit two distinct histological patterns: dysgerminoma and non-dysgerminomas, including embryonal carcinoma, choriocarcinoma, immature teratoma, endodermal sinus tumor, and mixed germ cell tumors (1). Many of these tumors are diagnosed at an early stage, and treatment with cisplatin-based regimens has led to better outcomes for the disease (2). For dysgerminomas, the estimated 5-year survival rate was almost 100%, and for non-dysgerminomatous malignant ovarian germ cell tumors, it was approximately 85% (3).
Our hospital is a tertiary care center and gets referrals from across the country. Due to poor socio-economic status, there is a delay in presentation, leading to increased tumor burden, surgical resection by inexperienced surgeons, and treatment toxicity, which leads to inferior outcomes as compared to advanced countries. An analysis of single-center data from Egypt and Argentina highlighted differences in disease presentation, treatment, and survival, which were attributed to variations in healthcare settings and availability (4, 5). In similar studies conducted in North India, it has been demonstrated that overall care management has a practical impact on patient outcomes (6).
The current study aims to bridge this gap by focusing on malignant ovarian germ cell tumors treated at a tertiary care hospital in Pakistan and analyzing the outcomes of patients treated with chemotherapy and surgery in a multidisciplinary setting, including survival rates, treatment complications, and recurrences over the last two decades.
This retrospective study was conducted at the Shaukat Khanum Memorial Cancer Hospital, Lahore, Pakistan, and included data collection on patient characteristics, provided treatment, and outcomes of female pediatric patients ≤18 years old diagnosed with malignant ovarian germ cell tumors from January 1999 to December 2022. The study was conducted after approval from the Institutional Review Board of Shaukat Khanum Memorial Cancer Hospital, Lahore, Pakistan (exemption number: EX-04-12-23-01). Information was obtained from the hospital’s electronic medical records, including patient socio-demographic data, tumor diagnosis, and treatment information. The patient population consisted of all individuals with histologically proven malignant ovarian germ cell tumors who had completed their treatment at our facility. Patients with incomplete information, those who lost follow-up, or who commenced treatment at another center, were excluded from the study. The diagnosis was established by morphology and immunohistochemistry. Staging was performed using computed tomography (CT) and magnetic resonance imaging (MRI), and a histopathology report was obtained (Table 1). Risk stratification was performed using the United Kingdom Children’s Cancer Study Group Germ Cell Working Group protocol 2005 for the treatment of extracranial germ cell tumors in children and adolescents (7) (Table 1).
Stage and Risk Stratification.
| Stage | Features |
|---|---|
| I | Limited to the ovary (peritoneal evaluation should be negative). There is no evidence of disease beyond the ovaries. (Note: The presence of gliomatosis peritonei does not result in changing Stage I disease to a higher stage.) |
| II | Microscopic residual; peritoneal evaluation negative. (Note: The gliomatosis peritonei does not change Stage II disease to a higher stage. Tumor markers normalize or decrease with an appropriate half-life. |
| III | Lymph node involvement (metastatic nodule); gross residual or biopsy only; contiguous visceral involvement (omentum, intestine, bladder); peritoneal evaluation positive for malignancy. |
| IV | Distant metastases, including the liver. |
| Risk | Features |
|---|---|
| Low | Gonadal Stage 1 tumors (regardless of AFP (Alpha fetoprotein) level if secreting). |
| Intermediate | Pure germinoma, Stage 2, 3, or 4, Pure HCG (Human chorionic gonadotrophin) secreting tumors, Stage 2 or 3 |
| High Risk | All Stage 4 tumors > 10,000 k U/L |
Those given JEB were classified per UKCCSG, and those given PEB per the Children’s Oncology Group (COG) protocol (8). Regimen selection was not based on any age criteria; rather, it was more of the physician’s discretion. From 1999–2022, there was no change in chemotherapy protocol or risk stratification, and UK-based JEB and COG-based PEB were used. Events for EFS were Death, Relapse, and progression.
Toxicity workup done at staging and during treatment, including hearing assessment and Renogram. Pulmonary function tests were done to assess bleomycin toxicity where possible. No specific tools were used for toxicity assessment; it was based on the results of investigations.
For patients who underwent upfront surgery, the treatment protocol was tailored to the risk group. Patients with stage I disease with complete resection and normalized tumor markers were categorized as the low-risk group and did not receive chemotherapy. Postoperatively, AFP (alpha-fetoprotein) is monitored weekly until it returns to normal levels, and then every 4 weeks. If there were only rising serum markers and no radiological disease, the disease would be treated as intermediate risk. If serum markers rose and radiological disease was apparent, the treatment was administered according to the relapse group.
Patients with intermediate risk received a total of 4 courses of JEB (Carboplatin, Etoposide, Bleomycin), at a 21-day interval. If AFP has not returned to normal after four courses, it was monitored weekly as levels normalized. Second-look surgery was considered when a residual mass persisted after four courses and serum markers were normal. Additionally, patients in the high-risk group received a total of 6 courses of JEB (Carboplatin, Etoposide, Bleomycin) at 21-day intervals.
Second-line chemotherapy for relapses or progression includes VeIP (Vinblastine, ifosfamide, cisplatin), TIP (Paclitaxel, ifosfamide, cisplatin), and Gemcitabine/Oxaliplatin.
Third-line chemotherapy included IPO (irinotecan, paclitaxel, and Oxaliplatin) if the patient could not respond to second-line chemotherapy. At the end of treatment, computed tomography (CT) scans were performed, and patients were followed up with AFP (Alpha feto protein) for secretory tumors and abdominopelvic ultrasound, along with chest x-ray for non-secretory tumors when no residual disease was found. If there was residual disease at the end of treatment, patients were discussed in a multidisciplinary meeting, and a decision was taken to undergo second-look surgery. Regular follow-up was done as an outpatient for disease relapse and to look for any significant long-term effects. As per our institution’s policy, all oncology patients diagnosed were kept on follow-up for 5 years from the end of treatment, after which they were discharged with instructions.
IBM SPSS (version 26.0) was used for data analysis. The key outcome factors examined were 5-year overall survival (OS), event-free survival (EFS), recurrence rates, and treatment-related complications. Patient demographics, disease status, and treatment characteristics were described using descriptive statistics, and survival outcomes were analyzed using Kaplan-Meier tests. A p-value of < 0.05 was considered statistically significant.
The study included 116 patients diagnosed with Malignant ovarian germ cell tumors, with a median age at diagnosis of 13.5 years. All patients were at least 10 years of age (81.0%), and the majority were between 11 and 17 years old. A follow-up was conducted at a median of 40 months (range, 5 to 72 months) after the initial diagnosis.
Thirteen patients had stage I (11.2%), 10 had stage II (8.6%), 56 had stage III (48.3%), and 37 had stage IV disease. (31.9%) The majority of histological subtypes identified were dysgerminoma (38.7%), followed by yolk sac tumor (29.3%), mixed germ cell tumor (27.6%), and embryonal carcinoma (4.3%). Patients classified into low-risk group 16(13.8%), intermediate 43(37.1%), high risk 57(49.1%). Initially, 102 (87.9%) patients underwent upfront surgical resection of the tumor, and delayed surgery or salvage surgery (post-chemotherapy) was done in 22 (12.1%). All patients received adjuvant chemotherapy after the initial workup and diagnosis, except for 7 (6.03%). Of the 109 patients who received chemotherapy after the initial diagnosis, 75 (68.8%) received JEB (Carboplatin, etoposide, bleomycin), 29 (26.6%) received BEP (bleomycin, etoposide, cisplatin), and 5 (4.6%) received PEB (cisplatin, Etoposide, Bleomycin), with a median of four chemotherapy cycles administered (range: 1–6). (Table 2) provides a summary of the patient’s demographics and other clinical features.
Patient’s demographic and clinical characteristics.
| Characteristics | n = 116 |
|---|---|
| Median follow up | 40 (5–72 months) |
| Median age at diagnosis | 13.5 years (10–17) |
| ≤11 years | 20 (17.24%) |
| >11 years | 94 (81.0%) |
| Histology | |
| Dysgerminoma | 45 (38.7%) |
| Embryonal carcinoma | 5 (4.3%) |
| Yolk Sac Tumour | 34 (29.3%) |
| Mixed Germ Cell Tumour | 32 (27.6%) |
| Stage | |
| I | 13 (11.2%) |
| II | 10 (8.6%) |
| III | 56 (48.3%) |
| IV | 37 (31.9%) |
| AFP (Alpha feto protein) | |
| <10 | 43 (37.1%) |
| 10–100 | 10 (8.6%) |
| 100–1000 | 14 (12.1%) |
| >1000 | 49 (42.2%) |
| Surgery | |
| Upfront surgery only | 102 (87.9%), |
| Delayed surgery + salvage surgery | 22 (12.1%) |
| Risk group | |
| Low | 16 (13.8%) |
| Intermediate | 43 (37.1%) |
| High | 57 (49.1%) |
| First-line chemotherapy | |
| JEB (Carboplatin, etoposide, bleomycin) | 75 (64.7%) |
| BEP (bleomycin, etoposide, cisplatin) | 29 (25.0%) |
| PEB (cisplatin, Etoposide, Bleomycin) | 5 (4.3%) |
| No chemotherapy | 7 (6.03%) |
Following the initial chemotherapy treatment, 22 patients (18.96%) had second-look surgery due to the presence of residual viable tumors at the end of treatment imaging. All were resectable, and 4 patients progressed. Among these, 13 patients showed no viable tumor, while there was one case of each of dysgerminoma, germ cell tumor, embryonal carcinoma, and ovarian fibroma. Mature teratoma was diagnosed in 4 patients. Chemotherapy was well tolerated in all patients, and very few neutropenic complications were observed while on treatment. The five-year event-free survival (EFS) rate for all patients was 87.1%, and the overall survival (OS) rate was 90.5% (Figure 1). The relapse rate was 2.6%, progression was 7.8%, and Deaths were 11 (10.4%). Disease progression was the main cause of death in 7 patients. Acute kidney injury due to tumor lysis was seen in 2 patients, while sepsis with neurotoxicity was seen in 1 patient with tumor progression leading to death. One patient diagnosed with secondary acute myeloid leukemia (AML) 36 months after treatment died before treatment could be started. (Table 3)
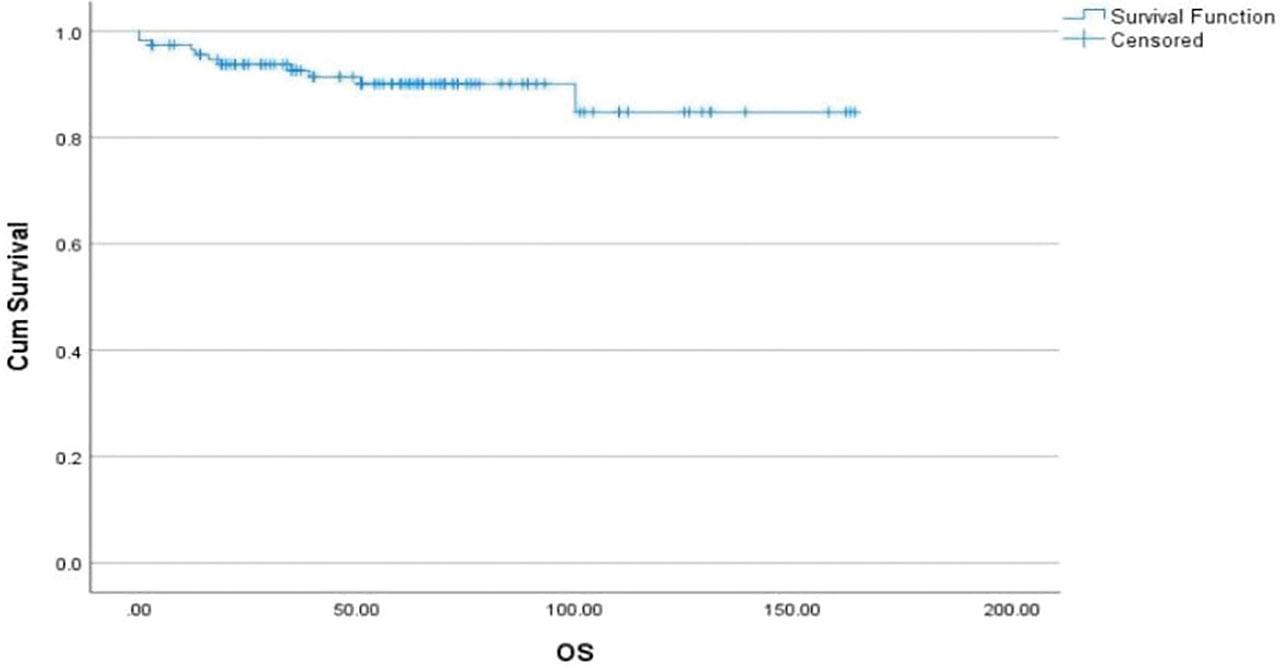
The five-year overall survival (OS) rate was 90.5%.
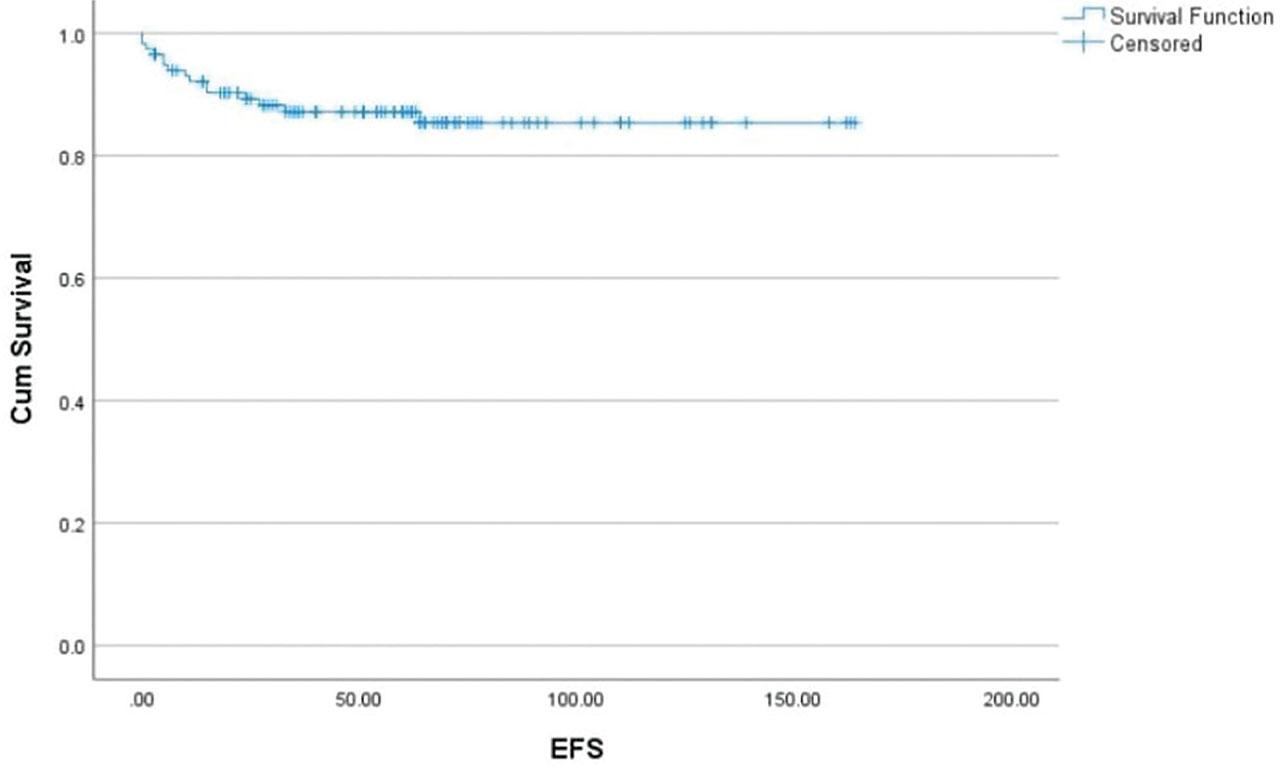
The five-year event-free survival (EFS) rate for all patients was 87.1%,
Characteristics of patients with deaths (n=11).
| Number | Age at Diagnosis (Years) | Histology | Stage | Surgery | Adjuvant Chemotherapy | Time from Diagnosis to progression, relapse (months) | Treatment after Progression or Recurrence | Status |
|---|---|---|---|---|---|---|---|---|
| 1 | 15 | YST | 3(HR) | Laparotomy | BEP (6 cycles) | 5months (progression) | Gemcitabine/oxaliplatin (6 cycles) | Died (due to progression) |
| 2 | 11 | YST | 3(HR) | Mets in liver | JEB (6 cycles) | 7 months (progression) | VeIP (6 cycle) | Died (due to progression) |
| 3 | 13 | Mixed GCT | 4(HR) | Nil | JEB (6 cycles) | 5 months (progression) | VeIP (6 cycles) | Died (due to progression) |
| Gemcitabine/oxaliplatin (6 cycles) | ||||||||
| 4 | 11 | Mixed GCT | 4(HR) | Laparotomy | BEP (4 cycles) | 36 months (relapse) | TIP (4 cycles) | Died (due to progression) |
| 5 | 12 | Dysgerminoma | 4(HR) | Nil | BEP (2 cycles) | 5 months (progression) | VeIP (2 cycle) | Died (due to progression) |
| 6 | 11 | YST | 4(HR) | Nil | JEB (6 cycles) | 14 months (progression) | VeIP (3 cycles) | Died (due to progression) |
| Gemcitabine/vinorelbine (1 cycle) | ||||||||
| 7 | 16 | Mixed GCT | 4(HR) | Nil | JEB (3 cycles) | 1 months (progression) | BEP (1 cycle) | Died (due to toxicity) |
| 8 | 17 | YST | 3(HR) | Irresectable | BEP (6 cycles) | 24 months (progression) | VeIP(1 cycle) | Died (due to toxicity) |
| VIP(1cycle) | ||||||||
| 9 | 11 | YST | 4(HR) | Nil | JEB (1 cycles) | 5 months (progression) | Nil | Died (due to toxicity) |
| 10 | 15 | Mixed GCT | 4(HR) | Nil | JEB (1 cycles) | 14 months (progression) | Nil | Died (due to toxicity) |
| 11 | 11 | Dysgerminoma | 4(HR) | Nil | JEB (6 cycles) | 36 months (Secondary AML) | Nil | Died (due to secondary AML) |
BEP (bleomycin, etoposide, cisplatin) TIP, (Taxol + ifosfamide + cisplatin); YST, yolk sac tumor; JEB, Carboplatin+ etoposide bleomycin; VeIP(Vinblastine, ifosfamide, cisplatin); HR (High risk) AML, Acute myeloid leukemia. AKI, Acute Kidney Injury. TLS, tumor lysis syndrome.
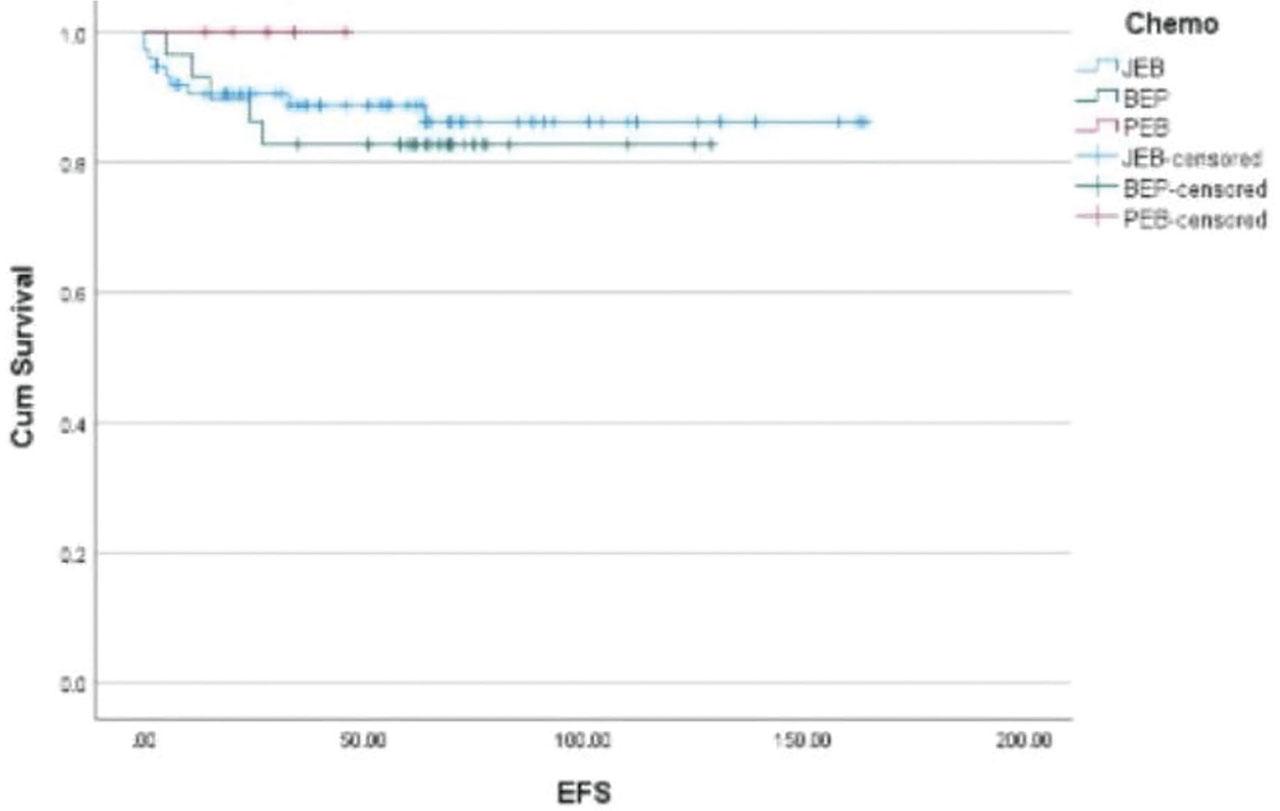
In terms of chemotherapy, the event-free survival (EFS) for JEB (Carboplatin, Etoposide, Bleomycin), BEP (bleomycin, etoposide, cisplatin), and PEB (cisplatin, Etoposide, Bleomycin) were 88.0%, 82.8%, and 100.0%, respectively (Figure 2).
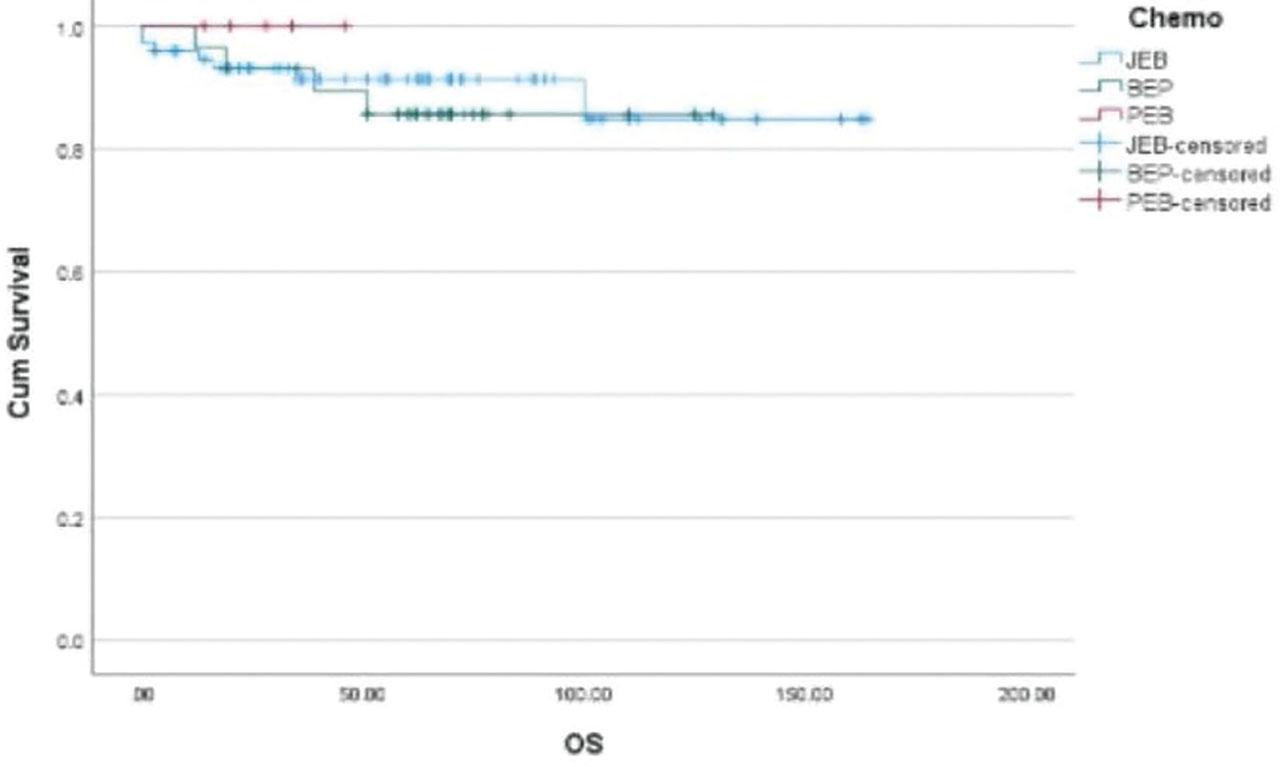
In terms of chemotherapy, the overall survival (OS) for JEB (Carboplatin, Etoposide, Bleomycin), BEP (bleomycin, etoposide, cisplatin), and PEB (cisplatin, Etoposide, Bleomycin) were 90.7%, 86.2%, and 100.0%, respectively.
In terms of chemotherapy, the event-free survival (EFS) for JEB (Carboplatin, Etoposide, Bleomycin), BEP (bleomycin, etoposide, cisplatin), and PEB (cisplatin, Etoposide, Bleomycin) were 88.0%, 82.8%, and 100.0%, respectively.
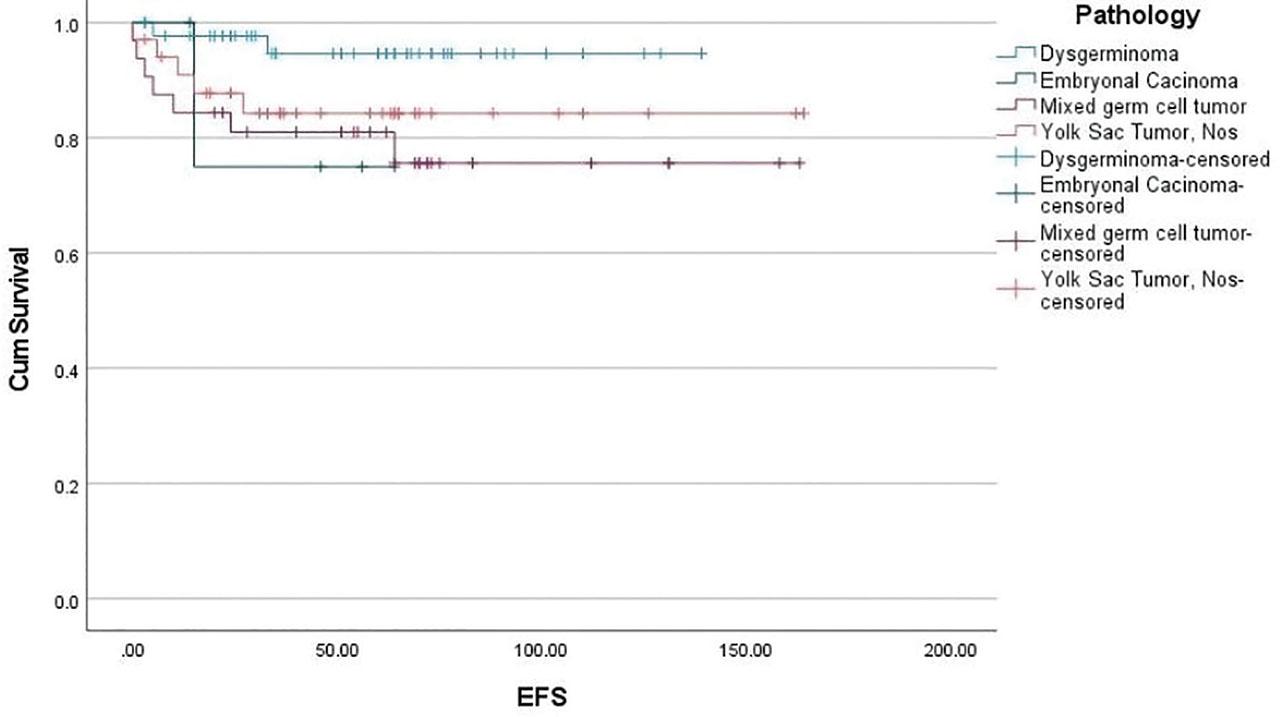
According to risk group, the EFS for low-, intermediate-, and high-risk groups were 93.8%, 97.7%, and 77.2%, respectively (Figure 3). Based on histological subtypes, the estimated five-year event-free survival (EFS) was 95.1% for dysgerminoma, 78.1% for mixed germ cell tumor, and 85.3% for yolk sac tumor (YST), as shown in Figure 4.
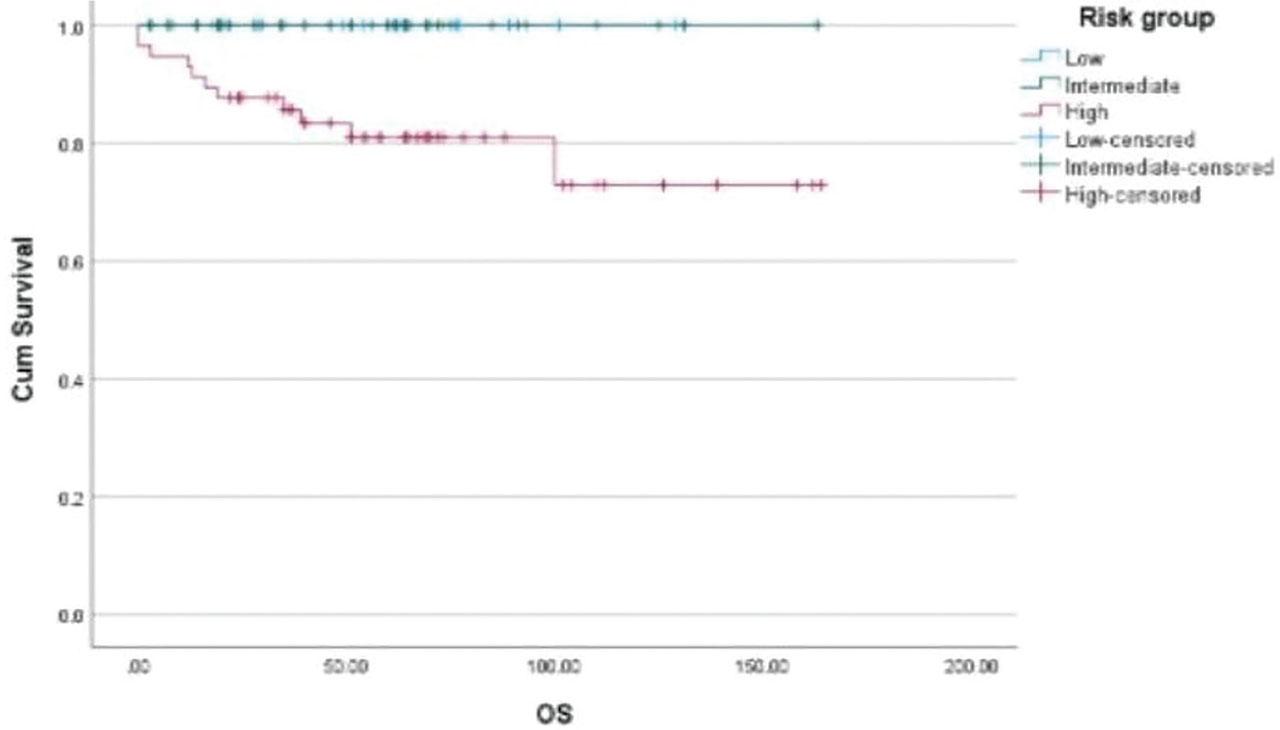
According to the risk group, the OS for low, intermediate, and high risk were 100%, 100%, and 80.7%, respectively.
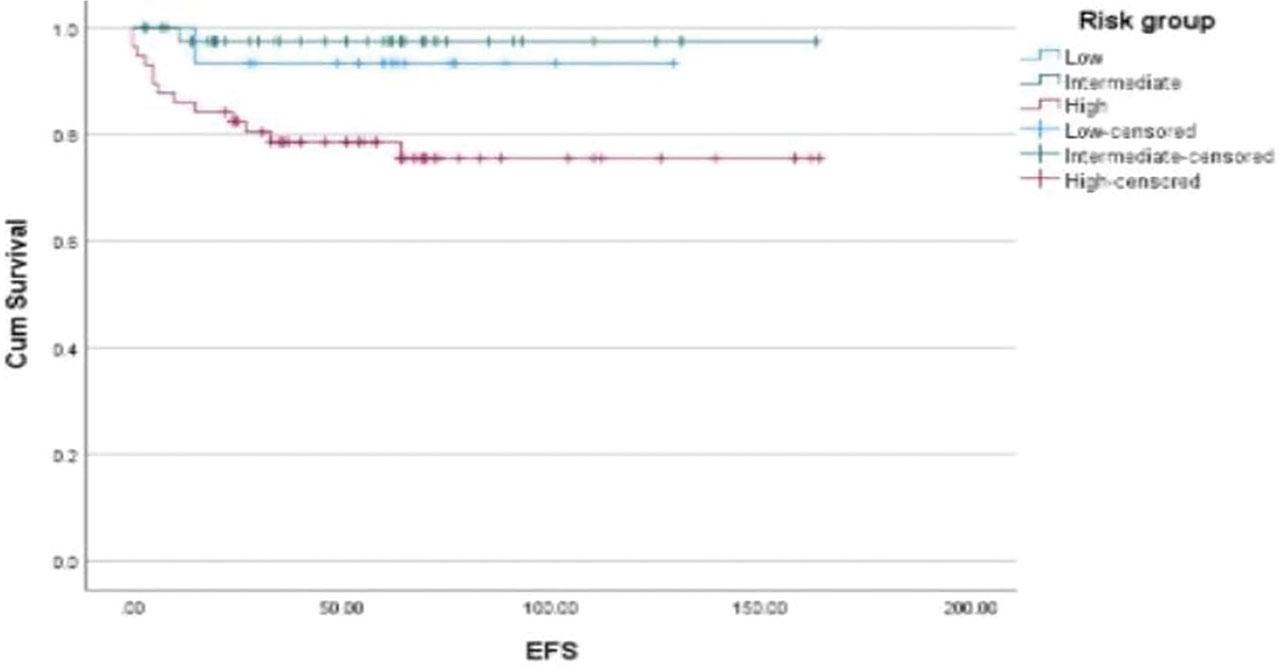
According to the risk group, the EFS for low, intermediate, and high risk were 93.8%, 97.7%, and 77.2%, respectively.
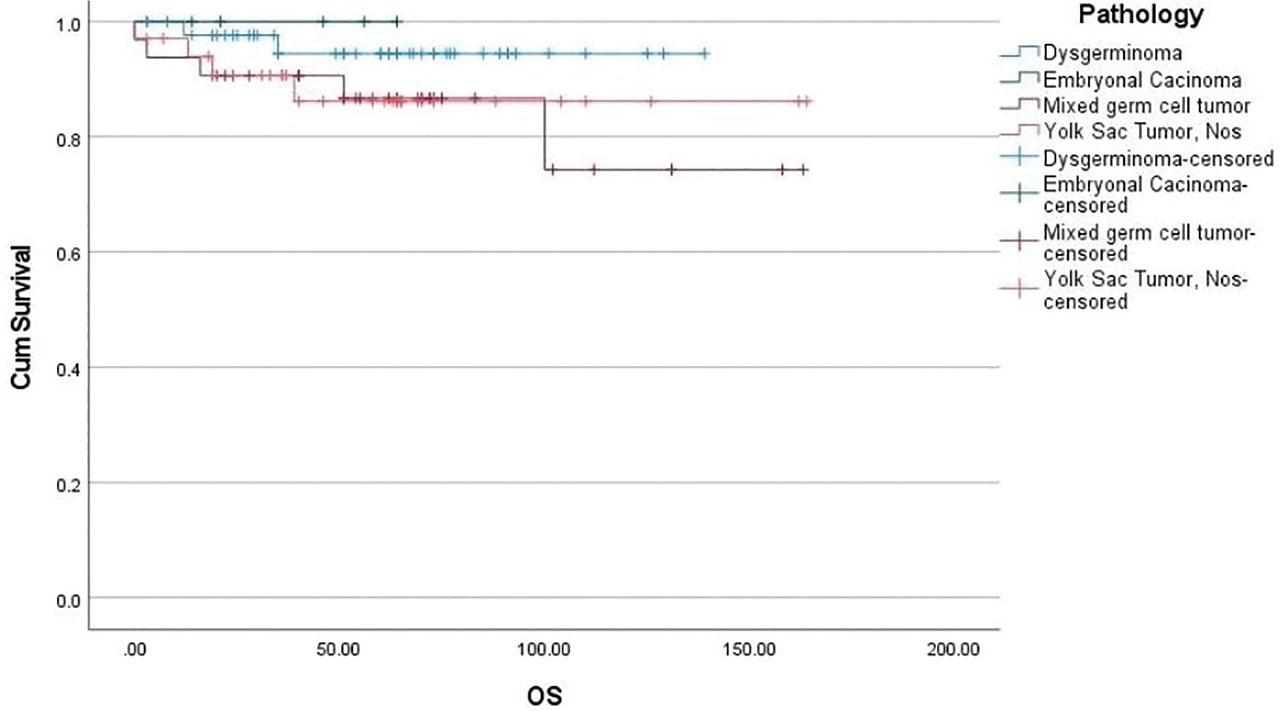
Based on histological subtypes, the estimated five-year OS was 95.1% for dysgerminoma, 84.4% for mixed germ cell tumor, and 88.2% for yolk sac tumor.
Based on histological subtypes, the estimated five-year event free survival (EFS) was 95.1% for dysgerminoma, 78.1% for mixed germ cell tumor, and 85.3% for yolk sac tumor.
Malignant ovarian germ cell tumors (MOGCTs) are a rare and diverse group of ovarian tumors, characterized by their varied presentations, histological features, and outcomes (9). This single-institutional cohort provides data on the management and outcomes of pediatric malignant ovarian germ cell tumors (MOGCTs) from a low-resource setting over two decades. Our results demonstrate that excellent survival outcomes are achievable through standardized multimodal therapy, even in LMICs. Further strengthening findings from high-income countries where survival rates exceed 85–90% for most subtypes of MOGCTs (9).
Our results show a five-year event-free survival (EFS) rate of 87.1% and an overall survival (OS) rate of 90.5%, which is comparable to outcomes reported in developed countries, where multimodal strategies have significantly improved prognosis (7, 11). These findings are significant given resource constraints and the common occurrence of late-stage presentations in LMICs (12).
There is a predominance of dysgerminoma in our cohort, and its excellent prognosis is consistent with recent reports showing that this histology remains the most chemosensitive and surgically curable subtype of MOGCTs (13). Inferior outcomes in yolk sac tumors (YSTs) and mixed germ cell tumors seen in our study are in line with evidence emphasizing their aggressive behavior and higher relapse rates despite platinum-based chemotherapy (14, 15). Additionally, risk stratification remains crucial for MOGCTs; patients classified as high-risk have inferior survival outcomes (16).
Tumor marker dynamics in MOGCTs are important, particularly the early normalization of alpha-fetoprotein (AFP) and beta-human chorionic gonadotropin (β-hCG), which were strongly predictive of favorable outcomes (17). Moreover, recent literature supports the integration of serial tumor marker monitoring in treatment response assessment and relapse prediction, and patients with delayed normalization of tumor markers are highly associated with increased risk of treatment failure (18).
Event-free survival with carboplatin vs cisplatin was compared; carboplatin was used in 75 patients (64.7%) with an Event-free survival of 88%, and cisplatin in 34 patients (29.3%) with an Event-free survival of 91.4%. The Overall survival with carboplatin vs cisplatin was 90.7% and 93.1%, respectively. JEB chemotherapy (carboplatin, etoposide, and bleomycin) demonstrated good outcomes in this cohort, with minimal toxicity, and can be administered as outpatient chemotherapy. More recently, cisplatin-based chemotherapy regimens are being used for children over 11 years, and this is given as an inpatient with optimal results; however, with a higher toxicity rate.
In LMIC settings where delayed admissions occur due to bed shortages, our results show that children aged 11 years or older with specific histology and advanced staging can be successfully treated with JEB chemotherapy. Additionally, a growing consensus favors carboplatin-based regimens in pediatric patients to minimize long-term toxicities, such as nephrotoxicity and ototoxicity (19). These findings are significant in LMIC, where intensive supportive care for cisplatin-related toxicities is limited.
In this cohort, mortality occurred predominantly in high-risk patients presenting advanced-stage disease or poor performance status, highlighting the persistent challenges of late presentation and suboptimal initial control. Salvage chemotherapy regimens such as VeIP and TIP were offered; however, standard treatments were not very effective in treating recurrent diseases, consistent with recent studies advocating for the exploration of targeted and immunotherapy options in refractory cases (20,21). Additionally, two patients died due to treatment complications, including tumor lysis syndrome (TLS) and acute kidney injury (AKI) after progressive disease and relapse, highlighting the importance of meticulous supportive care, mainly in resource-limited settings (22).
We observed one case of secondary acute myeloid leukemia following prolonged etoposide exposure and established a late complication of platinum and etoposide-based chemotherapy. This highlights the importance of long-term follow-up and survivorship care in pediatric oncology populations (23).
Fertility preservation counseling sessions were made with the adolescent patients along with parents, and their questions were addressed appropriately; however, we don’t offer fertility preservation, and follow-up was made for long-term toxicity for 5 years as per Institutional policy. Moreover, these issues remain crucial in the management of MOGCT survivors. Importantly, Carboplatin- and cisplatin-based regimens carry risks of gonadal dysfunction, while etoposide and platinum compounds also pose risks of secondary malignancies, as reflected by one patient developing secondary AML.
The strengths of our study include a large sample size, standardized treatment protocols, and extended follow-up. However, the retrospective nature introduces limitations, including missing data, selection bias, and limited information on fertility preservation and psychosocial outcomes. Furthermore, the absence of molecular profiling and genetic data limits the ability to gain deeper biological insights that may guide future personalized therapies. Finally, long-term follow-up data on late effects and quality of life were not systematically collected, limiting the assessment of critical survivorship issues in this young patient population.
Our study shows good outcomes for girls with ovarian tumors. Early tumor marker response and histological subtype are important prognostic factors. While outcomes in low-resource settings can match global standards with structured protocols, high-risk patients and those with relapsed disease remain a significant concern. Future directions should include incorporating molecular diagnostics, exploring novel agents for relapsed disease, and focusing on survivorship issues, such as late effects and fertility preservation.