
The World Health Organization’s current definition of pediatric palliative care (PPC) focuses on improving the quality of life (QOL) of children by actively addressing their physical, psychological, social, and spiritual needs, from the time of diagnosis through the course of illness. It also involves providing support to the family [1]. PPC is essential and ensures that children and their families receive compassionate, holistic care even when a cure is not possible.
Evidence from both high-income and low- and middle-income countries (LMICs) highlights significant, overlapping barriers to the provision of PPC. A systematic review of LMICs revealed critical gaps, including limited integration of PPC into national health systems, inadequate specialized training for healthcare providers, and restricted access to essential pain medications such as opioids. These deficits contribute to poor QOL, accessibility, and availability of PC services, with pain management and emotional support particularly lacking compared to high-income settings [2]. Moreover, communication barriers with patients and families represent a major hurdle in LMICs, where a scarcity of professional counselors often leaves doctors and nurses inadequately prepared and overburdened to provide effective counseling and psychosocial support [3]. Emotional and psychological challenges affect care globally; studies from high-income countries report caregiver distress, feelings of failure, reluctance to discuss death, and prognostic uncertainty as significant impediments to optimal PPC delivery [4].
Despite increasing recognition of the need for PPC globally, significant knowledge gaps remain regarding how contextual, cultural, and interpersonal factors shape the delivery and experience of care, particularly in LMICs. Existing studies have largely focused on quantifying service availability, workforce shortages, and policy limitations, but there are no studies that have focused on the problems faced by children, their families, and health care providers in this part of the world, where terrorism, security, and financial instability dominate over the limitations identified in other studies. A qualitative approach is therefore appropriate to capture the nuanced perspectives and experiences of patients and caregivers involved in PPC, enabling a deeper understanding of the barriers and facilitators that influence care delivery within real-world clinical and sociocultural contexts.
A retrospective qualitative content analysis was conducted by reviewing patient records extracted from the hospital information system (HIS) from January 1, 2019, to August 27, 2024. The study included 150 patients (≤18 years old, both genders) referred to the palliative medicine team in the outpatient and inpatient departments of a tertiary cancer hospital. The dataset was large and heterogeneous, enabling the capture of recurring patterns, and reached thematic saturation at 150 case reviews, after which no new concepts emerged. Ethical approval was obtained from the Institutional Review Board (EX-26-11-24-01).
The decision to use existing clinical notes rather than primary data collection was based on ethical and practical considerations. Engaging terminally ill children and their families in direct interviews posed significant ethical sensitivities and emotional burdens, as was noted in a study, where some family caregivers declined participation because grief-related distress made face-to-face interviews overwhelming [5]. Comprehensive team-based reviews by the palliative team, followed by multidisciplinary team meetings documented in clinical notes, provided valuable insights into real-world practice and challenges faced in routine care. This retrospective approach enabled the inclusion of a wide range of cases over several years, allowing the identification of recurring themes relevant to PPC delivery.
Data were extracted from narrative notes recorded by healthcare professionals in the HIS, and reflexive thematic analysis (RTA) was performed. RTA was conducted using Braun and Clarke’s six-phase, inductive, data-driven approach: (1) data familiarization, (2) code generation, (3) theme searching, (4) theme review, (5) theme definition, naming, and (6) report production. This approach aligns with a documentary thematic analysis perspective, applying reflexive interpretation to existing textual data to uncover how clinical meanings and practices are represented in the records. Operational definitions for key variables are provided in Supplementary File 1.
Data were manually coded line-by-line using NVivo 15 to support systematic, reflexive analysis. Codes were grouped into categories, from which key themes and sub-themes emerged, reflecting an iterative engagement with the data.
Since his study was based on a retrospective chart review, patient or caregiver quotes were unavailable. Thematic insights were derived from clinical notes, and the preliminary findings were independently reviewed by a palliative care co-researcher to enhance rigor and reduce bias. An audit trail documented coding and theme development, supporting dependability and confirmability, while detailed contextual descriptions aided transferability. Credibility was further ensured through prolonged engagement and secure data storage.
The research team had prior experience in PC and was involved in pediatric care during the study, alongside a pediatric oncology team. Reflexivity was maintained to account for potential interpretive influence.
Thematic analysis identified the following five themes as challenges in PC provision to terminally ill children. (See Figure 1)
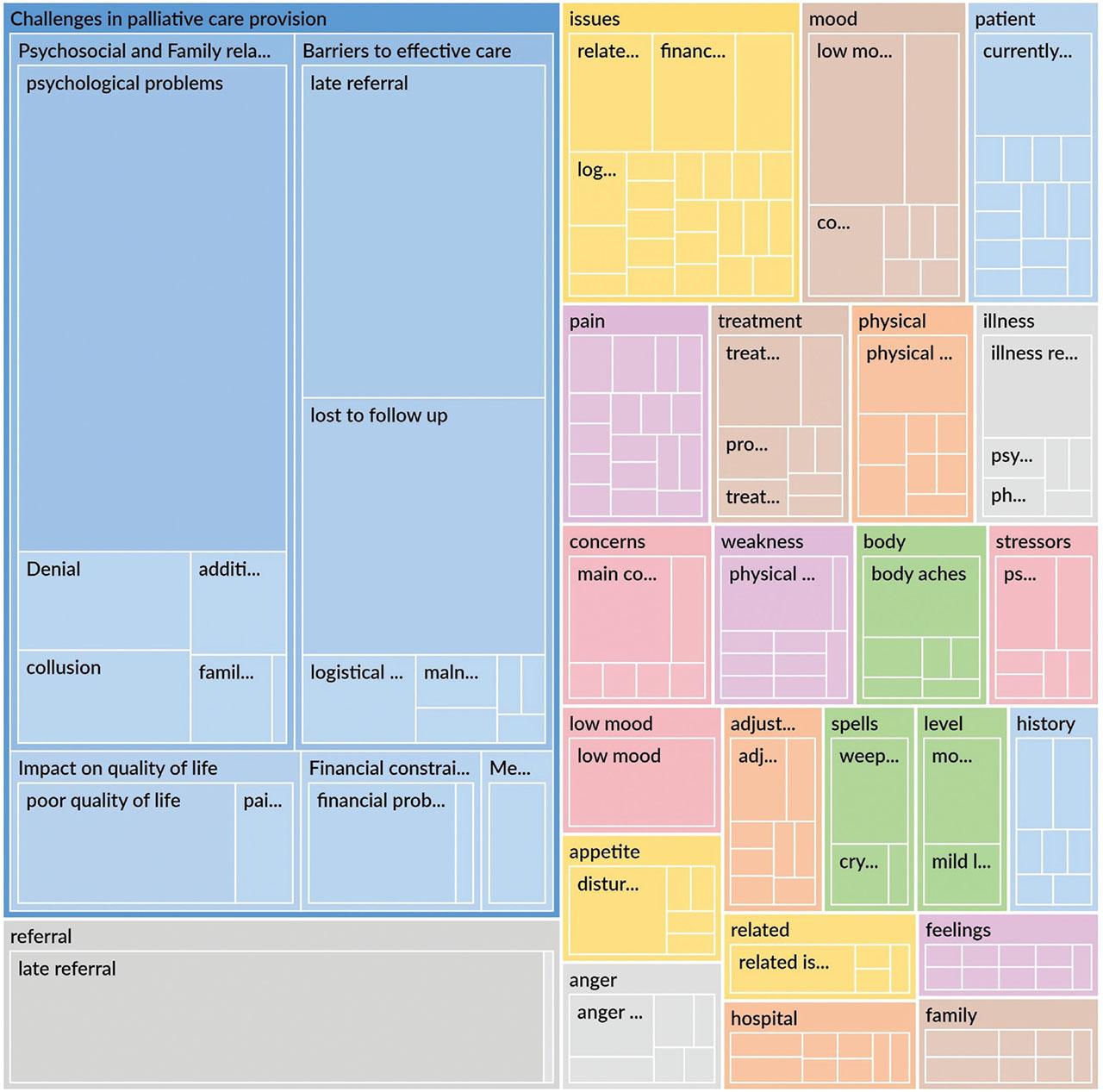
Hierarchy of themes derived from documented pediatric palliative care encounters.
This diagram illustrates the five main themes and associated sub-themes identified through Reflexive Thematic Analysis.
One of the major challenges identified in this study was the delay in referrals. Many children were introduced to PC only after curative treatments had failed, leaving insufficient time for effective symptom management and emotional support. Most patients had advanced disease and died within three months of referral to PC, as noted.
Disruptions in continuity of care were another notable barrier to effective service delivery. Clinician notes described limited awareness among families regarding the purpose of PC and its role in improving QOL. One entry stated, “The family asked for the next appointment for chemotherapy,” reflecting confusion about the shift from curative to palliative intent. Several notes documented families declining further visits after being informed that curative treatment was no longer possible, as expressed by one parent: “We will take our child back home if no cure is possible.” Furthermore, logistical barriers and financial constraints led to lost to follow-up, thereby rendering the care ineffective.
Denial of palliative treatment, coupled with language barriers, also limited access to proper care. One note mentioned that a patient “spoke Kurdish, and no interpreter was available,” which affected communication and understanding of care plans. Some patients from Afghanistan were lost to follow-up, and clinician notes indicated difficulties returning for care due to border-related issues. One note recorded, “Patient’s father reported they could not come for follow-up due to border closure.”
The major psychosocial stressors experienced by pediatric patients in this study were multifaceted, with several factors contributing to emotional and psychological distress. Clinician notes described work-related challenges, sleep disturbances, and nightmares as common issues. Hospital anxiety, difficulty adjusting to the hospital environment, and the emotional strain of being separated from family members added further stress. One child was recorded as saying she “missed her mother and wanted to go back home,” while another was noted to be “crying because he missed his siblings and wanted to play with them.” Adolescents, in particular, faced significant psychosocial challenges, including low self-esteem related to body image concerns and increased dependency, especially following amputation in osteosarcoma patients. This appeared to contribute to social isolation and limited physical activity. In one case, parents reported that their son “stayed all day long in his room,” reflecting reduced social engagement following treatment.
The prolonged nature of treatment, coupled with poor treatment response, was associated with irritability, aggressiveness, and exacerbated psychological distress. Many children had difficulty expressing their feelings and disease-related concerns, contributing to emotional strain for patients and their families. Clinician notes indicated pervasive family anxiety, with parents experiencing significant distress as they witnessed their children’s suffering. The fear of losing their child was a central stressor for many families. One family was noted saying, “he is the only living child, as they had recently lost their elder son.”
Anxiety and depression in patients were primarily associated with disease-related symptoms. One adolescent reported distress related to family circumstances, stating, “her husband has remarried and she feels emotional distress because of this,” highlighting how personal and family dynamics can also contribute to emotional distress. Suicidal ideation and behavior were observed in a few teenagers, often due to prolonged hospital stay and persisting symptoms. Clinician notes documented self-harm in one patient, noting “self-inflicted cuts on her wrist.” Uncontrolled pain was frequently reported in triggering such thoughts and actions. Some patients declined pain management, which was associated with increased anxiety, depressive symptoms, and, in a few cases, suicidal ideation, according to clinician observations.
Frustration from being unable to carry out daily activities due to pain and immobility, coupled with unmet expectations regarding their prognosis, added to the patients’ emotional burden and in some anger issues. Relationship issues between parents, high expectations, and difficulties arising from cross-border issues further contributed to the psychological strain experienced by both the patients and their families.
Suffering due to inadequate pain control or lack of support adversely impacted QOL. Poor mobility, postural instability, being bed-bound, wheelchair bound, and use of crutches/prosthesis in these patients negatively impacted the QOL. One patient was noted to be “from a hilly area, struggled to use a prosthesis on uneven terrain, and mobilized on a donkey,” highlighting the challenges of adaptation in a rural setting.
Financial difficulties were also observed as a theme in this study. Although the hospital covered the treatment costs, many families faced financial strain from travel expenses, making it hard to continue follow-up. This financial burden, often noted in counseling sessions, worsened the emotional and physical stress for both patients and their families.
Financial constraints, driven by unemployment and low income, hindered access to PC. One father shared, ‘He left his job to look after his daughter,’ while another family reported “living in a single-room house”. These challenges contributed to loss to follow-up and worsened QOL, with some patients returning to the hospital in the terminal phase.
Some patients did not follow the prescribed treatment plan, and families were sometimes unable to ensure adherence to analgesics. A grandfather reported, “His grandson did not want to take any medications.” Several patients returned with uncontrolled pain, making them dissatisfied with care.
The most common observed barrier to effective PC was delayed referrals. This delay often resulted from physicians’ lack of awareness about the importance of timely referrals, mistaking them for end-of-life care, and families’ unawareness of its benefits. Similar issues were reported in Japan, where families cited late referrals due to misunderstandings about palliative care, poor communication with doctors, and reluctance to accept the patient’s worsening condition [6]. Similarly, in a systematic review in India, PC referrals were perceived as a sign of surrender and linked to death [7]. These findings suggest that, in addition to cultural hesitancy, structural barriers, such as limited physician training and a lack of clear referral protocols, amplify delays in PC provision. Addressing these barriers through educating doctors and families and standardizing referral processes could help improve timely access and QOL for children with serious illnesses.
Discontinuity in care was mainly due to patients lost to follow-up and to a range of logistical, financial, and sociopolitical barriers. These included travel constraints, border closures, and language barriers, as well as patient factors, such as denial and limited understanding of PC. Some Afghan patients faced additional challenges due to the ongoing political crisis, border closure, war, and terrorism, which led to loss of follow-up care. This highlights how regional political instability can significantly affect healthcare access, creating barriers beyond the control of healthcare providers. Such geopolitical influences on PC delivery appear to be unique; similar challenges have not been prominently reported in the literature from either developed or developing countries. For example, a randomized controlled trial reported that 53 out of 146 patients were lost to follow-up within one month, primarily due to early deaths (n=36) or incomplete follow-up questionnaires [8]. In contrast, lost to follow-up in this study was largely driven by structural and sociocultural factors, such as financial hardship, travel difficulties, and border restrictions, rather than mortality or procedural noncompletion. This contrast highlights the importance of contextual factors in shaping continuity of care, particularly in LMIC settings, where systemic and geopolitical challenges can be as consequential as clinical outcomes in determining patient follow-up and care completion.
Psychological distress was a major obstacle in providing effective PC, particularly among adolescents. Both patients and their families commonly experienced anxiety and depression related to disease progression, uncertain outcomes, and strained parental relationships. In extreme cases, suicidal ideation, anger, and frustration were reported, often exacerbated by persistent pain and prolonged hospitalization. These challenges affected PC provision by reducing patients’ engagement with treatment and follow-up, complicating symptom management, and straining communication between families and healthcare providers, especially in families who had previously experienced the loss of a child. These findings highlight how untreated psychological distress can undermine the goals of PC. Similar findings have been reported in a prospective study, where high rates of depression among PC patients, especially younger individuals and women, were linked to poorer quality of life, strained relationships, and difficulties in symptom control [9]. Addressing mental health needs through early psychosocial support and counseling is therefore essential to improve adherence, patient comfort, and continuity of PC.
Refusal or inability to follow the treatment plan, along with families’ difficulties in ensuring their child adhered to prescribed pain medication, led to patients returning with uncontrolled pain. This caused dissatisfaction with the PC team and hindered efforts to improve the patients’ QOL.
Collusion emerged as a major family-related challenge in the provision of PC. In many cultural contexts, male family members are the decision-makers and often control the flow of medical information, limiting open communication between clinicians, patients, and female family members. In this study, this dynamic was evident as female relatives were frequently excluded from discussions and decisions regarding the patient’s condition, with some women even unaware of their own diagnosis. Societal expectations and domestic responsibilities often kept mothers from visiting the hospital, leaving elderly relatives such as grandparents to accompany children. This exclusion hindered information exchange with the care team, adversely affecting management and contributing to emotional distress and loneliness among pediatric patients deprived of maternal support. A prospective study in India highlighted similar issues, noting that familial hierarchies contributed to collusion, with women often the primary caregivers, being left out of crucial conversations about the diagnosis [10].
Denial about disease progression and prognosis was also observed. Upon disclosure by the palliative team, many patients and families were in denial and exhibited emotional responses. This reaction often delayed their acceptance of the illness and affected the quality of PC. In a literature analysis, denial emerged as both a coping mechanism and a barrier, providing temporary psychological protection while delaying crucial discussions about end-of-life care. Prolonged denial hindered key elements of PC, including discussions about advance care planning, symptom management, discussions about death, and cessation of futile treatments, ultimately obstructing the essential conversations necessary for comprehensive PC. [11]. This was particularly evident in our population, where cultural reluctance to discuss death appeared to reinforce denial, delaying timely palliative interventions and potentially compromising quality of care.
Immobility significantly affects the quality of life of terminally ill cancer patients, as was noted in this study, where amputations and lack of prosthesis led to dependence and reduced daily functioning. Similar findings were reported by Roh et al. (2014, who observed that older cancer patients in PC had low mobility levels closely linked to pain, fatigue, and sleep disturbance [12]. Likewise, Barbosa et al. (2024 found that children and young adults with cancer showed poorer functional mobility and daily activity performance than healthy peers [13]. These studies, together with our findings, highlight that immobility remains a major barrier to QOL across all age groups.
In addition, medication non-compliance due to financial hardship, limited understanding, or fear of side effects further reduced comfort in our patients. In PC settings, non-compliance remains a key challenge, with healthcare providers noting that “although we treat the patient properly and on time, the patient fails to follow the advice given to them, and their condition does not improve or even worsens” [14]. Financial constraints further worsen outcomes by limiting follow-ups and access to medications, adding emotional and physical stress for patients and families. Compared to behavioral non-compliance, financial barriers are structural, restricting care despite proper guidance. A pilot study showed that financial hardship, QOL, and symptom burden are strongly linked [15]. Both factors highlight the need for holistic support addressing clinical, psychosocial, and economic needs to improve adherence and QOL.
Major barriers to care included late referrals, loss to follow-up, psychosocial and family-related challenges, poor QOL, financial constraints, and medication non-compliance.
To overcome the barrier of lost to follow-up and reduce the financial burden of travel, a recent initiative by the hospital’s PC team, “Palliative Home Care Service and Helpline,” has been a valuable resource for patients who cannot regularly visit the hospital, especially those who are bedridden. The helpline improved follow-up by maintaining contact with the PC team, while the home service provided in-home support, reducing travel and logistical burdens.
To raise awareness of PC in rural areas, especially for those with chronic illnesses, we propose involving Lady Health Workers (LHWs), who are trusted and have easy access to these communities. By training LHWs in PC principles, they can effectively educate the population and increase awareness of PC services.
This retrospective qualitative review has certain limitations due to its reliance on patient notes; therefore, it does not fully reflect all challenges in providing PPC. The absence of direct patient and caregiver perspectives, incomplete documentation, and limited multidisciplinary input may have restricted insights. A prospective study with full resource availability is suggested. Providing PC to terminally ill children is fraught with challenges, ranging from healthcare system barriers and financial constraints to family struggles and non-compliance. The challenges and barriers identified in this study highlight the need for a multidisciplinary approach to care provided by the palliative medicine team. Efforts should focus on raising PC awareness, improving pain management, and strengthening psychosocial support for children and caregivers. By addressing these challenges, we can ensure that every child facing a life-limiting illness receives the compassionate and holistic care they deserve. We plan a prospective study to further explore challenges in PPC and identify actionable solutions.