Dementia is a chronic, irreversible, and neurodegenerative disease that affects cognitive functions, behavioral and motor functions, and physical abilities.1 Currently, it is incurable, with limited success from treatments such as anti-dementia medications and disease-modifying therapies. Since dementia is a complex syndrome, it negatively affects the people who are living with dementia. Given the necessity of complex care, it adversely impacts carers and society.2 Dementia is a global health problem and is common among older people. Globally,more than 55 million individuals are affected by dementia, and approximately 10 million people are diagnosed with dementia every year.3 Nearly two-thirds of individuals with dementia reside in low- and middle-income countries (LMICs).4 A recent review indicated inadequate early detection, delayed diagnosis, and limited availability of community services in dementia care.5 Consequently, particular focus must be given to advancing dementia care, especially in LMICs.
Given the high dementia population, more healthcare professionals are required to address the care needs of people with dementia.6 A fundamental understanding of this insidious syndrome7 and the continuous development of knowledge and skills among healthcare professionals are essential.8 Empowering healthcare workers allows for early detection, treatment, care provision, and disease prevention.9 Nursing is vital for caring for people with dementia in different settings, such as hospitals, aged care facilities, and communities. Therefore, nurses should have adequate knowledge of dementia care; however, the literature indicates poor knowledge concerning dementia care among nurses10,11 and nursing students.12,13
Moreover, recent literature indicates that nurses and nursing students in LMICs need more knowledge and higher preparation for caring for older people.14 Therefore, nurses experience profound care challenges in caring for people with dementia.15 In light of this situation, nurse professionals should be adequately trained to provide care for people with dementia in LMICs.
Sri Lanka is one of the LMICs in the South Asian region, with an increasingly older population. In 2015, approximately 147,000 Sri Lankans were predicted to have dementia, which is expected to reach 262,000 by 2030 and 463,000 by 2050.16 Sri Lanka Association of Geriatric Medicine17 emphasizes the need to pay special attention to dementia care; however, limited resources make comprehensive care difficult in the country. According to a recent review, dementia research in Sri Lanka has been lacking, especially concerning the prevalence, profiles of formal and family carers, care considerations, and supportive services.18 To our knowledge, no studies have explored dementia knowledge among health professionals, particularly nurses and nursing students, in Sri Lanka. Therefore, the assessment of dementia knowledge among this population is a priority.
Recently, the Dementia Knowledge Assessment Scale (DKAS) has been utilized to measure knowledge about dementia among different study cohorts, such as nurses,19 nursing students,20 and carers.21 The DKAS-25 item version, developed by researchers in Australia22, has been used in his study. It is a 5-point Likert scale with true/false statements. It has been translated and cross-culturally adapted into several languages: Indonesian,20 Chinese,23 Japanese,7 Singaporean,21 Spanish,24 and Turkish.9 There is no well-established, culturally accepted tool for assessing dementia knowledge in local languages in Sri Lanka. Therefore, this study aimed to develop the Sinhala version of the DKAS (Si-DKAS) and test its psychometric properties with a sample of nursing students in Sri Lanka.
A cross-sectional validation study was conducted in two phases: (i) questionnaire translation and adaptation (cultural adaptation process) and (ii) evaluating psychometric properties. The DKAS-25 item version has been translated and adapted with prior permission from the original authors (Cronbach’s alpha = 0.85).22 In scoring the DKAS, two points were assigned to a correct answer.23 One point was assigned for the answers of “probably true” to an accurate statement of the DKAS, and one point was assigned for the answers of “probably false” to a false statement of the DKAS.23 Zero points were assigned for the answers of “wrong” or “I do not know.”23 Total and subscale scores were calculated by summing points for each item, with a maximum of 50 points on the total scale.23
The World Health Organization guidelines for translating and adapting instruments were followed.25 This process included forward translation, backwards translation, pretesting with cognitive interviewing, and developing the final version.25
A bilingual nurse educator translated the original version in English into the Sinhala language, ensuring conceptual rather than literal translation. A panel of four health experts and a layperson reviewed the translated version. The forward translation was back-translated into English by an independent translator whose mother tongue was Sinhala, who was fluent in English and had no prior knowledge of the DKAS. Five health experts compared the back-translation with the original version to examine semantic equivalence. Eleven nursing students participated in the pretest, followed by cognitive interviews with them to evaluate the readability and understandability of the items. It also helped to establish face validity. They suggested making changes to the unclear sentences. Finally, a language expert fixed grammatical issues.
In the next stage, 12 health experts evaluated the content relevance using a 4-point Likert scale ranging from not relevant (1 mark) to highly relevant (4 marks). The content validity index (CVI) was calculated for each item on the scale Item-Level Content Validity Index (I-CVI) by dividing the number of examiners who rated 3 or 4 by the total number of examiners.23 The CVI for the total scale Scale-Level Content Validity Index (S-CVI) was determined by calculating the average I-CVI across items.23 I-CVI > 0.78 and S-CVI > 0.8 were considered adequate.26 The experts’ opinions were sought to ensure face validity, which involved identifying whether the items clearly and unambiguously addressed the topic of the scale.27 Their suggestions were incorporated into the scale with the approval of the original developers. This version was used in further psychometric evaluation (the prefinal version of the Si-DKAS).
A cross-sectional survey was conducted to establish the reliability and validity of the Si-DKAS.
A purposive sample of nursing students who followed the Diploma in Nursing Program at one Government School of Nursing attached to the Ministry of Health, Sri Lanka, participated in the study. We invited all the students (n = 565) enrolled in the Diploma Nursing Program during the data collection period. Students who were illiterate in Sinhala and who participated in the pretest were excluded.
A self-administered questionnaire comprising sociodemographic variables and the prefinal version of the Si-DKAS was utilized. The sociodemographic variables included age, gender, academic year, dementia training,22 and students’ preferences for future dementia care.
Necessary permission was obtained from the Principal, School of Nursing (Kadana), Sri Lanka. Initially, the researchers invited students through social media groups (i.e., WhatsApp). Due to the Coronavirus Disease 2019 (COVID-19) guidelines imposed, two batches were physically presented to the school. One of the researchers met students, introduced the study, and distributed written information sheets. Written informed consent was obtained from each student who fulfilled the inclusion criteria and provided consent to participate in the study. The students who did not present physically at the school completed the questionnaire online through a Google Form. Invitations with information sheets and survey links were distributed among them through social media groups (i.e., WhatsApp). Filling and returning the online forms implied their consent to participate in the study. Two weeks after the initial research, a subsample of students participated in the test–retest assessment.
The data were analyzed using the IBM Statistical Package for Social Sciences (SPSS, version 25, IBM Corporation, Armonk, New York, United States) and IBM SPSS AMOS (version 28, IBM Corporation, Armonk, New York, United States). Descriptive statistics were computed to characterize the sample, including frequencies, percentages, means/medians, and standard deviations. The Shapiro‒Wilk test was used to assess the normality of the data. A significance level <0.05 was used to indicate statistically significant findings. Reliability and validity were determined.
Internal consistency was evaluated by computing Cron-bach’s alpha and item-total correlation (ITC). Concerning stability, the test–retest reliability was computed to assess the intraclass correlation coefficient (ICC). A Cronbach’s alpha >0.70,28 an ITC >0.3,29 and an ICC >0.7028 were acceptable.
Construct validity was assessed using exploratory factor analysis (EFA), confirmatory factor analysis (CFA), and discriminant validity. In previous studies, the replicability of the four-factor structure of the 25-item DKAS was assessed through CFA.21,23 Accordingly, CFA was performed in the present study by importing the data into AMOS (version 28).22 Several parameters were considered when evaluating the suitability of the hypothetical model based on the CFA. The significance of the chisquare results indicates the rejection of the hypothetical model.30 A good fit of the model indicates an χ2/df (chisquare divided by the degree of freedom) ratio <3.0, fit indices ≥0.90, a standardized root-mean-squared residual (SRMR) <0.08, and a root-mean-squared error of approximation (RMSEA) <0.06.31–33 The model fit statistics of the prefinal version of the Si-DKAS were not within these acceptable levels. Therefore, EFA was undertaken to explore the factor structure of the Si-DKAS for Sinhala-speaking nursing students.
The principal component analysis (PCA) was used for EFA. The factorability of the Si-DKAS was examined by three approaches: (i) computing interitem correlations (correlations should be at least 3 with at least 1 other item), (ii) the Kaiser–Meyer–Olkin (KMO) statistics of sampling adequacy (accepted value >0.6), and (iii) Bartlett’s test of sphericity (needs to be significant).34,35 The number of factors to retain was determined based on the Kaiser Guttman rule (the eigenvalues of >1.0 were set for retention), a scree plot (plotting the eigenvalues against the number of variables present), and parallel analysis.36–38 The factor loading criterion of the scale items was computed by an orthogonal factor solution, thus Varimax rotation with Kaiser normalization.39 CFA and PCA finalized the Si-DKAS. The final version was used to measure the discriminant validity, descriptive statistics of the sample, and reliability statistics.
Knowledge differences determined discriminant validity. It was hypothesized that the students who completed dementia care as a part of the basic curriculum would have higher knowledge scores than students who did not complete the above content. The Kruskal–Wallis H test was used to compare knowledge level scores.
The conceptual and idiomatic equivalences of the original and translated versions were assured during the translation process. At consensus meetings after each step of the adaptation process, the research team finalized the Sinhala version, which was used to assess face validity and CVI.
In the Si-DKAS samples, the I-CVI ranged from 0.8 to 1, while the S-CVI was 0.9. With reference to face validity, experts assured that the content of the DKAS seemed relevant to measuring the intended construct (knowledge of dementia). Based on the comments given by the panel of experts, minor revisions were made to a few wordings to enhance their clarity and readability. Furthermore, we emailed this version to the original developers to ensure their agreement on cross-cultural adaptation. They suggested changing a few words of the back-translation. Based on their comments, the research team prepared a prefinal version of the Si-DKAS.
The pretest indicated that the nursing students understood most of the items. They suggested simplifying medical terms for a few items; however, the developers of the DKAS advised leaving the words exactly as they were without adding meaning to the terms. It took approximately 30 min to complete the questionnaire. The research team finalized the prefinal version of the Si-DKAS following the pretest, and a language expert corrected a few grammatical issues. This prefinal version was used to assess the psychometric properties in phase two.
A sample of 420 students completed the questionnaire, and 16 responses were removed due to missing values. In the dataset, 10 outliers were identified. Therefore, 394 responses (effective response rate = 69.73%) were included in the final analysis. The poor response rate might be attributed to the issues arising from COVID-19, such as students being victims of COVID-19 or being quarantined and travel restrictions imposed by the government due to the pandemic during the data collection period. The Shapiro–Wilk test showed that the data distribution deviated from normal (P < 0.04).
The majority of the participants were female (89.8%). Their average age was 24.20 ± 3.48 years. The students in our study were in three academic years: the second year (who did not complete the mental health and psychiatric nursing module that consists of dementia care), the early third year (who completed the theory component of dementia care), and the end of the third year (who completed theory and clinical placement in dementia care). Table 1 shows the sociodemographic characteristics of the participants.
Characteristics of the respondents (N = 394).
| Sociodemographic characteristics | Mean | SD | n | % |
|---|---|---|---|---|
| Age (in years) | 24.20 | 3.48 | ||
| Gender | ||||
| Male | 40 | 10.2 | ||
| Female | 354 | 89.8 | ||
| Academic year | ||||
| Second year (no exposure to theory or clinical experience in dementia) | 127 | 32.2 | ||
| Early third year (completed the theory only) | 57 | 14.5 | ||
| End of third year (completed the theory and clinical experience) | 210 | 53.3 | ||
| Participation in other training related to dementia care | ||||
| Yes | 7 | 1.8 | ||
| No | 387 | 98.2 | ||
| Preference for providing care for people with dementia in future | ||||
| Strongly agree | 32 | 8.1 | ||
| Agree | 185 | 47.0 | ||
| Not decided | 149 | 37.8 | ||
| Disagree | 26 | 6.6 | ||
| Strongly disagree | 2 | 0.5 | ||
The Cronbach’s alpha value of the 25-item Si-DKAS was 0.715, indicating acceptable internal consistency. Given the non-normal distribution of the data, the ITC was assessed using the Spearman correlation.40 All items of the Si-DKAS were significantly correlated with the scale’s total score (P ≤ 0.001; rho range, 0.162–0.508). In this stage, items with weak ITCs (r < 0.3) were not removed: items 7, 10, 14, 15, 16, and 24. Items were not removed using a single criterion, but multiple criteria were used to remove or keep the items. It ensured that the potentially essential items were not prematurely removed to provide a comprehensive exploration of the factor structure.
Next, CFA was conducted. A few parameters led us to use maximum likelihood as the estimation method, including a kurtosis value of -10.052, continuous variables (0 = wrong, 1 = partially correct, 2 = correct), and a large sample size (N = 394). The literature revealed that the sample size could be classified as small (<100), medium (100–200), and large (>200).41 The first-order four-factor model (four factors based on the original version) was checked, in which items were directly related to the extracted factors.33 The chi-square was significant (P < 0.001), and fit indices (e.g., comparative fix index [CFI], Turker–Lewis index [TLI], RMSEA) were not within the acceptable levels, indicating the rejection of the current four-factor model. Given the model’s poor fit to the sample, EFA was performed (Table 2: Model 1).
Fit indices for CFA of the 18-item Si-DKAS
| Fit index | Values of Model 1 (25 items) | Values of Model 2 (21 items) | Value of Model 3 (18 items) |
|---|---|---|---|
| Chi-square (χ2) | P < 0.001 | P < 0.001 | P < 0.001 |
| χ2/df | 2.541 | 2.450 | 2.116 |
| CFI | 0.611 | 0.698 | 0.809 |
| TLI | 0.567 | 0.653 | 0.773 |
| SRMR | 0.048 | 0.047 | 0.040 |
| RMSEA | 0.063 | 0.061 | 0.053 |
Note: CFA, confirmatory factor analysis; CFI, comparative fix index; RMSEA, root-mean-squared error of approximation; Si-DKAS, Sinhala version of dementia knowledge assessment scale; SRMR, standardized root-mean-squared residual; TLI, Turker–Lewis index; χ2/df, chi-square per degree of freedom ratio.
The KMO value of sampling adequacy was 0.715, indicating a very good value. Bartlett’s test of sphericity was statistically significant (χ2 = 1334.553, P < 0.001). The initial PCA resulted in the loading of a seven-factor structure. The pattern matrix showed that two items (items 5 and 13) did not load on any factor and were removed from the scale. The second round of PCA was computed with a factor loading criterion of 0.4. A seven-factor structure was loaded. Examining the “total variance explained” table favored a four-factor solution. The scree plot generated through parallel analysis further supported the four-factor structure.
Third, PCA was undertaken with a fixed number of factor extractions (four factors), and a factor loading criterion of 0.4. The KMO measure and Bartlett’s test of sphericity were computed for this four-factor model. The KMO measure of sampling adequacy showed a good value (0.708). Bartlett’s test of sphericity was statistically significant (χ2 = 1190.400, P < 0.001). This four-factor solution was found to explain 36.36% of the variance across all items. Item 11 was cross-loaded on two factors. Considering the most significant loading factor and interpretability, item 11 was retained in this “health promotion” factor. Items 18 and 19 were not loaded on any factor and were removed. The remaining number of items was 21, and these items were loaded at a criterion of >0.4 onto one of the four factors. Factors 1, 2, 3, and 4 were labeled “care considerations,” “cause and characteristics of dementia,” “health promotion,” and “misconceptions about dementia,” respectively.
Next, CFA was conducted to confirm the model obtained from PCA, and the model fit was unsatisfactory. Three items with poor factor loadings (items 14, 15, and 16) were removed, resulting in an improved model fit for the 18-item Si-DKAS (Table 2: Model 3). However, the factor loadings of the five items (7, 9, 10, 12, and 24) were <0.4, ranging from 0.23 to 0.38. These items were kept from the scale to retain more items to assess knowledge. Figure 1 shows the factor loadings on the arrows from the latent variables (factors) to the observed variables (items). Table 3 illustrates the factor loadings and item communalities of the 18-item final version.
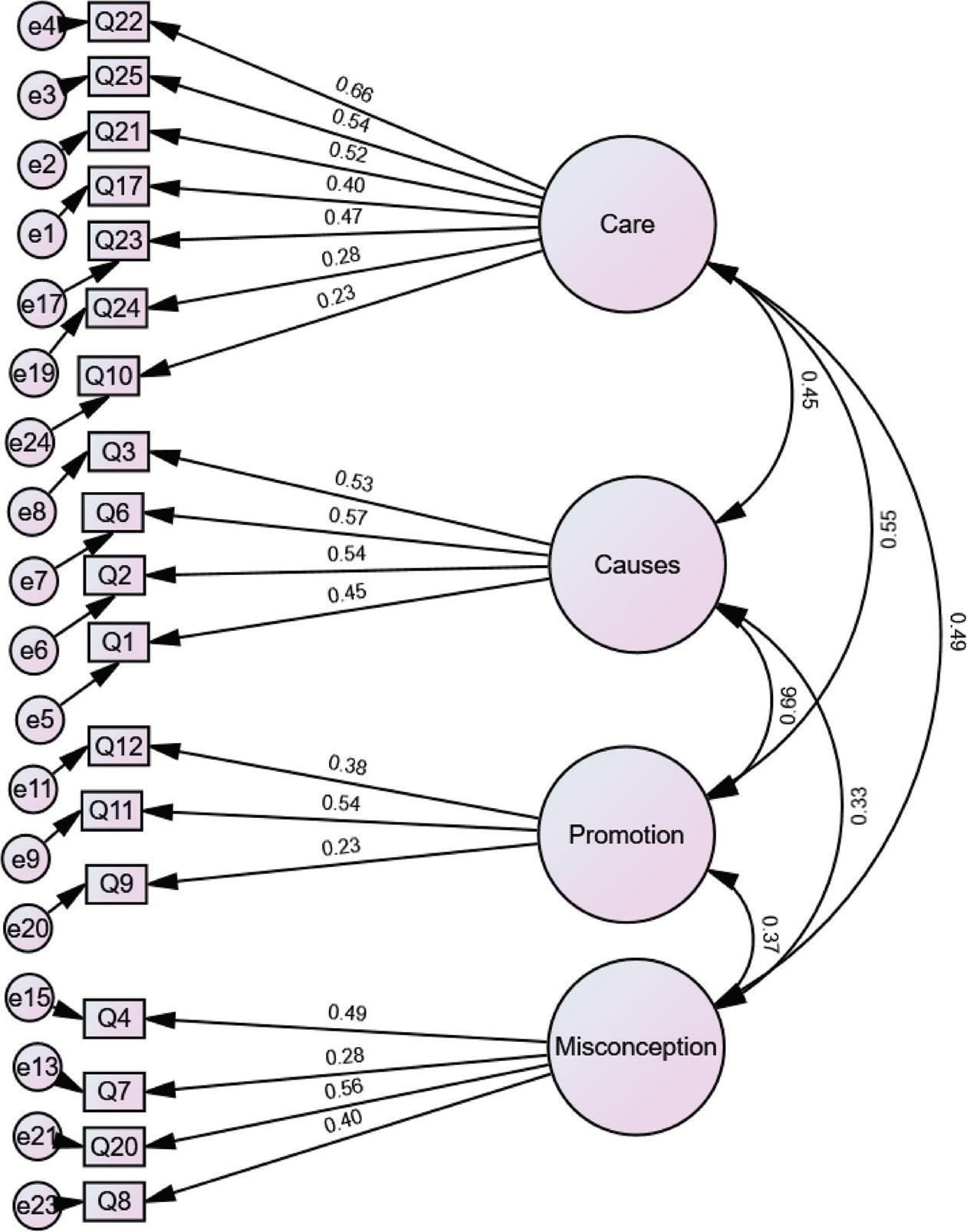
Path diagram*: CFA. Note: *The number of items was labeled based on the original version of DKAS.
Note: CFA, confirmatory factor analysis; DKAS, Dementia Knowledge Assessment Scale.
Rotated component matrix: factor loading and item communalities by PCA (N = 394).
| Item No. (original version) | Item No. (Si-DKAS) | Item | Component (factor) | Name of factors | Item communality (h2) | |||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||||
| 22 | 15 | People with advanced dementia may have difficulty speaking. | 0.619 | Care considerations | 0.478 | |||
| 25 | 18 | Daily care for a person with advanced dementia is effective when it focuses on providing comfort. | 0.549 | Care considerations | 0.372 | |||
| 21 | 14 | Movement is generally affected in the later stages of dementia. | 0.549 | Care considerations | 0.332 | |||
| 17 | 12 | People experiencing advanced dementia often communicate through body language. | 0.541 | Care considerations | 0.465 | |||
| 23 | 16 | People experiencing dementia often have difficulty learning new skills. | 0.522 | Care considerations | 0.341 | |||
| 10 | 9 | Symptoms of depression can be mistaken for symptoms of dementia. | 0.474 | Care considerations | 0.316 | |||
| 24 | 17 | Difficulty eating and drinking generally occurs in the later stages of dementia. | 0.406 | Care considerations | 0.178 | |||
| 3 | 3 | People can recover from the most common forms of dementia. | 0.699 | Causes and characteristics of dementia | 0.489 | |||
| 6 | 5 | Blood vessel disease (vascular dementia) is the most common form of dementia. | 0.668 | Causes and characteristics of dementia | 0.469 | |||
| 2 | 2 | Alzheimer’s disease is the most common form of dementia. | 0.563 | Causes and characteristics of dementia | 0.387 | |||
| 1 | 1 | Dementia is a normal part of the ageing process. | 0.560 | Causes and characteristics of dementia | 0.340 | |||
| 12 | 11 | Early diagnosis of dementia does not generally improve quality of life for people experiencing the condition | 0.588 | Health promotion | 0.382 | |||
| 11 | 10 | Exercise is generally beneficial for people experiencing dementia. | 0.438 | Health promotion | 0.399 | |||
| 9 | 8 | Maintaining a healthy lifestyle does not reduce the risk of developing the most common forms of dementia. | 0.431 | Health promotion | 0.331 | |||
| 8 | 7 | Having high blood pressure increases a person’s risk of developing dementia. | 0.685 | Misconceptions about dementia | 0.492 | |||
| 4 | 4 | Dementia does not result from physical changes in the brain. | 0.647 | Misconceptions about dementia | 0.444 | |||
| 7 | 6 | Most forms of dementia do not generally shorten a person’s life. | 0.440 | Misconceptions about dementia | 0.340 | |||
| 20 | 13 | People experiencing dementia do not generally have problems making decisions. | 0.435 | Misconceptions about dementia | 0.356 | |||
| Eigenvalue | 3.395 | 1.908 | 1.633 | 1.425 | ||||
| % of the variance | 14.761 | 23.056 | 30.157 | 36.355 | ||||
Note:DKAS, dementia knowledge assessment scale; PCA, principal components analysis; Si-DKAS, Sinhala version of dementia knowledge assessment scale.
We computed the reliability of the final version of the 18-item Si-DKAS. Cronbach’s alpha coefficient was 0.701. The Spearman correlation test revealed that the ITC of the current version was P ≤ 0.001; rho range, 0.249–0.574, and only two items exhibited an ITC < 0.3 (items 07 and 10). A subsample of 45 students participated in the test–retest reliability test, and the ICC was 0.953.
The discriminant validity of the scale was reflected in the differences in knowledge scores based on the academic years (Table 4). Mainly, knowledge scores for the Si-DKAS were significantly greater among students who completed the theory and clinical experience related to dementia care (third-year students) than among those who completed theory only (late second-year students) and who did not have exposure to either theory or clinical experience (early second year): χ2(2) = 86.015, P < 0.001, with mean rank knowledge scores of 236.07, 226.80, and 120.58, respectively.
Discriminant validity (N = 394).
| Variables (Kruskal–Wallis H test) | N | Total Si-DKAS | ||
|---|---|---|---|---|
| Mean rank | K-WH value | Sig. | ||
| Academic year | 86.015 | <0.001* | ||
| Early second year | 127 | 120.58 | ||
| Late second year | 57 | 226.80 | ||
| Third year | 210 | 236.07 | ||
| Preference for dementia care in future | 7.671 | 0.022* | ||
| Preference for providing dementia care | 217 | 186.71 | ||
| No preference for providing dementia care | 28 | 174.75 | ||
| Did not decided | 149 | 217.48 | ||
Note: Si-DKAS, Sinhala version of dementia knowledge assessment scale; K-WK, Kruskal-Wallis H Test;
Statistical significances at P value <0.05.
The descriptive findings for the total scale and subscales revealed that the standardized mean scores (mean score divided by the highest possible score and then multiplied by 100) for knowledge were <60%, except for the health promotion subscale, indicating a lower knowledge of dementia. Table 5 shows the mean values and standardized mean scores for the total scale and subscales.
Total and item-level scores (N = 394).
| Scale or subscale/score | Mean of the scale | Standardized mean score/100 (%) | Cronbach’s alpha | |
|---|---|---|---|---|
| Mean | SD | |||
| Total Si-DKAS/36 | 19.81 | 6.07 | 55.02 | 0.701 |
| Care consideration/14 | 7.78 | 3.08 | 55.57 | 0.631 |
| Causes of dementia/8 | 4.01 | 2.38 | 50.15 | 0.598 |
| Health promotion/6 | 3.73 | 1.67 | 62.10 | 0.347 |
| Misconceptions about dementia/8 | 4.28 | 2.11 | 53.50 | 0.487 |
Note: Si-DKAS, Sinhala Version of Dementia Knowledge Assessment Scale.
The purpose of this study was to translate, cross-culturally adapt, and assess the psychometric properties of the English version of the 25-item DKAS to Sinhala version. The study resulted in an 18-item Si-DKAS. Examining the psychometric properties assured the acceptable reliability and validity of Si-DKAS among nursing students. Reliability was examined using internal consistency (Cronbach’s alpha and ITC) and stability tests (test–retest reliability). Validity was examined through content validity, face validity, and construct validity. The construct validity was assessed using EFA, CFA, and discriminant validity. This study was the first to adapt the DKAS into Sinhala and examine its psychometric properties in a sample of nursing students in Sri Lanka.
During the translation and adaptation process, several rounds of reviews were performed by experts in dementia care, nursing students, developers of the DKAS, and a language expert to affirm face validity. Their suggestions helped refine the items, ensuring they reflected the original concepts in the adapted version while maintaining brevity. The results of the CVI of the Si-DKAS confirmed the relevance and representativeness of the items used to measure the construct (knowledge of dementia). This finding was consistent with the acceptable levels of CVI in Chinese23 and Turkish versions.9
Factor analysis was performed to test the psychometric properties of the Si-DKAS for Sri Lankan nursing students, resulting in a four-factor model with 18 of the original 25 items. Adaptation and validation studies in Japan7 and Singapore21 also reported a reduction in the number of items. In contrast, the researchers who adapted the Chinese version did not remove the items with poor factor loading from the four-factor model, which also exhibited poor fit indices.23 They reported that they did not remove items, given the clinical importance of the items in measuring knowledge toward dementia.23 They argued that poor psychometric properties might indicate poor knowledge and could not be attributed to irrelevant items to measure the construct being measured.23
This study found a relatively low percentage of variance explained by a factor solution in PCA. It indicates that factors do not fully capture the underlying structure of the knowledge. Moreover, CFI and TLI were lower than the acceptable levels.31–33 It also implied that the proposed model does not correctly capture the underlying structure of the data. However, some model fit indices of the CFA were within the satisfactory level, including χ2/df ratio, SRMR, and RMSEA. Given the complexity of the construct being measured with nursing students who showed poor knowledge of dementia, it might be challenging to explain a high percentage of variance and exhibit a satisfactory model fit. Furthermore, the low variance explained, and the suboptimal model fit indices might be due to the quality of the adapted items, the educational goals of the psychiatric nursing curriculum, the impact of nursing education by the COVID-19 pandemic, and the cultural implications within the context of Sri Lanka.
The four-factor model of this study did not align perfectly with the factor model of the original version of the DKAS.22 Factors of the original version included “cause and characteristics,” “communication and behaviors,” “care considerations,” and “risks and health promotion.”22 In this study, four factors were labeled “care considerations,” “cause and characteristics of dementia,” “health promotion,” and “misconceptions about dementia” based on careful consideration of the original version of the DKAS,22 the Singaporean version,21 and a literature survey. The factors of the Singaporean version (three-factor model) included “misconceptions about dementia,” “caregiving considerations toward dementia,” and “dementia symptoms.”21
The differences in factor loading may be attributed to sample characteristics21 and knowledge level. For example, the original development study recruited a diverse international population of health professionals, students, family carers of people with dementia, and the public involved in an online dementia course.22 We recruited only nursing students with different educational levels, indicating the need to test their psychometric properties in different populations in further studies in Sri Lanka. On the contrary, the literature has reported that when factor analysis is applied in medical education instrument development, it may not always produce favorable outcomes.42
This study indicates that Si-DKAS is sensitive to individual differences in measured traits. A comparison of the Si-DKAS scores among students of different academic years revealed excellent discrimination capacity. It helped to identify differences in nursing students’ knowledge based on their theoretical knowledge and experience of caring for people with dementia. Similarly, it was reported in the literature that the DKAS was a valid and reliable scale for detecting knowledge differences and variations among different study populations and their tailored dementia education requirements.43,44
This study revealed poor knowledge of dementia among nursing students. The Japanese,7 Indonesian,20 and Chinese23 validation studies revealed that dementia knowledge scores among health professionals and students were lower than those in this study. In this study, the lowest knowledge was reported for item numbers 24 (item number 17 of the Si-DKAS = difficulty eating and drinking generally occurs in the later stages of dementia) and 7 (item number 6 of the Si-DKAS = most forms of dementia do not generally shorten a person’s life). Similarly, Japanese study participants also showed poor levels of knowledge for items 24 and 7. In contrast, the Chinese cohort reported the lowest mean score for items 13 (the sudden onset of cognitive problems is characteristic of common forms of dementia) and 6 (blood vessel disease [vascular dementia] is the most common form of dementia).23 In this study, item number 13 was removed, while students showed less knowledge of item number 6.
In summary, the DKAS can be employed as a valuable tool for assessing knowledge of dementia among nursing students. The current findings revealed that the Si-DKAS is a valid and reliable scale for measuring four dimensions of knowledge of dementia among nursing students. This version could be considered a student version of the Si-DKAS. Nursing students in Sri Lanka receive training in psychiatric nursing, which includes dementia care, to equip them for the growing need in this area. Validating the tool with nursing students would help to identify the unique requirements of their training, which would prepare future health professionals to deliver optimal nursing care for people with dementia.
Future research is indicated by utilizing different extraction methods to explore an alternative factor structure to increase the variance explained and to ensure a satisfactory model fit. The findings of the knowledge assessments indicate that nursing students’ knowledge about dementia should be improved.
This study followed a rigorous cross-cultural translation and adaptation process proposed by the World Health Organization.25 The authors validated this scale with a large sample of nursing students to identify gaps in knowledge within the context of Sri Lanka, thereby strengthening the study.
Several limitations were identified. First, the validation study was undertaken only with nursing students in a selected nursing school, and findings may not be generalized to diverse categories of other health professionals, including practicing nurses. Second, the PCA revealed a low percentage of variance explained by the extracted components, which may lead to not presenting the complete and complex structure of knowledge of dementia. Third, a few model fit indices, especially CFI and TLI, were below the generally acceptable level threshold of 0.9, indicating a suboptimal model fit. Fourth, CFA and EFA were conducted on a single sample. Fifth, the criterion validity was not measured since there was no alternative scale to measure dementia-related knowledge in the Sinhala language, adding a limitation in assessing the psychometric properties.
The study adapted a culturally appropriate, psychometrically sound scale to measure dementia knowledge. The 18-item Si-DKAS is a valid and reliable tool for assessing knowledge of dementia among nursing students in Sri Lanka. This version further supports the differentiation of knowledge about dementia among nursing students based on their experiences. Overall, students’ knowledge of dementia is poor. This study indicates the need for curriculum revision related to dementia education in nursing curricula. Regular evaluation of knowledge related to dementia care is essential for developing educational modules for nursing students. Future studies are recommended to validate the DKAS in different populations, such as nurses, doctors, occupational therapists, formal and informal carers, and the public. Refining and improving the factor model of the Si-DKAS is recommended. Adaptation and validation of the DKAS into Tamil, another official language in Sri Lanka, is suggested.