Coronavirus disease-2019 (COVID-19) is currently considered to be a systemic infection, involving multiple systems and causing chronic complications. Compared with other post-viral fatigue syndrome, coronavirus disease postinfection (post-COVID condition) symptoms have a wider range of complications and greater intensity. The most common symptoms are fever, extreme fatigue, dyspnea, memory/cognitive impairment, and anosmia/hypoosmia.1 On 13 December 2022, the Shandong Provincial Health Commission issued a notice on further optimizing the relevant policies on epidemic prevention and control in medical institutions, pointing out that nucleic acid results will no longer be examined for personnel entering all levels and types of medical institutions in the province (http://wsjkw.shandong.gov.cn). After the optimization and adjustment of COVID-19 epidemic prevention and control policy, the number of confirmed cases increased suddenly, the number of visits to medical institutions increased in a short period of time, and the work pressure of clinical medical staff increased rapidly. As a department with advanced monitoring facilities and advanced diagnosis and treatment technology, the Department of Intensive Care Unit (ICU) focuses on the treatment of all kinds of patients with severe and multisystem failure. It is the key department for patients with basic diseases such as severe pneumonia caused by COVID-19 infection.2 ICU nurses not only have to face the increasing number of critically ill patients and undertake intensive nursing work but also have to bear the infection of themselves, their colleagues, and their families. In this very special environment, nurses are under unprecedented physical and psychological pressure at work.3 Exploring the work experience of nurses at this time is of a great significance to the intervention research on the improvement of nurses’ physical and mental health. Some studies have found that the incidence of physical symptoms in nurses is very high, which is significantly higher than that of doctors (P < 0.01).4 The quality of work is affected by fever, severe fatigue, headache, and nasopharynx symptoms. However, at present, there is little research on the work experience of ICU nurses infected with COVID-19 in China, so this study interviewed the ICU nurses infected with COVID-19 to understand their work experience and provided a theoretical basis for the intervention research on improving the physical and mental health level and work efficiency of ICU nurses under the pressure of COVID-19 infection.
We conducted an explorative descriptive study using the inductive thematic analysis. This study adheres to the Consolidated Criteria for Reporting Qualitative research checklist.5
The recruitment period lasted for 2 months, from December 2022 to January 2023, and ICU nurses in the Department of Intensive Care Medicine of a tertiary grade A Hospital were selected. Based on the existing literature, the heterogeneity of survival of nurses in ICU was described,6 and we used the maximum difference sampling method to select the subjects according to sex, symptoms, length of service, and marital status. The specific criteria were as follows: (1) The nurse has had positive nucleic acid results and has been working for at least a week, and (2) the nurses who participated in the survey had informed consent and had time for our interview. The exclusion criteria were as follows: The selected nurses did not rotate or study in other departments during the investigation period.
First, we set up a research group (the members included two head nurses of intensive care department, two ICU postgraduate nurses, and one ICU nurse with working experience in isolation ward) and identified the interviewer (the interviewer who had been trained in qualitative research, and she is an ICU nurse). After reviewing the literature and discussing with the research group,7,8 it was concluded that symptoms of the novel coronavirus vary among individuals, leading to different experiences and recovery times. It is important to consider this heterogeneity when developing the interview outline. Additionally, the impact of family dynamics should be taken into account due to the rapid spread of infections. Following an initial interview with two ICU nurses utilizing the original interview outline, adjustments were made to the language of the outline to enhance respondent comprehension. The refined semi-structured interview outline is presented in Table 1.
| Research questions |
|---|
|
Before the interview, the interviewer explained the purpose and method of this study to the interviewees in advance, obtained the patient’s informed consent, and signed the informed consent form. The interview was in the form of face to face, and the interview place took place in department’s demonstration classroom. Besides, the interview time was the nurses’ rest time. During the in-depth interview, an appropriate use of questioning, repetition, response, summary, and other skills to encourage patients to express their ideas to the maximum extent, carefully observe the interviewees’ pronunciation, intonation, facial expressions, and body movements, and take notes. It is worth noting that our interviewers always maintained language neutrality throughout the interview, did not make too much judgment, and observed and recorded in an objective manner.
The data of this study were collected and analyzed at the same time. Within 48 h after the interview, the recording materials were transcribed into text word by word using “audio to text” APP, and then the two researchers listened to the recording and checked the text. The interview data were kept anonymously in the form of case number to protect the privacy of patients. After the formation of the text data, the data of the patient were timely checked, verified them, saved them as a word document, and used MAXQDA 2020 Analytics Pro (VERBI Software GmbH, Berlin, Germany) to manage and summarize the data.9 This study carries on the theme analysis according to the inductive content analysis method.10,11 The specific analysis steps are as follows: (1) carefully study the original data to obtain the overall sense; (2) according to the research purpose or research standard, determine the selection criteria of meaningful items; (3) select meaningful semantic units according to the criteria; (4) open the open coding mode to encode meaningful semantic units; (5) compare, summarize, and compress the resulting codes into the ultimate coding; and (6) repeatedly modify and verify the topic structure.
Participants received written information about the study, detailing the purpose of the study, the criteria for participation, and their right to withdraw at any time. The names or other identity information of the participants are not mentioned in the recording and analysis but are indicated by the letter “P” to ensure confidentiality. Participants signed an informed consent form before being interviewed. This study has been formally approved by the ethics committee of the investigated hospital (No: QYFY WZLL 26722).
This study analyzed the following 5 themes of the work experience of ICU nurses after COVID-19 was reinstated: (1) Stress and challenge caused by the change of work focus; (2) downsizing, overtime, taking up work with illness, and physical discomfort; (3) dedication and family debt; (4) unknown fear and helplessness; and (5) professional responsibility and sense of benefit. We made a concise graph based on the results of the interview as shown in Figure 1. The interview time was 20–50 min.
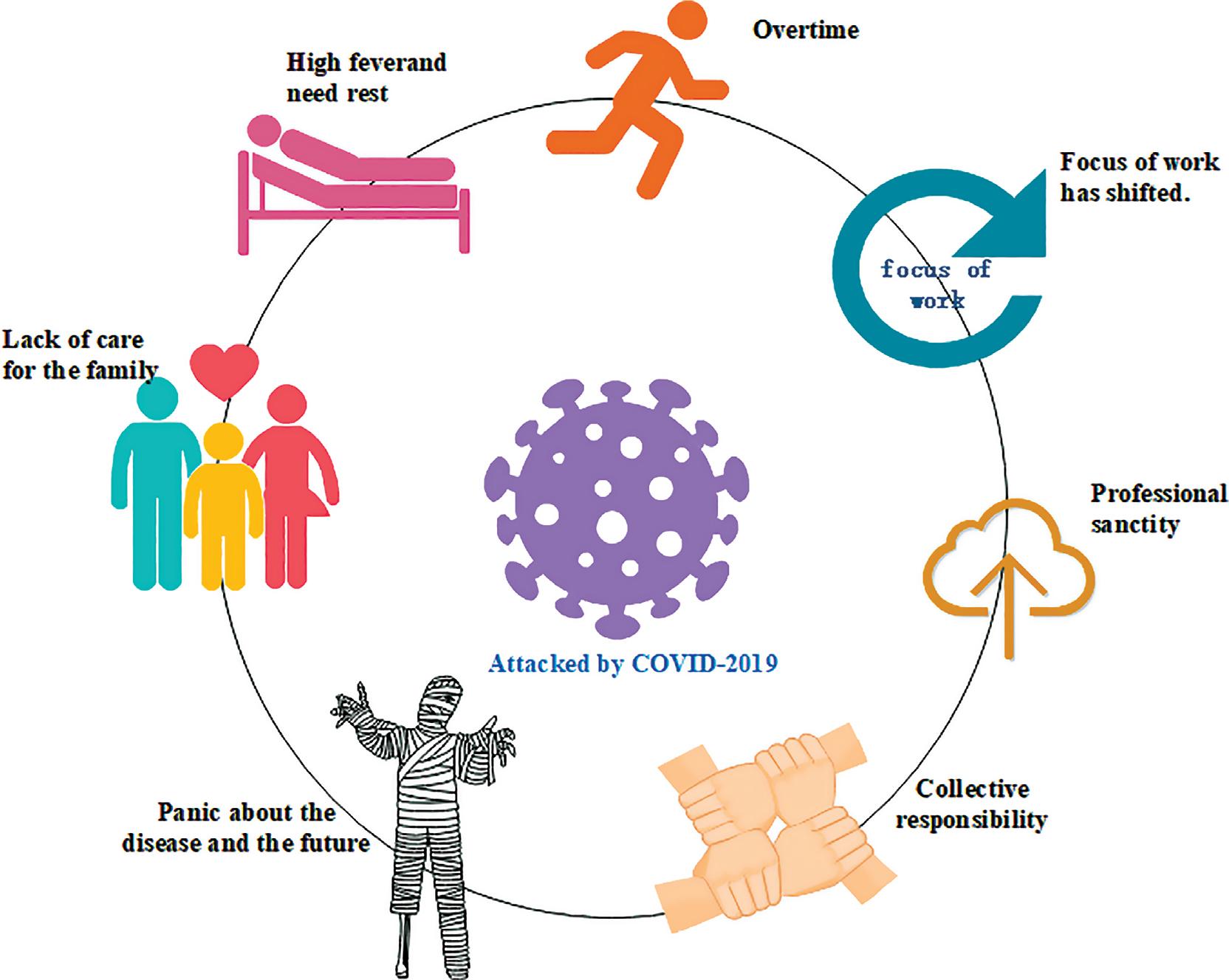
Concise graphic representation based on five themes.
Notes: Nurses attacked by COVID-19 will face three problems in their work time, one is the problem of working status (staff reduction, overtime, and the change of work focus), and the other is their own state (physical aspect: discomfort caused by disease infection, fever and other symptoms; psychological aspect: panic about disease and future). Third, the family aspect (COVID-19 is very contagious, nurses ICU often have family members who need to take care of, they will feel guilty because they conflict with the sense of dedication to group work, resulting in unable to take care of their families). It should be noted that in the course of our interview, we found some surprising things, that is, the nurses had some positive effects through this incident. for example, the sense of professional sanctity has increased (have recognized the greatness of their profession) and the sense of collective responsibility (has realized that the meaning of the collective is unity).
COVID-19 infection causes severe pneumonia, which leads to a gradual increase in the number of patients with multiple organ failure, especially in the elderly with underlying diseases, perennial bedridden, and low resistance. Then, the frequency of high intensity and difficult nursing operations such as prone position therapy and extracorporeal membrane pulmonary oxygen (ECMO) support increased. In ICU, critical patients treated with prone ventilation often receive invasive mechanical ventilation, blood purification, or extracorporeal membrane oxygen support, and need to carry important pipes such as central venous intubation and endotracheal intubation. To avoid patient discomfort and tube prolapse, they are generally given deep sedation (responsive to physical stimuli).12 In a state of deep sedation, nurses are needed to assist in turning over. Additionally, the pipeline and skin protection must be properly fixed to prevent the occurrence of nursing adverse events. Most nurses said that, recently, the focus of work has shifted to patients with severe pneumonia caused by COVID-19 infection. Elderly patients tend to have low resistance, accompanied by several basic diseases, the focus of nursing is more complex, the skin is prone to stress injury, ECMO supported patients, patients with prone position ventilation significantly increased, and work pressure increased.
“Recently, there are a lot of elderly patients, all from emergency channels. The workload and pressure of such patients are much greater than those after surgery. When admitted to the department, it is found that the patients have about 60% oxygen saturation and need endotracheal intubation, often accompanied by electrolyte disorders, septic shock and other symptoms, and may need to go through deep veins at the same time, CRRT (blood purification therapy), ECMO and so on.” (P10) “Recently, there are many elderly people, and skin problems have increased. Some patients need to report adverse events of stress injury when they are admitted to hospital. Usually, they also need us to pay more attention to and turn over frequently.” (P4)
With the increase in the number of patients with severe pneumonia, nurses was also faced with a large number of infections and attrition, resulting in an increase in the frequency of overtime for nurses and an increase in the number of nurses on duty with illness. Most of the respondents said that the workload was very heavy, they went to work with illness while the workload increased, and physical discomfort such as physical fatigue, general pain, cough, weakness, and so on brought great trouble to their work.
“A while ago, there was a real shortage of people. People around us were infected one after another, and too few people were able to go to work, which led to more overtime work, but there were no fewer patients. Going to work was like fighting a war, and more patients went to ECMO. It was really a challenge for us, because this kind of patient’s condition was unstable, and we would be very busy if we had to organize assistance and rescue under routine treatment.” (P12) “Everyone goes to work with illness and comes to work without turning overcast. In reality, they are not allowed to rest for a long time. The body does feel tired, headache, sore throat, cough, palpitations, and sometimes tinnitus. Even if you want to drink water, you have no time to go.” (P1) “I really don’t feel well. Although I came back to work without a fever, my throat was so dry that I didn’t bother to drink water when I was busy. Everyone coughed at work, it was inconvenient to spit with masks, I couldn’t speak with a sore throat, and the atmosphere at work was very depressing. I can’t turn the patient over.” (P2)
Egoism is an evolutionary instinct, derived from genes, for survival. Altruism is a product of social division of labor and education, which links others by overcoming instincts in order to make a living. The medical staff under the pressure of COVID-19 have the impact of collective dedication and difficulty in taking care of the “small family.” Interviewees said that while contributing to the collective, it was difficult to take care of the infected family members, and the family felt a clear sense of debt.
“I had a fever and rested for a few days, so I hurried back to work. Corey was so short of people. My family was positive and the baby was positive, so I had to rely on her father to take care of him. I saw the video from my father crying to his mother during the work break. I’m so sad. Her father works very hard, too. He has to take care of the child with a fever, and the child doesn’t have a good rest. When his family needs time away, he feels very indebted to them.” (P1) “I don’t have a rest. I have to keep the department running, family. I really couldn’t take care of the two children (wry smile). His father took care of them. When I went home without Yang, I didn’t dare to hold the baby. After Yang, I felt that I could finally hold the baby.” (P13) “My parents are not very well, and they are both positive, especially because my mother still has high blood pressure and coughing dizziness. She is not feeling well today and went to the health clinic to make a bottle. She really wants to ask for leave and go home. However, I understand that this is a time when there is a shortage of people, and I have a responsibility. I must sacrifice my family at this time, otherwise all departments will ask for leave, and who will take care of the patients?” (P7)
Fear, a basic emotional state, is an emotional experience that attempts to get rid of or escape from a certain situation and suffers from helplessness. COVID-19 spread is known as an “invisible enemy.”13 Some interviewees said that COVID-19 is a new virus beyond their own control and unknown, and they are afraid of its uncertain consequences. Some respondents expressed fear and concern about their own body and future nursing work, showing a significant sense of anxiety and powerlessness.
“Will there be another wave of infection in the future? When will this day end? I’m really afraid to take the kids out.” (P1) “The virus may be around us, anywhere, the patient I care for has a fever all the time, it may be on the bed, and he feels very dangerous.” (P3) “I am already healthy, but I always feel that the surrounding environment is very dangerous and may infect me again, including in the lounge, unconsciously disinfecting and panicking when I go to work.” (P9) “Recently, there are many elderly patients, many basic diseases, and a long course of disease. Now it is the peak of severe illness, and for those patients who cannot be collected, everyone has a feeling that there is no end in sight, and they do not know how long they need to be busy.” (P10) “I didn’t rest. In fact, I was scared. I was afraid that I would be tired and get myocarditis. I felt uncomfortable after Yang, including before Yang. I still felt very panicked, and the whole person was more anxious.” (P13)
Most of the respondents said that they are engaged in a special profession, and the department is a group, and a nurse’s rest often requires other nurses to sacrifice their rest time to work overtime, out of a sense of professional responsibility and teamwork spirit. When needed by the organization and patients, they must actively obey the arrangement. Some interviewees said that when they are recognized by others, including the media and the public, they will have a sense of career benefit. They often think that their efforts can benefit multiple families, which is a valuable expression, so they feel satisfied and motivated to work.
“Everyone has a very short rest time. In fact, we all understand that nurses have a responsibility on their shoulders. What we are carrying is neither money nor machines, but life and the hope of a family. For example, my symptoms are relatively serious and I have a high fever, but I am embarrassed to take more rest, because every sister in Korie is working hard and sacrificing. The number of days I rest may be overtime by others. When the temperature drops, I apply to come to work (cough).” (P8) “Seeing that there are many people speaking for medical staff on the Internet, as well as thank-you letters from some public platforms, I feel that the work is a little tired, but it is worth it. What we have done can be seen and affirmed by everyone, including the use of some sophisticated equipment. It makes me feel that our position is very meaningful and amazing.” (P12)
The results of this study showed that the number of patients with severe pneumonia caused by COVID-19 infection in the emergency department increased. These kinds of patients often had the characteristics of old age, low resistance, and many basic diseases, and the number of patients who needed prone position ventilation and ECMO support treatment increased accordingly, which were similar to the results of previous studies.14,15 Nursing work was trivial and onerous, technical requirements were high, and nurses were not feeling well, so ICU nurses were faced with unprecedented work pressure and challenges.14,15 It is suggested that nursing managers should be forward-looking in their work, do a good job in predicting and rehearsing various emergencies in peacetime, and prepare for emergencies, especially in public health emergencies, so as to improve the wartime level. In crisis nursing, according to the “3s” (personnel, material, and structure) system framework theory,16 in the face of the surge crisis (the sudden and large-scale increase in health system demand), the first task is to do a good job of personnel regulation and control. With the assistance of other parts, nursing managers can comprehensively sort out the situation of on-duty personnel in various clinical departments, reintegrate nursing human resources, and strengthen the manpower allocation of critical medical resources. In addition, the mobile nurse database is established by relying on the information system to realize the coordinated alternative personnel plan of the whole hospital.17 In the department, it is suggested that managers should do a good job in the training of relevant theoretical knowledge according to the focus of work and the training needs of nurses. In the process of training, they should pay attention to the full coverage of objects, standardization of content, and diversification of forms. Relevant guidelines, expert suggestions, and guidelines in response to COVID-19 are timely collected and distributed, training through online and offline learning models are organized, using problem-oriented teaching methods, nursing rounds are strengthened, and ensured that relevant requirements are implemented in nursing work. Fragmentation time, such as morning shift time, can be used to lead nurses to review relevant theories and knowledge points, so as to prevent nurses from suddenly facing a large number of patients with severe pneumonia, which makes it difficult to achieve holistic nursing, resulting in increased nursing pressure. Reasonable evaluation of nurses’ ability to care for patients is to ensure that nurses can effectively perform their duties.
In the rescue of public health emergencies, nurses are prone to negative emotions due to heavy work pressure and empathy for patients. If there is no strong psychological bearing capacity and do not get timely psychological intervention and support, there may be stress reactions. Related studies have shown that health-care workers facing overwork and life-threatening risks can lead to mental performance, various physical symptoms, and even serious mental illness.18,19 Cai et al.20 reported that nurses may have more opportunities to have close contact with patients infected with COVID-19 and have a higher risk of infection than other health-care professionals during the epidemic. Therefore, nurses are more likely to have physiological symptoms related to psychological stress. During the pandemic, there was a significant correlation between psychological outcomes and physical symptoms of health-care workers, and nurses often experienced depression, anxiety, insomnia and pain, which may be due to shift-induced circadian disorders, work stress, and lack of family care.21,22 To sum up, due to COVID-19 pandemic, ICU nurses faced multiple pressures and shocks and faced various psychological symptoms. Therefore, managers should pay attention to nurses’ mental health and relieve nurses’ negative emotions in time. In this special period, managers should pay attention to nurses’ work stressors and stress experience, carry out psychological intervention and stress management, and guide ICU nurses to correctly understand and relieve stress. Make every effort to do a good job in the security of front-line medical staff and their families, understand their needs from the aspects of life, psychology, humanities, and safety, provide timely material and psychological help, pay attention to the physical and mental health of medical personnel, and embody humanistic care. Pertinent psychological intervention should be given if necessary. In the future, under the condition of sufficient manpower, we will actively carry out mental health lectures and organize psychological counseling and counseling. In addition, psychological assistance can be carried out through mutual support among colleagues, such as the establishment of a Balint group.23 Nurses themselves should also improve their psychological flexibility, adjust their state in time, give themselves positive psychological cues, and look for suitable decompression methods, such as music therapy, talking, and so on. In addition, the results of this study showed that some interviewees expressed panic about the unknown nature of the disease and suggested that managers should educate nurses on disease knowledge, make correct guidance, make good protection to avoid reinfection, and set up the idea of not trusting Internet rumors. Excessive fear leads to the decline of physical resistance.
Research shows that medical workers are prone to diseases when exposed to strong pressure for a long time.24 It is suggested that department leaders face nurses’ work pressure and psychological problems during COVID-19’s pandemic and give nurses a humanistic care. Even if nurses have a sense of professional responsibility, blindly letting them make sacrifices will inevitably lead to nurses’ job burnout. In addition, studies have shown that an important reason for the psychological pain experienced by medical workers after COVID-19 infection is their long-term heavy workload.25 Common physical symptoms related to the epidemic among health workers included headache (31.9%), sore throat (30.0%), joint/muscle pain (20.6%), cough (16.9%), rhinitis (14.0%), and sputum (11.3%),18 which were similar to the results of this study. Nurses returned to nursing work after being infected with COVID-19, and the nurses had insufficient rest, heavy workload, and worried about their own safety. The relevant managers should pay attention to this and do a good job of protection and education to avoid reinfection of nurses. At the same time, enhance the frequency of communication with front-line nurses, timely evaluate nurses’ physical recovery, individualized intervention, reasonable and practical arrangement of work posts of corresponding intensity, and flexible scheduling, ensure nurses’ rest time, ensure nurses’ safety, and avoid nurses’ long-term overload. In addition, nurses are conducive to career development only when they are in a warm, loving, accepted, or protected environment,26 which suggests that managers should be fully aware of the dual identity of nurses as professionals and social people, start from multiple angles, strengthen the cultural management of on-the-job nurses, and increase the post allowance.27 Making nurses fully feel love and warmth, safety and harmony will help to improve nurses’ work enthusiasm and nursing quality.
Through in-depth interviews with 13 ICU nurses, this study revealed the real work experience of ICU nurses returning to work after being infected with COVID-19. The results showed that although the ICU nurses infected by COVID-19 had a sense of professional responsibility and a sense of benefit as their work motivation, they had multiple pressures in work, physical and psychological aspects, felt a sense of debt to their own family while contributing, and were full of worry and fear about the virus and the future work situation.