Early and progressive mobilization has been suggested as a safe and effective intervention.1 The rehabilitation nurse (RN) in the intensive care unit (ICU) provides holistic and adapted care to the critically ill person, to minimize, among other complications, neuromuscular changes, as these are one of the most common and devastating complications.2 The aim of this case study is to identify the health gains made by the RN in an early mobilization program in the ICU.
Mobilization should begin as soon as possible and is recommended to be started up to 72 h after admission to the ICU,3 as long as hemodynamic stability is ensured. This case report describes the treatment complexity in an intensive care setting of a surgical patient who developed acute respiratory distress syndrome (ARDS), who further developed cardiovascular, hematological, and ventilator instability. This was the reason to postpone the early mobilization with regard to the rehabilitation program by about 8 days. The decision was made based on the rehabilitation specialist nurse’s critical thinking and decision making skills, ensuring that safety criteria guidelines adopted by the ICU were met at all times.
This patient presented with multiple comorbidities, in need of prolonged invasive mechanical ventilation as well as a prolonged stay in intensive care. During that time, the patient required to be positioned in the prone position and presented severe Intensive Care Acquired Muscle Weakness (Medical Research Council of 24), and maintained Intensive Care Acquired Muscle Weakness on his last day of intensive care stay (Medical Research Council of 46).
This case report describes a 65-year-old male, Caucasian, Portuguese nationality, single, living with his brother, and previously independent in his daily living activities. The following comorbidities were identified: obesity, hypertension, degenerative osteoarticular disease, and peripheral venous insufficiency. He looked for assistance with his local primary healthcare service on June 4, 2022 for generalized abdominal pain and an increase in abdominal perimeter, which had been going on for 4–5 days. After clinical observation, he showed improvement in respiratory function, transferred to a specialized healthcare environment (emergency department), and then to the emergency room because of a suspected acute abdomen. He remained awake and in pain despite receiving analgesia, but then quickly developed an altered conscious state. Skin appeared pale and jaundiced. Although no signs of respiratory distress were observed at this point, his PaO2/FiO2 ratios were progressively worsening, requiring a higher FiO2 supply, 50% O2 supply via Venturi mask (Intersurgical, Lithuania; distributed in the USA, East Syracuse). Gas analysis: pH 7.45; pCO2 23 mmHg; pO2 59 mmHg; HCO3 16 mmol/L; SatO2 91%; lactates 3.7 mmol/L; glucose 174 mg/dL. Regarding other complementary diagnostic tests, the computerized tomography (CT) scan revealed small areas of pneumoperitoneum. The case was discussed with the surgical team, and the patient was transferred to the operating theatre for an exploratory laparotomy. He was then transferred to the ICU with a diagnosis of pneumoperitoneum and septic shock with severe multiple organ dysfunction, and was discharged on June 30, 2022.
The evolution of the patient’s stay in the ICU in illustrated in Figure 1. In the first 24 h after admission to ICU, this patient was given, using the Simplified Acute Physiology Score II (SAPS II) a score of 54, a score of 22 using the acute physiology and chronic health evaluation score II (APACHE II), a score of 15 using the sequential organ failure assessment (SOFA) and a score of 39 using the therapeutic intervention scoring system 28 (TISS 28). This patient presented several concomitant risk factors for developing acquired muscle weakness in the intensive care unit (AMWICU), such as hyperglycemia, parenteral nutrition, vasopressor therapy use, sedation, certain types of antibiotic therapy, neuromuscular blockers, and high doses of corticosteroid therapy for a significant period of time,4 along with ventilator weaning attempts and associated delirium.
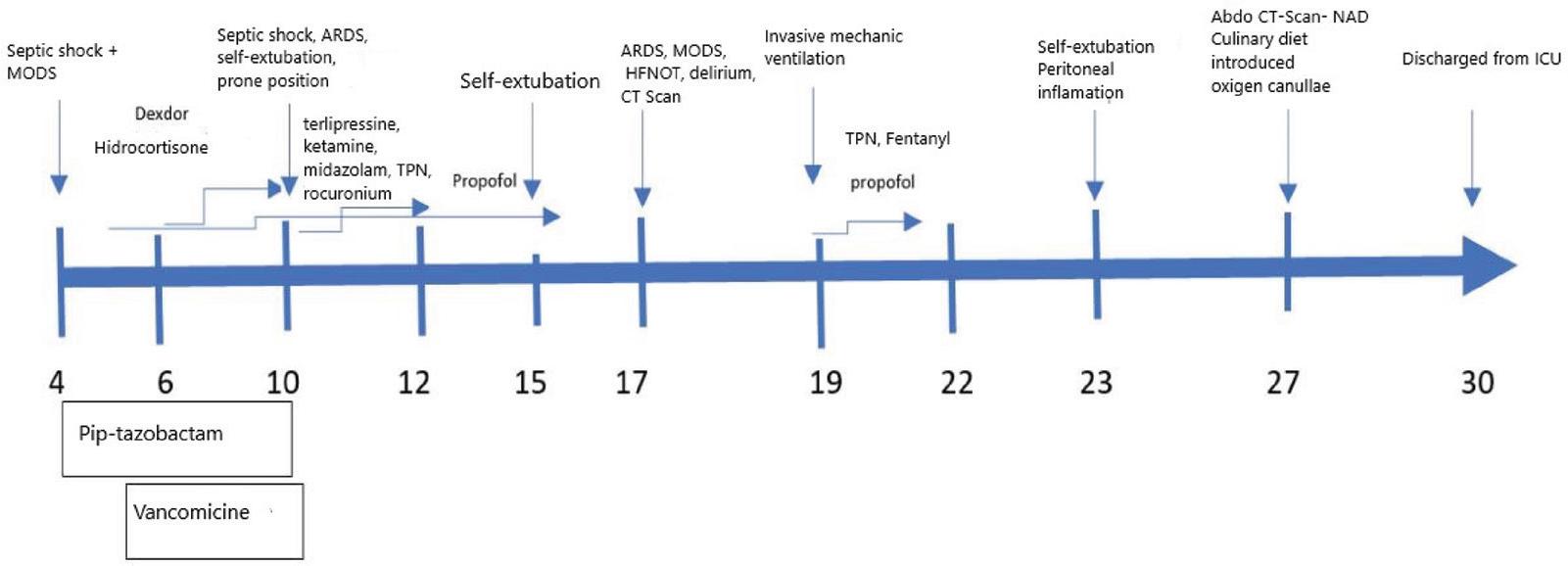
ICU stay timeline. Abbreviations: ARDS, acute respiratory distress syndrome; CTscan, computerized tomography; HFNO, high flow nasal oxygen therapy; ICU, intensive care unit; MODS, multiple organ dysfunction syndrome; TPN, total parenteral nutrition.
Early mobilization is considered a complex nonpharmacological nursing intervention with proven physical, psychological, and cognitive benefits.5
The rehabilitation program began on the June 13 until the date of the patient’s discharge from the ICU and was set up by an RN on both morning and afternoon shifts for 7 days a week. It was implemented to meet the needs of the patient in critical condition, following a set of principles that take into account neurological assessment using the Glasgow Coma Scale, agitation and sedation using the Richmond agitation—sedation scale (RASS), pain assessment using the Pain-Indicating Behaviors Scale (ESCID) or the numerical pain scale depending on the patient’s consciousness state, and delirium using the confusion assessment method for the ICU (CAM-ICU) scale. The patient’s cooperation is assessed using the standardized questions for cooperation scale (S5Q-S). The medical research council (MRC) scale for muscle strength was used to measure muscle strength, and the patient’s mobility in an ICU environment was assessed using the ICU mobility scale.
The patient was assessed daily by the RN to adjust the intervention type in order to achieve the best possible outcome, establishing which type of mobilization was possible for each day.
The program takes into consideration all the 7 categories based on expert consensus6 (neurological, respiratory, cardiovascular, hemodynamic, hematological, and others). For each category of consideration, there are several items with a color-coded symbol and a traffic light system for the exercises to be performed in bed and out of bed. The color green means low risk, yellow moderate risk, red high risk (Table 1), taking in consideration the following guiding principles: it ‘s adapted to the person in critical condition; it’s an intervention carried out exclusively by ICU RN, whose role is to provide specialized rehabilitation care in this context; it’s carried out individually and in the patient’s unit; in the “lift” and “transfer” activities, whenever necessary, the collaboration of the multidisciplinary team is requested; the mobilization intensity recommended to be 10 repetitions per joint segment, with the resistance being adapted to each patient; the degree of the exercises is based on tolerance and based on safety criteria; when a patient performs the planned activities at a certain level, they move on to the next level.
Safetycriteria.
| Conditions | Mobilization in bed (mobility scale 0–2) | Mobilization out of bed (ICU mobility scale 3–10) | Date | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 5/06 | 6/06 | 7/06 | 8/06 | 9/06 | 10/06 | 11/06 | 12/06 | |||
| Hemodynamic status | ||||||||||
| Unstable, with changes ≥ during bed exercises | ◊ | ◽ | √ | |||||||
| Stable with vasopressors | + | ◊ | ||||||||
| Addition of antiarrhythmics in the last 24 h | ◽ | ◽ | √ | √ | ||||||
| Hematological status | ||||||||||
| Hemoglobin > 7g/dL | + | + | ||||||||
| Hemoglobin ≤ 7g/dL | ◽ | ◽ | √ | √ | ||||||
| Platelets ≤ 20,000/mm3 | ◽ | ◽ | √ | |||||||
| Other | ||||||||||
| Prone position | ◽ | ◽ | √ | √ | ||||||
Note: ◽ = Red, mobilization contraindicated; ◊ = Yellow, individual decision; √ = Green, active mobilization; ICU, intensive care unit.
From the 13th to 15th of June, the patient had a RASS—4 (deep sedation);—2 (light sedation), scale of 3 (light pain) using the ESCID. Since the patient was sedated, delirium, cooperation, and muscle strength were not assessed, as the application of the scales implies the person’s cooperation. The level reached on the ICU mobility scale was 0, which describes active mobilization as contraindicated. The intervention performed by RN was massage, positioning, and passive muscle exercises to preserve the range of movement and elevation of the headboard between 30° and 45°.
On the 9th of June, the patient’s RASS score ranged from -1/+1, which means the conscious status was oscillating between a confused and restless period; with pain of 3 (moderate) using the modified numerical scale; muscle strength was not assessed, the level reached on the ICU mobility scale was 2. The intervention consisted of passive exercises in bed, passive lifting, and sliding transfer to the chair, where he remained for about 1 h. He then received the same treatment in the afternoon shift.
Between the 22nd and the 25th of June, AMWICU is diagnosed using the MRC scale, being assessed twice within a 24-h interval. On the 25th of June, the patient had a RASS of 0 (awake and calm), maintaining the same score on the ICU mobility scale.
Between the 28th and the 30th of June, the patient maintained a RASS of 0, with no pain, without delirium, cooperative, muscle strength evolved from 36 to 46, scored 5 on the ICU mobility scale. The patient was then able to perform active exercises out of bed, step onto the floor, move his feet to the chair, and actively transfer load from one limb to another. On the 30th of June, the patient scored 6 on the ICU mobility scale, showing the ability to march on the side of the bed, alternately lifting his feet off the floor, demonstrating the ability to take steps, at least 2 steps per foot, with or without assistance, as can be seen in Table 2.
Neurological and motor assessment results.important because it is the technical-scientific knowledge and the respective alignment between theory and evidence-based practice that enables the development of various non-pharmacological nursing interventions, always based on clinical decisions and responsibilities, which subsequently translate into the results obtained by the critically ill patient.
| Assessments | Date | ||||||
|---|---|---|---|---|---|---|---|
| 13/06 | 15/06 | 19/06 | 22/06 | 24/06 | 28/06 | 30/06 | |
| Neurological assessment | |||||||
| Agitation and sedation (RASS) | –4 | –2 | –1/+1 | +1 | 0 | 0 | 0 |
| Pain (ESCID scale; numerical scale) | 3 | 3 | 3 | 3 | 0 | 0 | 0 |
| Delirium (CAM ICU scale) | NA | NA | S | S | S | N | N |
| Cooperation (S5Q scale) | 0 | 0 | 4 | 4 | 4 | 5 | 5 |
| Motor assessment | |||||||
| Muscle strength (6 degrees MRC scale) | NA | NA | NA | 24 | 24 | 36 | 46 |
| ICU mobility (ICU mobility scale) | 0 | 0 | 2 | 2 | 2 | 5 | 6 |
Note: CAM-ICU, confusion assessment method for the ICU; ESCID, pain indicating behaviors scale; ICU, intensive care unit; MRC, medical research council for muscle strength scale; NA, not applicable; RASS, Richmond agitation—sedation scale; S5Q-S, standardized questions for cooperation scale.
Systematized procedures within the multidisciplinary team in the ICU is the aim of implementing rehabilitation nursing intervention program, to prevent potential permanent damage associated with immobility, promoting early recovery, endorsing improved results for people in critical situations, reflected in increased muscle strength, increased level of functional independence, reduced days of invasive mechanical ventilation, reduced length of stay, reduced number of hospital readmissions, reduced mortality, and increased quality of life.7
As part of the clinical reasoning process, people with complex needs arising from increasing morbidity require complex nursing interventions from highly competent nurses.8–10
This case report provides an accurate version of the hospitalization of a patient who spent 26 days in ICU with a diagnosis of pneumoperitoneum and septic shock with multiple organ dysfunction syndrome (MODS). With SAPS II severity index of 54, APACHE II severity index of 22, SOFA severity index of 15, and a TISS 28 severity index of 39, the patient required invasive mechanical ventilation with several unsuccessful ventilator weaning. With episodes of delirium and a diagnosis of AMWICU with associated risk factors for its development, such as septic shock, prolonged invasive mechanical ventilation, MODS, vasopressor therapy, sedation, antibiotic therapy, neuromuscular blockers, corticosteroid therapy, and insulin therapy.4
The early mobilization program implementation by RN enabled gains to be made for the patient, pointing toward the increase in muscle strength and mobility in the ICU, improving the mobility and quality of transfer through an increase in the score on the ICU mobility scale.7,11 The diagnosis of AMWICU allowed the intervention to be adequately directed in terms of the type of exercise, although the ideal quantity (frequency, level, or duration) is still uncertain,11 an individualized program was chosen. There was also a decrease in delirium throughout the program, which states that mobilization is considered a fundamental strategy in the management of delirium, and early mobilization may be the first known intervention to prevent cognitive impairment in critically ill patients undergoing invasive mechanical ventilation.12,13 The programs instituted by RN are essential to optimize nursing interventions. Their effectiveness depends on the congruence, line of action, knowledge, and being able to share the same goals by the RN team. The implementation of early mobilization needs to be considered individually based on the patient’s purpose, using the best evidence, optimizing safety, and the recovery of the level of functional independence, thus minimizing the risks.7
Early mobilization is supposedly the first intervention that has been shown to improve cognitive impairment, quality of life, and AMWICU in the critically ill patient. As a significant area of nursing concern, early mobilization as a complex intervention should be included in the nursing care plan.
The early mobilization program, as part of the rehabilitation of the critically ill patient, is particularly important because it is the technical-scientific knowledge and the respective alignment between theory and evidence-based practice that enables the development of various non-pharmacological nursing interventions, always based on clinical decisions and responsibilities, which subsequently translate into the results obtained by the critically ill patient.