
Depression is one of the most common psychiatric disorders among people with substance use disorders (SUDs). SUD is the frequent use of alcohol or drugs (cannabis, stimulants, hallucinogens, and opioids) that causes functional or clinical impairment.1-3 Approximately half of the patients diagnosed with alcohol use disorder (AUD) have been co-diagnosed with depression.4-7 The co-occurrence of SUD and major depressive disorders is associated with a greater severity and worse prognosis than either disorder alone, including a heightened risk for suicide. 1,8-10 For instance, Lynch et al.9 found that SUDs were associated with increased suicide mortality; the adjusted odds ratios ranged from 2.0 (95% confidence interval [CI]: 1.7, 2.3) for patients with multiple SUDs, including a combination of alcohol (i.e., alcohol use disorder [AUD]), drug (i.e., drug use disorder [
Given the significant overlaps, many researchers and theories suggest that addressing the dual care needs of patients with co-occurring depression and SUD is essential to improving morbidity and mortality.11 However, in 2018, only 11% of adults with cooccurring psychiatric problems and SUDs received such integrated treatment and over 30% received no treatment at all.11,12 Therefore, we hypothesize that there is an opportunity to consider the use of alternative and complementary treatments, such as mindfulness-based interventions (MBIs), to address the existing treatment gap.
MBI is cognitive training focusing attention on experiences occurring in the present with the explicit requirement that judgment is withheld (i.e., the present is examined in the absence of judgment). With training, it has been documented those individuals can improve their well-being and mental health after MBIs.13–15 Current MBIs include a variety of forms, with different methods of delivery occurring over a range of sessions between the provider and the patient. For instance, mindfulness-based stress reduction (MBSR) was proposed by Jon Kabat-Zinn,16 which focuses on stress management strategies combined with mindfulness meditation, body awareness, and yoga to assist individuals in mindfulness. By contrast, mindfulness-based cognitive therapy (MBCT) was designed for mentally and physically ill patients to learn about the relationship between thoughts, emotions, and behaviors and then teach individuals to become more flexible, reasonable, and positive.14 Another form of MBI is mindfulness-based relapse prevention (MBRP), which is a novel approach specifically developed for substance use patients.17 The intent of MBRP is to raise awareness of triggers, monitor internal reactions, and foster more skillful behavioral choices. MBRP focuses on increasing the acceptance and tolerance of positive and negative physical, emotional, and cognitive states such as craving, thereby decreasing the need to alleviate associated discomfort by engaging in substance use.17
Several researchers reported that MBI was effective for SUD treatment and relapse prevention.18–20 For instance, a meta-analysis by Cavicchioli et al.20 found that MBIs had a small effect size (ES) to reduce overall mental health in AUD and DUD (d = 0.06, 95% CI: -0.11, 0.23, s = 5). However, Cavicchioli et al.20 included small primary studies (s = 5) and did not measure depression as an outcome. Another meta-analysis by Grant et al.21 found that MBRP had a small effect on decreasing depressive symptoms in SUD patients (SMD = -0.09 95% CI: -0.39, 0.21, s = 4). However, Grant et al.21 included only 4 primary studies and specifically examined only the effect of MBRP. With a small number of included studies, random errors frequently cause overestimation of the treatment effect.22,23 Despite these previous meta-analyses, no prior studies examined the effects of MBI on depressive symptoms among SUD patients and examined the subgroup analysis to explore the source of heterogeneity. Thus, the objective of this systematic review and meta-analysis is to examine the effects of MBIs on depressive symptoms in patients with SUD. In addition, we will examine the source of heterogeneity to explore the potential variables affecting the ES.
The Preferred Reporting Items of Systematic Reviews and Meta-Analyses (PRISMA) framework guided this systematic review by assisting in the identification, selection, and critical appraisal of the literature.24,25 PRISMA is an effective and broadly recognized tool in the standardization of the retrieval of information. For this systematic review and meta-analysis, no protocol exists.
A medical librarian-assisted literature search was performed in 8 English databases including Ovid Medline (1946+), Ovid PsycINFO (1967+), CINAHL (1937+), PubMed (1809+), Scopus (1788+), ProQuest Dissertation and Theses (1996+), Cochrane Library (1995+), and Clinical Trials (2000+). Eligible studies were identified by searching the databases for the literature collected from their inception till November 2021. We used the Medical Subject Headings (MeSH) term, and search terms are as follows: (mindfulness OR mindful* OR meditation OR meditat*) AND ((substance use disorder*) OR (substance use) OR (drug* addict*)). Truncating these terms with an asterisk allowed for plural and singular results and other related terms. Reference lists were also searched for relevant studies (ancestry studies) and previous literature reviews. Table 1 depicts an example of the search strategy used in this systematic review and meta-analysis. Figure 1 displays the flowchart of eligible studies.
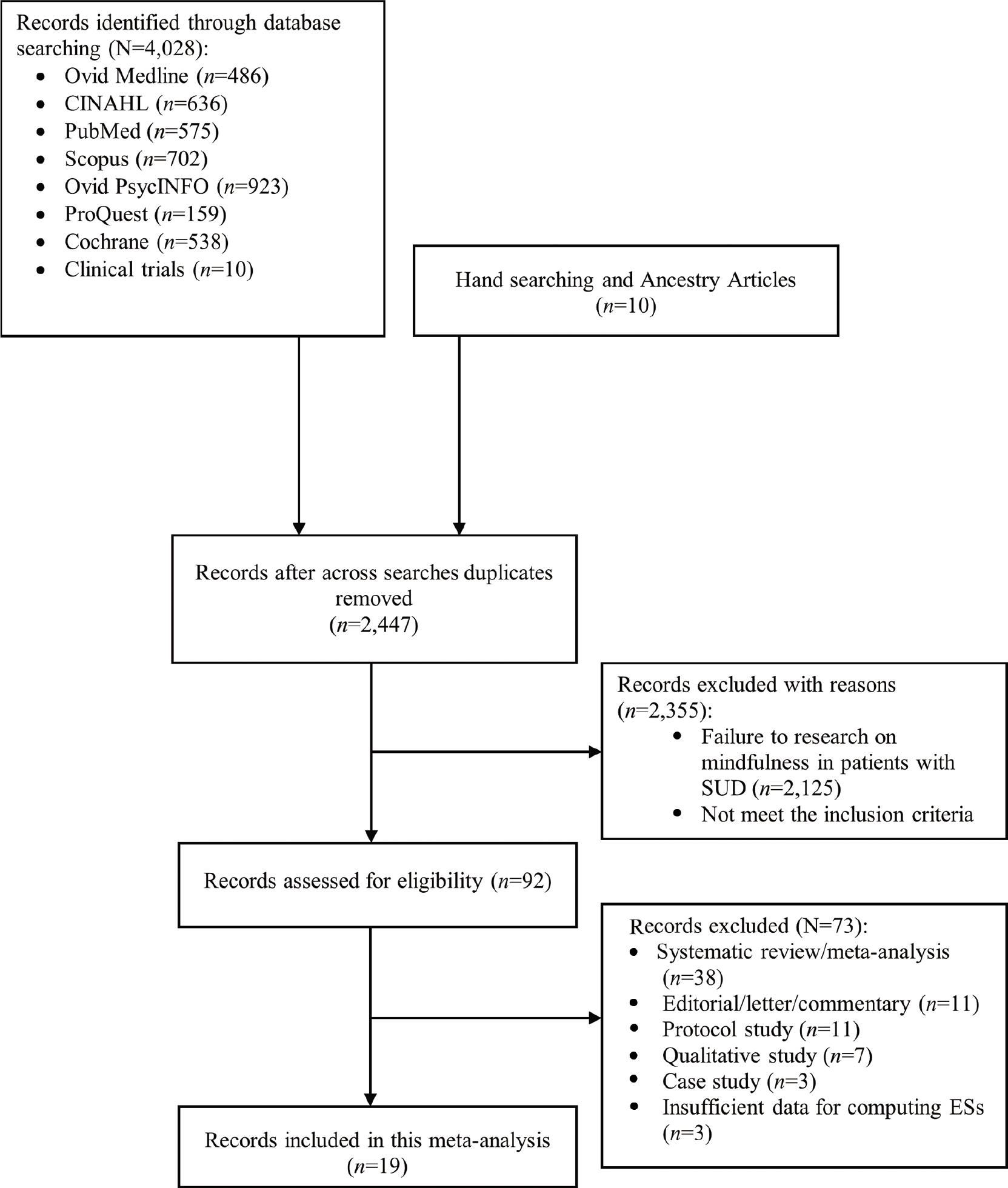
PRISMA flow of included primary studies in systematic review and meta-analysis. PRISMA, Preferred Reporting Items of Systematic Reviews and Meta-Analyses; SUD, substance use disorder.
An example of the electronic search strategy.
| No. | Searches | Results |
|---|---|---|
| 1 | Search mindfulness OR mindful* OR meditation OR meditat* | 14,861 |
| 2 | Search (“mindfulness”[Mesh])OR “meditation” [Mesh] | 5353 |
| 3 | Search ((mindfulness OR mindful* OR meditation OR meditat*)) OR ((“mindfulness”[Mesh])OR “meditation” [Mesh]) | 14,861 |
| 4 | Search (substance use disorder*) OR (substance use) OR (drug* addict*) | 91,476 |
| 5 | Search (“substance-related disorders”[Mesh] or (“substance abuse treatment centers” [Mesh] OR “substance abuse, Intervenous” [Mesh] OR “psychoses, substance-induced” [Mesh] OR “substance abuse, oral” [Mesh] OR “substance withdrawal syndrome”[Mesh]) | 276,574 |
| 6 | Search (“substance-related disorders”[Mesh] or (“substance abuse treatment centers” [Mesh] OR “substance abuse, Intervenous” [Mesh] OR “psychoses, substance-induced” [Mesh] OR “substance abuse, oral” [Mesh] OR “substance withdrawal syndrome”[Mesh]) OR ((substance use disorder*) OR (substance use) OR (drug* addict*)) | 313,986 |
| 7 | Search ((mindfulness OR mindful* OR meditation OR meditat*)) OR ((“mindfulness”[Mesh])OR “meditation” [Mesh]) AND ((((“substance-related disorders”[Mesh] or (“substance abuse treatment centers” [Mesh] OR “substance abuse, Intervenous” [Mesh] OR “psychoses, substance-induced” [Mesh] OR “substance abuse, oral” [Mesh] OR “substance withdrawal syndrome”[Mesh]) OR ((substance use disorder*) OR (substance use) OR (drug* addict*)))) | 599 |
| 8 | Search ((mindfulness OR mindful* OR meditation OR meditat*)) OR ((“mindfulness”[Mesh])OR “meditation” [Mesh]) AND ((((“substance-related disorders”[Mesh] or (“substance abuse treatment centers” [Mesh] OR “substance abuse, Intervenous” [Mesh] OR “psychoses, substance-induced” [Mesh] OR “substance abuse, oral” [Mesh] OR “substance withdrawal syndrome”[Mesh]) OR ((substance use disorder*) OR (substance use) OR (drug* addict*)))) Filters: Clinical trial | 100 |
| 9 | Search ((mindfulness OR mindful* OR meditation OR meditat*)) OR ((“mindfulness”[Mesh])OR “meditation” [Mesh]) AND ((((“substance-related disorders”[Mesh] or (“substance abuse treatment centers” [Mesh] OR “substance abuse, Intervenous” [Mesh] OR “psychoses, substance-induced” [Mesh] OR “substance abuse, oral” [Mesh] OR “substance withdrawal syndrome”[Mesh]) OR ((substance use disorder*) OR (substance use) OR (drug* addict*)))) Filters: Clinical trial; Review | 215 |
| 10 | Search ((mindfulness OR mindful* OR meditation OR meditat*)) OR ((“mindfulness”[Mesh])OR “meditation” [Mesh]) AND ((((“substance-related disorders”[Mesh] or (“substance abuse treatment centers” [Mesh] OR “substance abuse, Intervenous” [Mesh] OR “psychoses, substance-induced” [Mesh] OR “substance abuse, oral” [Mesh] OR “substance withdrawal syndrome”[Mesh]) OR ((substance use disorder*) OR (substance use) OR (drug* addict*)))) Filters: Clinical trial; Review; Publication date from 2018/01/01 to 2020/12/31 | 50 |
We included studies that (1) reported MBIs directed only at SUD patients; (2) assessed depression as a quantitative outcome; (3) included a control group to the treatment group (waitlist, usual care group); and (4) were written in English language.
We excluded studies that (1) involved MBIs plus an additional or alternative intervention that potentially affected depression (e.g., Tai Chi, qigong, transcendental meditation [TM], dialectical behavioral therapy [DBT], or acceptance and commitment therapy [ACT]), (2) lacked complete data, and (3) did not provide sufficient data for computing ES.
Two independent researchers (CR and SP) screened titles and abstracts of retrieved citations. We obtained full texts for citations judged as potentially eligible by at least one reviewer. Each reviewer independently assessed full texts against the specified eligibility criteria, and any disagreements regarding eligibility were resolved through discussion additional discussions including the author team (SB and SO).
After reviewing all eligible primary studies, we developed the codebook. Two researchers (CR and SP) revised the codebook after pilot testing with 5 studies. All researchers (CR, SP, SB, and SO) independently extracted and coded information from each study. Data from each primary study included the source of information (e.g., country, year of publication, and publication status), methods included quality of study (e.g., assignment into group, concealed allocation, blinded, intention-to-treat, power of sample, and fidelity of intervention), interventions (e.g., type of MBIs, number of session/week, and duration of each session), participant characteristics (e.g., mean age, sample size of each group, and health conditions), and outcome (e.g., depression instrument, reliability of scale, and mean and standardized depression score). As with the inclusion criteria, all discrepancies were resolved through discussion to achieve consensus.
Two researchers separately coded studies. We compared data for discrepancies. Differences in coding were discussed, and a third researcher was consulted when consensus could not be reached. When primary studies had more than two MBI groups, we coded to not duplicate participants by dividing control participants as equally as possible across comparisons. Thus, from 19 primary studies (s = 19), we coded 20 comparisons (k = 20).
We used SPSS to analyze data to describe the overall characteristics of studies. Then, meta-analysis was performed using Comprehensive Meta-Analysis version 3.0 (CMA). Because depression was measured using multiple ways across the primary studies, we used standardized mean differences of depression scores between the postintervention and control groups using Hedges’ g with 95% CIs. We used Hedges’ g because Cohen’s d has been shown to demonstrate a potential bias, which tends to overestimate the ES with small numbers of primary studies.26 We assumed the value of ESs was normally distributed with heterogeneity due to varying participant, method, intervention, and outcome characteristics. We used the random-effects model—in which CMA weights each study by the inverse of the within- and between-studies variance—to estimate the mean of the true effects. Studies with a higher precision were weighted more heavily than studies with a lower precision.26,27
We used a forest plot, Q statistic (weighted sum of squares reflecting total dispersion), and the I2 statistic (a ratio of real variability across the values of ES) to explore heterogeneity across studies. A forest plot is a graph comparing the values of ESs across studies.26 This graph visually reflects heterogeneity across studies. A significant Q statistic value indicates that heterogeneity exists. The benchmarks for I2 are 25%, 50%, and 75%, indicating low, moderate, and high heterogeneity, respectively. If an I2 value is near 100%, it means that the most observed variance is true variance.26 When heterogeneity was observed, a moderator analyses, that is, subgroup analyses based on source, participant, method, and intervention characteristics, was used to explore how these various characteristics influenced ES. A meta-analog of analysis of variance (ANOVA) was used for categorical moderators, while meta-regression was used for continuous moderators.26
Primary study quality assessment is essential for performing meta-analysis. Low-quality studies may distort the summary effect estimate.28 In this systematic review and meta-analysis, we used quality indicators as moderators and examined the difference of the values of ES for studies with and without quality indicators. Quality indicators included concealed allocation, random assignment, data collector masking, a priori power analysis, comparison of groups, and intention-to-treat analyses.28 These indicators were analyzed as dichotomous moderators, while the sample size and attrition were analyzed as continuous moderators.29,30 Table 2 lists the quality indicators for each primary study.
Quality indicators of included primary studies (n = 19).
| Author(s)/years | Assignment into groups | Concealed allocation | Masked data collector | Intention-to-treat | A priori of power | Compared groups at baseline | Baseline characteristics equal | Fidelity check | Interventionist trained |
|---|---|---|---|---|---|---|---|---|---|
| Alexander (2018)31 | 5 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| Bevan (2012)32 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
| Cooperman et al. (2021)33 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 |
| de Souza et al. (2020)44 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 |
| Glasner-Edwards et al. (2017)34 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 |
| Hosseinzadeh and Barahmand (2014)46 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 |
| Machado et al. (2020)45 | 2 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 |
| Nakamura et al. (2015)35 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | NR |
| Price et al. (2012)37 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 |
| Price et al. (2019)36 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 |
| Rogojanski et al. (2011)47 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | NR |
| Ross et al. (2019)38 | 1 | 0 | 0 | 1 | 0 | 0 | NR | 1 | NR |
| Sarvandani et al. (2021)41 | 5 | 0 | 0 | 1 | 1 | 0 | NR | 0 | NR |
| Shareh et al. (2018)42 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | NR |
| Spears et al. (2017)39 | 1 | 0 | 0 | 0 | 0 | 0 | NR | 0 | NR |
| Wongtongkam et al. (2018)49 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 |
| Yadav (2016)48 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | NR |
| Zemestani and Ottaviani (2016)43 | 5 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 |
| Zullig et al. (2021)40 | 3 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
Note: Quality indicators: 0, No; 1, Yes; ND, no dropouts; NR, not reported, except; Assignment into groups: 1, individual randomization; 2, non-randomization.
We used the funnel plot, Begg and Mazumdar rank correlation test, and Egger’s bias value for estimating publication bias. A symmetrical funnel-shaped distribution represents the absence of publication bias. A significant value of the Begg and Mazudar rank correlation test and Egger’s bias were used to suggest the presence of publication bias (one tail).29
Our searches returned 4028 studies, which were reduced to 2437 studies when duplicates were removed. A total of 10 additional ancestry studies were added. After screening the titles and abstracts of the 2447 studies, 2355 studies that did not meet inclusion criteria were removed. Of the remaining 92 primary studies, we excluded 73 studies for the following reasons: systematic review and meta-analysis (s = 38), editorial/letter/commentary document (s = 11), research without results/protocol (s = 11), qualitative study (s = 7), case study (s = 3), and insufficient information for computing ESs (s = 3). Finally, we retrieved 19 primary studies that met inclusion criteria (s = 19) (Figure 1).
The 19 primary studies that met our inclusion criteria (s = 19) reported data on 19 between-group comparison (k = 20) and 14 pre-/post-test/control group comparison. All primary studies were published between 2010 and 2021. A total of 1352 participants were included in this systematic review and meta-analysis; among them, 686 participants underwent MBIs and 578 served as controls. Ten primary studies were conducted in the United States,31-40 3 studies in Iran,41-43 two studies in Brazil,44,45 and one study in Turkey,46 Canada,47 India,48 and Thailand, respectively.49 Table 3 depicts the demographics of the 19 studies. The mean age of participant ranged from 28.4 years to 50.4 years (mean = 38.6 ± 7.0, s = 15). Female participants represented between 0 and 50.0% of the participants (mean = 24.6%). Primary researchers used 7 different depressive instruments: (1) Depression Anxiety and Stress Scale (DASS-21, s = 2), (2) Beck Depression Inventory (BDI-II, s = 9), (3) Center for Epidemiological Studies Depression (CES-D, s = 4), (4) Overall Depression Severity and Impairment Scale (ODSIS, s = 1), (5) Hamilton Depression Rating Scale (HAM-D, s = 1), (6) Hospital anxiety and Depression Scale (HAD, s = 1), and (7) Brief Symptom Inventory (BSI, s = 1). Higher scores reflect higher levels of depression. The reliability of these scales ranged from 0.66 to 0.93 (s = 8). Eleven primary studies were funded (s = 11). Nine research teams employed adapted mindfulness-based interventions (adapted MBIs), 8 employed MBRP, and one each employed MBSR. Table 4 shows more information about the intervention.
Summary demographic of included primary studies (n = 19).
| No. | Author | Study design | Samples/setting | Age mean ± SD | MMI/control Control | MMIs characteristics | F/U (month) | Measures | Results | Comments |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Alexander (2018)31, USA | Quasi | 83 SUD mothers with depression A comprehensive treatment facility | 30.5 48% <30 years. | 70/13 | - MBSR | - | BDI | At baseline: | - 92% unemployed |
| 2 | Bevan (2012)32, USA | RCT | 75 inpatients with SUD | 42 (11) | 35/40 | - A 5-d MBI training first. | 2 weeks. | DASS-21 | At 2 weeks. F/U Depression: MMI: 22.09 (11.69) to 8.40 (8.95) | - 97% white |
| 3 | Cooperman et al. (2021)33, USA | RCT | 30 people with opioid use disorder and chronic pain 2 clinics in New Jersey, USA | 50.4 (8.8) | 15/15 | Weekly as group format over 8 weeks, with 15 min. daily for home practice | 4 | CES-D | At 4 months F/U | - 53% whites |
| 4 | De Souza et al. (2021)44, Brazil | RCT | Adults with smoking Outpatient public health tobacco treatment service in Brazil | 50.0 (10.5) | 14/18 | MBRP | 4 | HAD | At 4 months F/U. | - Small sample size |
| 5 | Glasner-Edwards et al. (2017)34, USA | RCT | Stimulant dependent adults UCLA | 45.3 (8.9) | 14/12 | MBRP | 1 | BDI-II | At 1 months F/U | - Small sample size |
| 6 | Hosseinzadeh et al. (2014)46, Turkey | RCT | 35 males with drug-dependent (opium or heroin) who suffered from depression | 29.5 | 18/17 | MBCT | - | BDI-II | At posttest | - Small sample size |
| 7 | Machado et al. (2020)45, Brazil | RCT | 42 patients in SUD treatment from Outpatient clinics in city of Sao Paulo | 44 (11.2) | 10/6 | MBRP | 3 months | CES-D | At 3 months F/U | - 50%-75% attrition rate |
| 8 | Nakamura et al. (2015)35, USA | RCT | Women with SUD 89% not married/separated/divorced 100% whites At a facility in Salt Lake City, Utah | MBB: 30.4 (8.3) | 14/17 | MBB | - | CES-D | At posttest Depression | - Included only women |
| 9 | Price et al. (2012)37, USA | RCT | Women with SUD | 39 | 31/15 | MABT | 9 | BSI | At 9 months F/U | - Small sample size |
| 10 | Price et al. (2019)36, USA | RCT | Women with SUD-Nonprofit SUD treatment facility in the NW United States | 35 | 41/54 | MABT | 12 | BDI-II | At 12 months F/U | - 75% whites |
| 11 | Rogojanski et al. (2011)47, Canada | RCT | Adults with smoking | 40.34 (12.42) | 31/30 | Mindfulness intervention | 7d | DASS-21 | At 7 d F/U. | - The intervention was just a brief mindfulness intervention for coping with smoking urges |
| 12 | Ross et al. (2020)38, USA | RCT | Adults with SUD Two clinical sites | 38.44 (10.92) | 103/95 | MBRP | - | BDI-II | At posttest Depression MBRP = mean difference = -0.01 (0.45) | - 78% males |
| 13 | Sarvandani et al. (2021)41, Iran | Quasi | Adults with SUD Addition treatment clinics in Kerman | NR | 25/25 | MBSR | - | BDI-II | At posttest | - Small sample size |
| 14 | Shareh et al. (2018)42, Iran | RCT | 40 adolescents with methamphetamine- addicted | 28.41 | 20/20 | MBRP | - | BDI-II | At posttest | - No F/U |
| 15 | Spears, et al. (2017)39, USA | RCT | Adults with smoking | > 18 years | 154/103 | MBAT | - | CESD | - MBAT vs. Usual care Depression -.18[-0.40, 0.03], P = 0.099 | - 48% African American |
| 16 | Wongtongkam et al. (2018)49, Thailand | RCT | Adults with alcohol dependence Rehabilitation center, Thailand | 40.22 (8.74) | 23/15 | Vipassana mindfulness meditation | - | BDI-21 | At posttest: Depression: MMI: 16.04 (6.53) to 13.86 (9.18) | - 100% males |
| 17 | Yadav (2016)48, India | RCT | Patients with AUD All males | 35.67 (7.75) | 15/15 | Body scan meditation | - | HAM-D | HDRS: MMI: 3.0 (1.51) to 2.0 (1.61) | - 100% males |
| 18 | Zemestani and Ottaviani (2016)43, Iran | RCT | 74 adults with SUD At the treatment community center in Ahvaz, Iran | 30.1 (9.7) | 37/37 | MBRP | 2 | BDI-II | At 2 months F/U | - 80% males |
| 19 | Zullig et al. (2021)40, USA | Qua-si | Patients receiving MOUD | 36.3 (NR) | 45/35 | MBRP | 4 months | ODSIS | Depression score was different compared control group. (F = 5.94, P < 0.0001) | - 27% attrition rate |
Note1. AUD, alcohol use disorder; BDI-II, Beck Depression Inventory; BSI, Brief Symptom Inventory; CES-D, Center for Epidemiological Studies Depression; DASS-21, Depression Anxiety and Stress Scales;
HAD, Hospital Anxiety and Depression Scale; HAM-D, Hamilton Depression Rating Scale; MABT, mindful awareness in body-oriented therapy; MBB, Mind Body Bridging; MBCT, mindfulness-based cognitive therapy; MBI, mindfulness-based intervention; MBRR mindfulness-based relapse prevention; MBSR, mindfulness-based stress reduction; MOUD, medication for opioid use disorder, NR, not reported; ODSIS, Overall Depression Severity and Impairment Scale; SUD, substance use disorder; HE, Health education; MM, Mindfulness Meditation; MMI, Mindfulness Meditation Intervention; NANO, An Apple iPod Nano; NW, Northwestern; RCT, Randomized Controlled Trial; SMD, Standard Mean Difference; SES, Socioeconomic status; HDRS, Hamilton Depression Rating scale.
Characteristics of primary studies.
| Characteristic | n | Min | Q1 | Mdn. | Q3 | Max | Mean | SD |
|---|---|---|---|---|---|---|---|---|
| Mean age (years) | 15 | 28.4 | 32.4 | 38.4 | 44.0 | 50.4 | 38.6 | 7.0 |
| Total sample size at analysis | ||||||||
| MBI group | 19 | 10.0 | 15.0 | 23.0 | 37.0 | 154.0 | 36.1 | 36.4 |
| Control group | 19 | 6.0 | 15.0 | 18.0 | 37.0 | 103.0 | 30.4 | 26.9 |
| Female | 8 | 0 | 0 | 29.9 | 43.7 | 50.0 | 24.6 | 22.3 |
| White | 6 | 0 | 27.5 | 72.9 | 97.0 | 100.0 | 63.1 | 38.3 |
| African American | 4 | 0 | 0.3 | 16.1 | 47.7 | 53.3 | 21.4 | 25.6 |
| Asian | 4 | 0 | 0.3 | 1.2 | 75.3 | 100.0 | 25.6 | 49.6 |
| Weeks of structured MBI | 19 | 1.0 | 5.0 | 8.0 | 8.0 | 48.0 | 8.8 | 10.0 |
| Days across intervention (length) | 19 | 5.0 | 28.0 | 49.0 | 49.0 | 322.0 | 55.4 | 67.7 |
| Structured MBI session/week | 19 | 1.0 | 1.0 | 1.0 | 2.0 | 7.0 | 2.0 | 2.0 |
| Structured MBI min./session | 16 | 20.0 | 63.8 | 120.0 | 120.0 | 120.0 | 95.0 | 33.3 |
| Dose (length × duration) | 16 | 100.0 | 2178.8 | 5880.0 | 5880.0 | 19,320.0 | 5306.9 | 4514.8 |
| Days after intervention measured | ||||||||
| Attrition, MBI group | 18 | 0 | 0 | 19.3 | 54.6 | 59.1 | 23.1 | 24.4 |
| Attrition, control group | 18 | 0 | 0 | 8.1 | 31.2 | 70.0 | 19.6 | 24.9 |
Note: Max, maximum; MBI, mindfulness-based intervention; Mdn, median; Min, minimum; Q1, first quartile; Q3, third quartile.
Overall, MBIs had moderate ES to reduce depressive symptoms in patients with SUD (g = 0.67, 95% CI: 0.29, 1.05, I = 89%). Figure 2 displays the forest plot of individual studies; 12 primary studies showed significant values of ES. MBIs grouped into pre-/post-comparisons demonstrated significant reduction in depressive symptom, with a value of ES of.95 for correlated (r = 0.8), and g was 0.90 for uncorrelated groups. The value of ES with the control group showed improvement of depressive symptoms, with a value of 0.28 for correlated (r = 0.8), and g was 0.29 for uncorrelated groups, which suggests that spontaneous recovery of depression was likely to exist. Table 5 depicts the ES of MBI versus control comparisons.
ES of MBI vs control groups.
| Comparison | MM group | |||||||
|---|---|---|---|---|---|---|---|---|
| k | ES | P (ES) | 95% CI | SE | I2 | Q | p (Q) | |
| MBI vs. control groups | 19 | 0.67 | 0.001 | 0.29, 1.05 | 0.19 | 89.59 | 172.87 | <0.001 |
| Single group MBI | ||||||||
| Pre- vs. post- (r = 0.0) | 14 | 0.90 | <0.001 | 0.51, 1.29 | 0.20 | 75.44 | 52.94 | <0.001 |
| Pre- vs. post- (r = 0.8) | 14 | 0.95 | <0.001 | 0.59, 1.30 | 0.18 | 94.42 | 232.98 | <0.001 |
| Control group | ||||||||
| Pre- vs. post- (r = 0.0) | 14 | 0.29 | 0.036 | 0.02, 0.56 | 0.14 | 61.47 | 33.74 | 0.001 |
| Pre- vs. post- (r = 0.8) | 14 | 0.28 | 0.025 | 0.04, 0.52 | 0.12 | 90.81 | 141.41 | <0.001 |
Note: CI, confidence interval; ES, effect size; MBI; mindfulness-based intervention; SE, standard error.
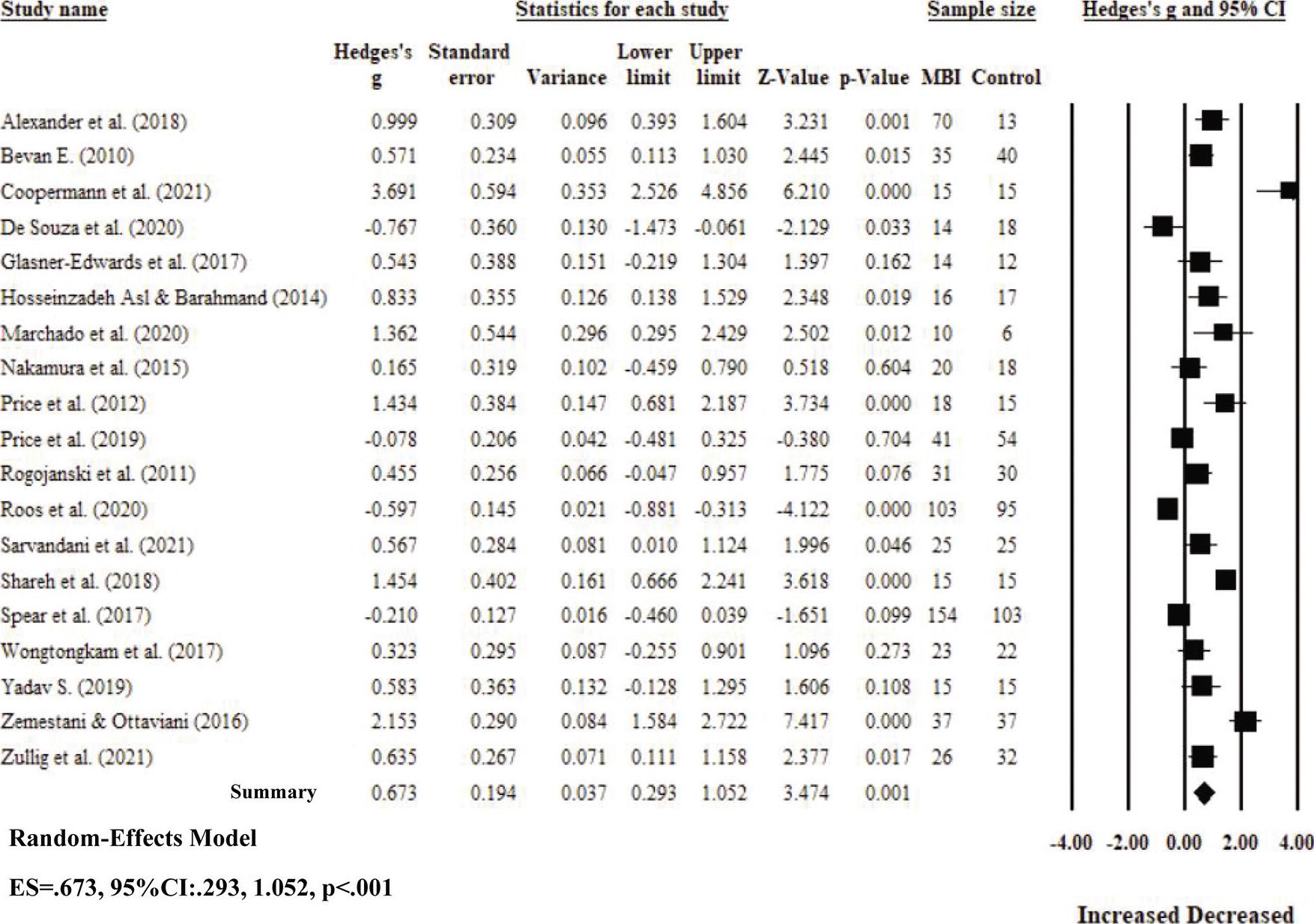
Effect of MBI on depressive symptoms in patients with SUD.
Note: ES, effect size; SUD, substance use disorder; CI, confidence interval; MBI, mindfulness-based intervention.
After we found moderate heterogeneity (I2 = 89%), we conducted subgroup analyses. Only one moderator significantly influenced ES: providing a MBI using a mixed format (i.e., individual plus group intervention) had a greater effect (g = 2.13) on reducing depressive symptoms in patients with SUD than providing MBI as a group intervention (g = 0.64) or an individual intervention (g = 0.33, P = 0.034). Recruiting participants using concealed allocation tended to reduce depressive symptoms (g = 1.22) as compared to not using concealed allocation (g = 0.48, P = 0.086). No other quality indicators—such as blinded data collection, intention-to-treat, and fidelity of intervention—were demonstrated to have a moderating influence on the value of the ES. Tables 6 and 7 show subgroup analyses.
Categorical moderator results for depression comparing MBI versus control groups.
| Moderator | k | ES | SE | Var. | 95% CI | Z | p(Z) | Qbet | P (Qbet) |
|---|---|---|---|---|---|---|---|---|---|
| Source characteristics | |||||||||
| Funding | 0.033 | 0.856 | |||||||
| Unfunded | 8 | 0.725 | 0.294 | 0.087 | 0.148, 1.301 | 2.463 | 0.014 | ||
| Funded | 11 | 0.654 | 0.254 | 0.065 | 0.156, 1.153 | 2.573 | 0.010 | ||
| Type of publication | 0.036 | 0.982 | |||||||
| Journal article | 16 | 0.683 | 0.221 | 0.049 | 0.025, 1.116 | 3.096 | 0.002 | ||
| Dissertation | 2 | 0.787 | 0.608 | 0.369 | -0.404, 1.977 | 1.295 | 0.195 | ||
| Thesis | 1 | 0.600 | 0.895 | 0.802 | -1.155, 2.354 | 0.670 | 0.503 | ||
| Method characteristics | |||||||||
| Blinded data collection | 0.349 | 0.554 | |||||||
| No | 17 | 0.634 | 0.210 | 0.044 | 0.222, 1.045 | 3.021 | 0.003 | ||
| Yes | 2 | 1.004 | 0.590 | 0.348 | -0.153, 2.160 | 1.701 | 0.089 | ||
| Intention-to-treat | 1.066 | 0.302 | |||||||
| No | 8 | 0.437 | 0.311 | 0.097 | -0.173, 1.046 | 1.403 | 0.161 | ||
| Yes | 11 | 0.863 | 0.271 | 0.073 | 0.332, 1.393 | 3.185 | 0.001 | ||
| Concealed allocation | 2.946 | 0.086 | |||||||
| No | 14 | 0.478 | 0.220 | 0.048 | 0.047, 0.909 | 2.174 | 0.030 | ||
| Yes | 5 | 1.221 | 0.373 | 0.139 | 0.490, 1.952 | 3.275 | 0.001 | ||
| Baseline characteristics equal across groups | 0.444 | 0.505 | |||||||
| No | 3 | 0.629 | 0.468 | 0.219 | -0.288, 1.545 | 1.344 | 0.179 | ||
| Yes | 12 | 0.980 | 0.245 | 0.060 | 0.500, 1.460 | 4.000 | <0.001 | ||
| Fidelity | 0.460 | 0.498 | |||||||
| No | 12 | 0.577 | 0.251 | 0.063 | 0.085, 1.069 | 2.296 | 0.022 | ||
| Yes | 7 | 0.865 | 0.342 | 0.117 | 0.195, 1.535 | 2.53 | 0.011 | ||
| Intervention characteristics | |||||||||
| MBI type | 0.100 | 0.992 | |||||||
| MBSR | 1 | 0.567 | 0.911 | 0.831 | -1.219, 2.353 | 0.622 | 0.534 | ||
| MBCT | 1 | 0.833 | 0.936 | 0.876 | -1.001,2.668 | 0.891 | 0.373 | ||
| Adapted MBI | 9 | 0.732 | 0.308 | 0.095 | 0.128, 1.337 | 2.375 | 0.018 | ||
| MBRP | 8 | 0.624 | 0.329 | 0.108 | -0.021, 1.269 | 1.896 | 0.058 | ||
| Group discussion | 0.027 | 0.869 | |||||||
| No | 6 | 0.688 | 0.343 | 0.117 | 0.017, 1.360 | 2.008 | 0.045 | ||
| Yes | 12 | 0.619 | 0.239 | 0.057 | 0.150, 1.089 | 2.587 | 0.010 | ||
| Counseling | 0.211 | 0.646 | |||||||
| No | 12 | 0.578 | 0.239 | 0.057 | 0.110, 1.046 | 2.421 | 0.015 | ||
| Yes | 6 | 0.768 | 0.338 | 0.114 | 0.106, 1.430 | 2.274 | 0.023 | ||
| Home assignment | 0.427 | 0.514 | |||||||
| No | 8 | 0.763 | 0.270 | 0.073 | 0.234, 1.293 | 2.826 | 0.005 | ||
| Yes | 10 | 0.525 | 0.246 | 0.061 | 0.042, 1.008 | 2.128 | 0.033 | ||
| Structure MBI format | 6.790 | 0.034 | |||||||
| Individual | 8 | 0.330 | 0.288 | 0.083 | -0.235, 0.895 | 1.145 | 0.252 | ||
| Group | 8 | 0.639 | 0.293 | 0.086 | 0.066, 1.213 | 2.185 | 0.029 | ||
| Mixed (individual + group) | 2 | 2.130 | 0.628 | 0.394 | 0.899, 3.361 | 3.392 | 0.001 | ||
| Outcome measure | |||||||||
| Days after intervention measured | 0.001 | 0.974 | |||||||
| Immediate post-MBI | 7 | 0.671 | 0.335 | 0.112 | 0.014, 1.328 | 2.001 | 0.045 | ||
| Delayed follow-up | 12 | 0.685 | 0.260 | 0.067 | 0.175, 1.194 | 2.635 | 0.008 | ||
Note: Adapted MBIs, adapted mindfulness-based interventions; CI, confidence interval; ES, k, number of comparisons; MBCT, mindfulness-based cognitive therapy; MBI, mindfulness-based intervention; MBRP, mindfulness-based relapse prevention; MBSR, mindfulness-based stress reduction; NR, not reported; Q, heterogeneity statistics; SE, standard error; Var., variance.
Continuous moderators of the effects of mindfulness-based intervention on depression.
| Moderator | k | Slope | SE | Tau2 | Qmodel | P-value |
|---|---|---|---|---|---|---|
| Study characteristic | ||||||
| Publication year | 19 | -0.007 | 0.062 | 0.70 | 0.01 | 0.917 |
| Sample characteristic | ||||||
| Age (mean) | 15 | -0.004 | 0.038 | 0.83 | 0.01 | 0.918 |
| Women | 7 | 0.014 | 0.022 | 1.36 | 0.41 | 0.520 |
| Method characteristic | ||||||
| Attrition | 18 | -0.004 | 0.010 | 0.76 | 0.15 | 0.703 |
| Reliability of depressive instruments | 8 | 0.337 | 2.69 | 0.32 | 0.02 | 0.900 |
| Intervention characteristics | ||||||
| Intervention length (total week) | 19 | 0.001 | 0.021 | 0.70 | 0.00 | 0.962 |
| Online MBI sessions/week | 6 | 0.036 | 0.132 | 0.44 | 0.08 | 0.783 |
| Duration of online MBI min./session | 16 | 0.001 | 0.008 | 0.86 | 0.01 | 0.922 |
| Dose (length × duration) | 16 | 0.000 | 0.000 | 0.86 | 0.01 | 0.933 |
| Days after intervention measured | 19 | -0.001 | 0.002 | 0.69 | 0.14 | 0.706 |
Note: k, number of comparisons; MBI, mindfulness-based intervention; Q, heterogeneity statistics; SE, standard error.
The result of the funnel plot was visually asymmetrical, which suggests the possibility of publication bias26,27 (Figure 3). The Begg and Mazumdar rank correlation test resulted in a Kendall’s tau of 0.391 (P = 0.009), which further suggests the existence of publication bias. In addition, the value of Egger’s regression intercept was 5.66 (95% CI: 2.98, 8.34, P< .001). While the weight of evidence strongly suggests the presence of publication bias, the small number of included primary studies indicates that caution should be used in the interpretation of the potential of publication bias.26,29
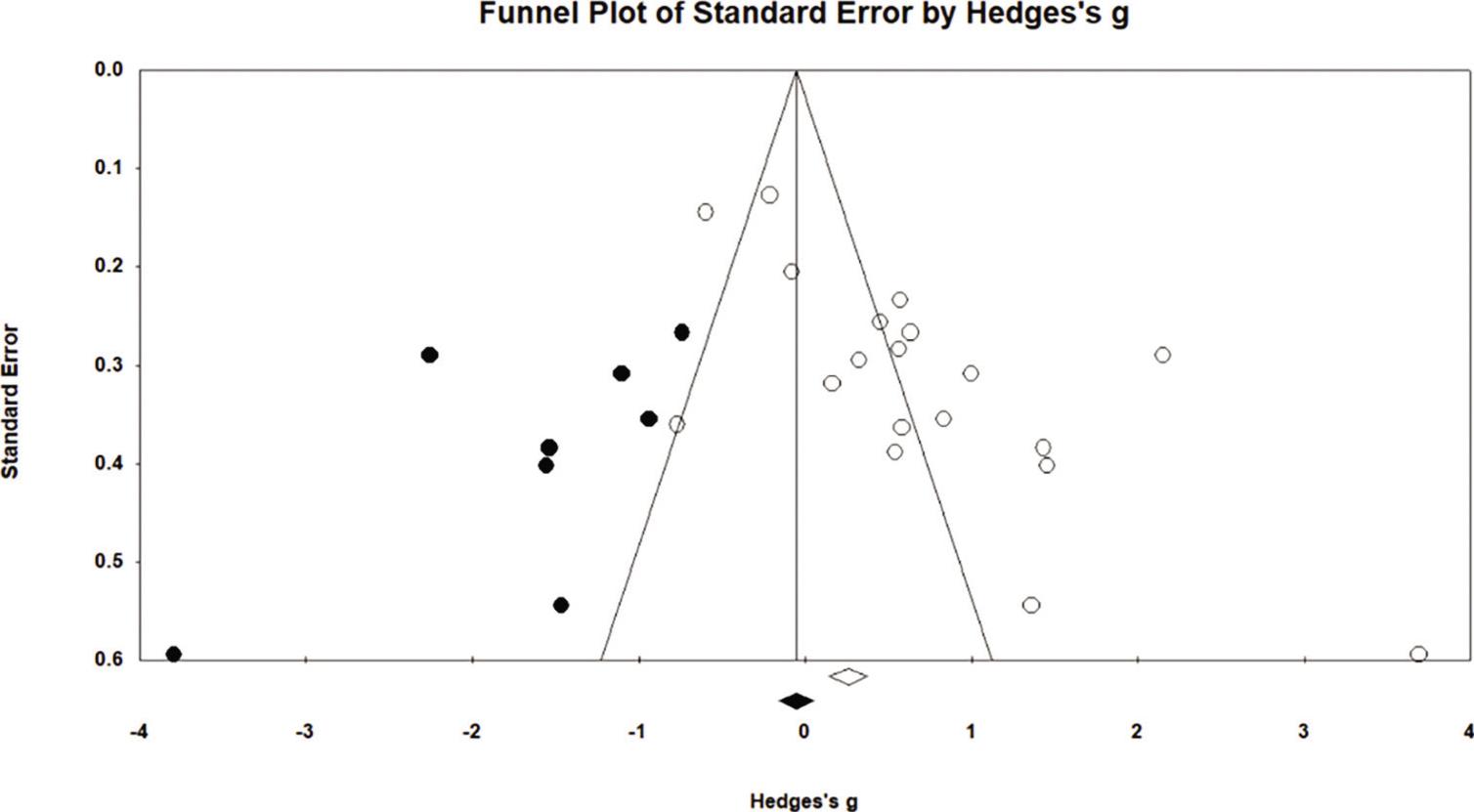
Funnel plot.
An increasing body of evidence has demonstrated that MBIs had a moderate effect to reduce depressive symptoms (g = 0.67, 95% CI: 0.29, 1.05, I2 = 89%). We cannot compare our findings to those of previous meta-analyses because prior meta-analyses were not specific for patients with SUD13,50 and did not measure depression separately but combined depression with other psychological outcomes.20,21 Thus, this is a first systematic review and meta-analysis providing evidence exclusively on the effect of MBIs in patients with SUD. In addition, to provide maximum coverage, our meta-analysis included both randomized and non-randomized control testing, and our search window covered inception to November 2021 in each of the 7 databases we examined. Our choice of criteria reflects the growing interest in the use of MBIs to treat patients with SUD.
Moderator analyses are essential for examining heterogeneity, and they can help generate hypotheses for future research. The use of MBIs in a mixed format (i.e., using both an individual and a group format) correlated to a greater effect on reducing depressive symptoms than the use of MBI either in a group or as an individual. One possible cause for our observed correlation may be that patients with SUD experienced a greater positive change with group social support and benefits of informal peer-to-peer education arising from group discussion.51 In addition, group social support of SUD patients allows the sharing of feelings, thoughts, and personal experience with best practices for dealing with depression, which may create an authentic peer-to-peer learning environment. While mindfulness practice is described as cognitive learning, patients with SUD may benefit from an environment with less judgment, which helps patients adopt a comfortable position and pay close attention.16 With individual mindfulness practice, patients with SUD learn how to cope with repetitive or ruminative thoughts related to depression. Therefore, we speculate that providing MBIs using a mixed format might be useful, especially for patients with SUD.
Although not statistically significant, researchers who used a concealed allocation showed greater values of ES on reducing depressive symptoms in patients with SUD than in who did not use concealed allocation. One possible cause to explain the correlation we observed is that allocation concealment is the technique for ensuring that implementation of the random allocation sequence occurs without the knowledge of which patient will receive which treatment.52 This method helps minimize research and participants’ bias. Thus, this technique would provide more reliable estimates of mindfulness effectiveness.
No other quality indicators moderated the effects of MBI on depression in patients with SUD. One possible reason might be that we observed relatively little variation across primary studies with regard to reporting of quality indicators. In fact, few researchers addressed the use of quality indicators in their studies. For example, only two research teams reported that they used blinded data collection in their study, whereas 17 research teams did not use blinded data collection. We note that the imbalance in the number of individuals across subgroups can increase the risk of false-negative values of ES because of inadequate power.53
We highlight the following strengths of our systematic review and meta-analysis. First, we performed a comprehensive database search, which included both published and non-published studies in an effort to identify as many possible sources of relevant data. Second, we conducted a rigorous quality assessment, and we used the results of this assessment for moderator analyses to understand how these variables impacted the value of the ES. Third, we performed subgroup analyses to explore the source of heterogeneity, which has not been reported in prior studies.
We highlight the following weaknesses of our systematic review and meta-analysis. First, we included only primary studies written in English, which may contribute to the risk of publication bias. Second, several primary studies provided only limited information, which indicates that we only had a small number of primary studies upon which we base our analyses. Based upon what we observed in the literature, we urge future researchers to pay attention to possible influence factors (such as types of MBI, guided meditation, and gender of participants) so that the correlation between those factors and the effectiveness of MBIs on depression among patients with SUD can be evaluated.
This systematic review and meta-analysis provides evidence for the use of MBIs for patients with SUD. Specifically, nurses and health care providers might consider using the mixed format intervention, which includes both individual and group interventions. Given the value of the ES we observed, MBIs may be used as adjunctive or alternative complementary treatment to decrease depressive symptoms in patients with SUD, especially when staffing availability limits the number of health care providers. With regard to research implications, we recommend that the future researchers should consider enhanced methodological strategies—such as using concealed allocation to provide the greater reliability in the value of ES. Interestingly, we note that only a few researchers measured depressive symptoms in long-term effects of MBIs, so we would suggest that the further researcher might examine the long-term effects of MBIs on depression.
Through a systematic review and meta-analysis, we found that MBIs had moderate effects on reducing depressive symptoms in patients with SUD. Providing MBI as a mixed format (with both individual and group treatments) had a greater impact on reducing depressive symptoms than providing either individual or group intervention alone. In future, greater attention to methodological quality indicators is needed.